
Abstract
Background
Acute care surgery (ACS) services have evolved in an effort to provide 24-h surgical services for a wide array of general surgical emergencies. The formation of ACS services has been shown to improve outcomes and lead to more expeditious care. Despite the advances of ACS, the etiology and timing of patient mortality has yet to be described. We hypothesized that infectious complications occur more frequently in ACS patients that die during their hospitalization.
Methods
A retrospective review of a local ACS service (non-trauma) registry was conducted. Demographic variables, admission and discharge data, and ICD-9 codes were collected. ICD-9 codes were used to identify patients with sepsis, shock, GI perforation, peritonitis, and other hospital acquired infections (urinary tract, bloodstream, and ventilator-associated pneumonias). Univariate and multivariate logistic regression analysis was performed to model the outcome of death.
Results
1,329 patients were analyzed. 53 % were male with the mean age of 52 years and an average length of stay of 13 days. 106 (8 %) died while in the hospital. Of the patients who died, 34 (32 %) died within 7 days of admission. The majority of mortalities (56 %) occurred after hospital day 14. In ACS patients that died, there were significantly higher rates of sepsis, shock, peritonitis, urinary tract infections, and VAP. After adjustment; age, sepsis on admission, and shock on admission were associated with greater odds of death.
Conclusion
ACS patients with sepsis and shock have higher mortality rate than those patients without. The majority of ACS patient deaths occurred after hospital day 14. Further investigation and continued focus on preventing and rapidly treating infectious complications as they arise is warranted.
Similar content being viewed by others

Introduction
Acute care surgery (ACS) services continue to grow and expand as data consistently shows increased emergency department throughput [1–4], a reduction in time to the operating room [5, 6] and overall decreased hospital length of stay [7]. Perhaps more importantly, ACS teams facilitate timely resuscitation and complex surgical care of the emergency general surgery patient with deranged physiologic parameters.
Recent studies have illustrated that emergency surgery patients have a significantly higher incidence of systemic inflammatory response syndrome (SIRS) than do non-emergent general surgical patients [8]. Furthermore, investigators have shown increased mortality in emergency surgery patients with increasing levels of systemic inflammation [9]. However, the specific cause of mortality in this patient population is not well defined.
The aim of the current study is to better elucidate the cause of mortality in the ACS patient population. We hypothesized that infectious complications occur more frequently in the ACS patients that die during their hospitalization, in comparison to those that survive to discharge from the hospital.
Methods
The University of Maryland Medical Center is a large tertiary hospital in Baltimore, an urban city in the eastern United States. The Acute Care Emergency Surgery (ACES) at the medical center consists of two teams of acute care surgeons, various residents, fellows, and mid-level providers that dedicate their clinical efforts to the care of the non-trauma general surgical patient requiring acute care. In December 2009, the ACES service began prospective collection of patient data and creation of an ACES-specific patient registry. Patients cared for primarily by the ACES service or consulted on by the service are included in the data set. After obtaining institutional review board (IRB) approval, retrospective review of the prospectively collected database from the time period of its inception (12/2009) to 12/2012 was performed.
Patients cared for by the ACES service (admissions and consults) were included in the analysis. Demographic data collected from the medical record included age and sex. ICD-9 diagnosis codes were collected for admission and discharge data. These codes were entered status-post patient discharge, utilizing standard administrative criteria. Admission variables collected included the presence of sepsis, shock, gastrointestinal perforation, and/or peritonitis. In-hospital mortality, day of mortality, and hospital length of stay were additionally captured.
Patients were divided into two separate groups, those who died and those who survived to discharge. Student’s t test was used to compare continuous variables. Categorical variables were compared using Chi-squared or Fischer’s exact test, as appropriate. Univariate and multivariate regression techniques were employed to model the outcome of death. A stepwise selection technique was used, with removal of all variables with a significance level greater than 0.20 from the model. Twelve effect modification terms were considered; a statistically significant interaction between age and length of stay was found, and this variable was added to the multivariate model. Post estimation, the model was checked with residual plots, histograms, and goodness-of-fit tests (Pearson’s and Hosmer–Lemeshow). Robust standard errors were estimated. All tests were two-tailed, and a p value of <0.05 was considered statistically significant. The univariate and multivariate analyses were performed in Stata Version 12.1 (Stata Corp, College Station, TX).
Results
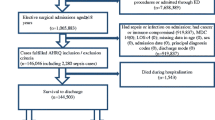
One-thousand three-hundred twenty-nine consecutive patients were seen by the ACES service over the three-year study period. The majority were male (53 %) with a mean age of 52-years. African-American and Caucasian patients were the predominant ethnic groups. The median hospital length of stay was 6 days (mean 13 days). Overall, in-hospital mortality for the group was 8 % (n = 106) and patients that died were older than those that survived. Hospital length of stay was significantly greater for patients that died (Table 1). Thirty-four patients (32 %) died within the first seven hospital days, while 13 patients (12 %) died between days 7 and 14. Fifty-six percent of deaths (n = 59) occurred after hospital day 14.
Sepsis was present on admission in 76 (72 %) of patients that died, versus 152 (12 %) of patients that survived to discharge (p < 0.001). Similarly, shock was present in 72 (68 %) patients that did not survive, versus 94 (8 %) of patients that survived (p < 0.001). Peritonitis was present on admission in 8 (6 %) of those that died in comparison to 31 (3 %) of patients that survived to discharge (p = 0.003). Perforation of the gastrointestinal tract was present in 6 % (n = 6) of patients that survived, versus 3 % (n = 33) of those that died (p = 0.08) (Table 2).
When evaluating for hospital acquired infection (HAI), urinary tract infections (UTI) were present in a significantly higher number of patients that died (24 versus 7 %, p < 0.001). Similarly, ventilator-associated pneumonia (VAP) was higher in patients with in-hospital mortality (9 versus 1 %, p < 0.001). The rate of bloodstream infection was the same between both groups (2 versus 2 %, p = 0.99) (Table 3).
Of patients that died during their hospitalization, 77 (73 %) had at least one infectious diagnosis (sepsis, shock, gastrointestinal perforation, peritonitis) on admission to the hospital. Eighty-one (76 %) of patients that died had the cumulative effect of an infectious diagnosis on presentation, plus a HAI (UTI, BSI, VAP) (Table 4).
After adjustment for multiple covariates, a statistically significant interaction between age and length of stay was detected. Age, sepsis on admission, and shock on admission were independently associated with greater odds of death. The presence of peritonitis, UTI, and any infectious complication were not associated with odds of death after adjustment (Table 5).
Discussion
In the current series; sepsis, shock, and peritonitis are more likely to be present on admission in ACS patients that proceed to die during their hospitalization. Patients that died were more likely to die after two weeks of hospitalization. Additionally, patients that proceeded to die were more likely to develop a UTI or VAP during admission, and infectious etiologies appear to be strongly associated with mortality in the ACS patient.
As acute care surgeons, influences from the care of the traumatically injured patient are inevitable, as acute care surgery inherently encompasses surgical critical care, trauma, and emergency general surgery. Trauma remains the leading cause of death in young adults aged 1–44 years and hemorrhage is the major cause of death [10, 11]. Knowledge of these facts has enabled the growth of resuscitative research and advanced the care of the traumatically injured patient. Despite these advances in the realm of trauma surgery, the etiology of death in the non-trauma ACS patient has yet to be clearly defined. In light of the current results, an infectious etiology appears to be the major contributor to non-trauma, emergent general surgery mortality and the majority of those deaths appear to happen after hospital day 14. Recognizing infection as a primary contributor to patient mortality will enable future research into optimal methods of source control, anti-microbial therapy, and resuscitative strategies specific to the ACS patient.
In the current study, consisting solely of patients cared for by an ACS team, 72 % of patients that died in the hospital had sepsis present as an admission diagnosis, versus only 12 % of those that survived. Our results are in accordance with previous research showing that patients undergoing emergent general surgical operations have SIRS present at the time of operation in 44 % of cases, versus only 7 % of patients undergoing elective general surgical procedures [8]. Researchers have also illustrated that the degree of inflammatory burden has a significant impact on patient outcomes [12–14]. Specifically examining emergent colorectal operations, Becher and colleagues showed an increased chance of death in patients presenting with sepsis and septic shock, versus those with SIRS [9]. Thus, an early hyper-inflammatory state appears to predominate in the emergency general surgery patient population and contributes to poor patient outcomes.
Secondary to scientific and procedural advances in the care of the septic patient, survival continues to increase in critically ill patients with severe sepsis [15]. Concerns regarding multi-drug resistant organisms continue to rise and pose a threat to this patient population. A recent study comparing trauma and surgical intensive care units found 31 % of first pneumonias in the trauma unit to be associated with drug-resistant organisms, versus 66 % of those in surgical intensive care units [16]. Therefore, treatment must not only be focused on source control and appropriate anti-microbial therapy, but additionally a high index of suspicion for multi-drug resistant organisms must be maintained. Currently, rapid source control and targeted anti-microbial therapy appear to be the cornerstones for treatment of the infected ACS patient.
As the field of ACS evolves, the optimal training of American ACS fellows-in-training continues to adapt in response to novel research. Given the current findings and the work of others, fellow education should include a focus on infectious diseases and anti-microbial therapy while continuing to emphasize the importance of early source control. May et al. [17] surveyed ACS program directors throughout the United States who ranked thoracic infectious, soft tissue infectious processes, abdominal infectious, biology of sepsis, and prevention of infections as their top priorities for fellow education in the field of infectious diseases. As research more clearly elucidates the predominant contributors to mortality, the collective energy of ACS can be focused on rapidly controlling the most immediate infectious threats to the patient.
Many investigators endorse the notion of regionalization of ACS resources in efforts to optimize patient outcomes [18] and have shown that patients transferred to definitive care from an outside hospital arrive with more physiologic compromise and have worse outcomes than patients not transferred [19]. In light of the current results, prompt anti-microbial therapy and source control predominate as priorities in the ACS patient population and whether this manifests as initial operation at an outside hospital prior to transfer to a higher level of care, or expedited transfer directly to definitive care, is not yet clear. However, recognition of ACS infectious pathologic entities as time-sensitive diseases should influence hospital and regional policies to expedite transfer of this patient population with the goal of prompt source control.
This work is not without its limitations. In addition to the inherent loss of granularity present with the retrospective nature of the current research, the existing registry is in its early stages of development and continues to evolve with the evolution of the clinical practice, including the addition of further metrics to assist in evaluating physiologic severity of illness. Maturation of local, nationwide, and international emergency general surgery registries will enable large-scale studies and advance knowledge with the hopes of improving patient outcomes. Additionally, this is a single-institution study performed at a large American tertiary referral center, and thus may not be applicable to other institutions. However, this work is strengthened by utilization of a dedicated ACS registry avoiding dilution inherent in more generic data sets.
This study contributes to the literature identifying infection and overwhelming inflammatory response as a contributor to ACS patient mortality. ACS patients are a unique population and infectious insult is associated with poor outcomes. Therefore, control of the infectious etiology exists as a potential target for further investigation, targeted resuscitation, and focused treatment. When present on admission; sepsis, shock, and peritonitis are much more likely in patient’s that do not survive hospitalization. These early indicators of potential mortality should alert the clinician to the possibility of an adverse outcome and serve as an area of future interventional research in improving the outcomes of non-trauma emergency general surgical patients.
References
Ball CG, Hameed SM, Brenneman FD. Acute care surgery: a new strategy for the general surgery patients left behind. Can J Surg. 2010;53(2):84–5.
Ball CG, MacLean AR, Dixon E, et al. Acute care surgery: the impact of an acute care surgery service on assessment, flow, and disposition in the emergency department. Am J Surg. 2012;203(5):578–83.
Britt RC, Weireter LJ, Britt LD. Initial implementation of an acute care surgery model: implications for timeliness of care. J Am Coll Surg. 2009;209(4):421–4.
Ciesla DJ, Cha JY, Smith JS, et al. Implementation of an acute care surgery service at an academic trauma center. Am J Surg. 2011;202(6):779–85 (discussion 785–6).
Earley AS, Pryor JP, Kim PK, et al. An acute care surgery model improves outcomes in patients with appendicitis. Ann Surg. 2006;244(4):498–504.
Britt RC, Bouchard C, Weireter LJ, et al. Impact of acute care surgery on biliary disease. J Am Coll Surg. 2010;210(5):595–601.
Cubas RF, Gomez NR, Rodriguez S, et al. Outcomes in the management of appendicitis and cholecystitis in the setting of a new acute care surgery service model: impact on timing and cost. J Am Coll Surg. 2012;215(5):715–21.
Becher RD, Hoth JJ, Miller PR, et al. A critical assessment of outcomes in emergency versus nonemergency general surgery using the american college of surgeons national surgical quality improvement program database. Am Surg. 2011;77(7):951–9.
Becher RD, Hoth JJ, Miller PR, et al. Systemic inflammation worsens outcomes in emergency surgical patients. J Trauma Acute Care Surg. 2012;72(5):1140–9.
Hess JR, Holcomb JB, Hoyt DB. Damage control resuscitation: the need for specific blood products to treat the coagulopathy of trauma. Transfusion. 2006;46(5):685–6.
Injury: The leading cause of death among persons 1–44 (Internet); (2014). Available from: http://www.cdc.gov/injury/overview/leading_cod.html. Accessed 28 Dec 2014.
Hartman KG, Bortner JD, Falk GW, et al. Modeling inflammation and oxidative stress in gastrointestinal disease development using novel organotypic culture systems. Stem Cell Res Ther. 2013;4(Suppl 1):S5.
Vitetta L, Linnane AW. Endocellular regulation by free radicals and hydrogen peroxide: key determinants of the inflammatory response. Inflammopharmacology. 2014;22(2):69–72.
Zaaqoq AM, Namas R, Almahmoud K, et al. Inducible protein-10, a potential driver of neurally controlled interleukin-10 and morbidity in human blunt trauma. Crit Care Med. 2014;42(6):1487–97.
Kaukonen KM, Bailey M, Suzuki S, et al. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand JAMA. 2014;311(13):1308–16.
Becher RD, Hoth JJ, Neff LP, et al. Multidrug-resistant pathogens and pneumonia: comparing the trauma and surgical intensive care units. Surg Infect Larchmt. 2011;12(4):267–72.
May AK, Cuschieri J, Johnson JL, et al. Determining a core curriculum in surgical infections for fellowship training in acute care surgery using the delphi technique. Surg Infect Larchmt. 2013;14(6):547–53.
Diaz JJ Jr, Norris PR, Gunter OL, et al. Does regionalization of acute care surgery decrease mortality? J Trauma. 2011;71(2):442–6.
Santry HP, Janjua S, Chang Y, et al. Interhospital transfers of acute care surgery patients: should care for nontraumatic surgical emergencies be regionalized? World J Surg. 2011;35(12):2660–7.
Conflict of interest
Brandon R Bruns declares that he has no conflict of interest, Matthew Lissauer confirms that he has no conflict of interest. Ronald Tesoriero confirms that he has no conflict of interest. Mayur Narayan confirms that he has no conflict of interest. Laura Buchanan confirms that she has no conflict of interest. Samuel M Galvagno Jr confirms that he has no conflict of interest. Jose Diaz confirms that he has no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bruns, B.R., Lissauer, M., Tesoriero, R. et al. Infectious complications and mortality in an American acute care surgical service. Eur J Trauma Emerg Surg 42, 243–247 (2016). https://doi.org/10.1007/s00068-015-0538-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-015-0538-4