
Abstract
Objective
Stabilizing sacral fragility fractures without radiation exposure to the surgical team.
Indications
Non-displaced or minimally displaced unilateral or bilateral transalar, transforaminal or central sacral fractures in weak and osteoporotic bone.
Contraindications
Displaced or highly unstable sacral fractures. Patients under therapeutic anticoagulation. Patients needing fast track orthopedic surgery.
Surgical technique
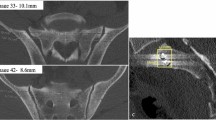
Prone position. Reference clamp installation on posterior iliac crest. Initial 3D scan of posterior pelvic ring. Image-guided virtual determination of 2–3 interforaminal iliosacroiliac trajectories in sacral vertebrae I and II. Lateral transgluteal mini-open approach. 3D image-guided insertion of 2–3 guide wires along planned trajectories. 3D-scan for controlling guide wire positions. Virtual determination of screw lengths. Cortical drilling and cannulated screw insertion along guide wires. Radiological documentation.
Follow-up
Clinical and radiological follow-up after 12 weeks, 12 and 24 months including radiographs in anteroposterior, lateral, inlet and outlet views.
Results
From October 2011 until October 2016 a total of 124 sacral fracture sites (in sacral vertebrae I and II) were treated with 120 navigated sacral screws in 52 patients (48 females, 4 males; mean age 76 ± 10 years, range 36–90 years) using 3D image guidance for screw placement. Image-guidance accuracy was 99.2% (119/120 screws correctly placed). Complications comprised revision surgery for subfascial hematoma evacuation (n = 1) and screw removal due to loosening after 12 weeks (n = 2). Four patients died before final follow-up. Mean pain visual analogue scale (VAS) decreased from 8.9 ± 1.1 (presurgery value) over 3.6 ± 1.7 (postsurgery value) to 1.8 ± 1.9 (2-year follow-up value), mean Oswestry disability index (ODI) improved from 86.2 ± 4.9% (presurgery value) over 28.5 ± 9.5% (postsurgery value) to 23.3 ± 13.7% (2-year follow-up value).
Zusammenfassung
Operationsziel
Belastungsstabile Schraubenosteosynthese nichtdislozierter Sakrumfrakturen ohne Strahlenbelastung des OP-Personals.
Indikationen
Nicht-/wenig dislozierte ein-/beidseitige und zentrale Sakrumfrakturen bei reduzierter Knochenqualität/Osteoporose.
Kontraindikationen
Dislozierte/hochgradig instabile Sakrumfrakturen. Therapeutische Antikoagulation. Kreislaufinstabilität.
Operationstechnik
Bauchlagerung. Installieren der Navigationsreferenz am hinteren Beckenkamm. 3‑D-Scan des hinteren Beckenrings. Navigierte virtuelle Festlegung von 2–3 interforaminalen iliosakralen Trajektorien im 1. und 2. Sakralwirbel. Minimal-invasiver lateraler transglutealer Zugang. Navigiertes Einbringen von 2–3 Führungsdrähten entlang der geplanten Trajektorien. 3‑D-Scan zur Kontrolle der Führungsdrahtlage. Virtuelle Schraubenlängenbestimmung. Führungsdrahtgeführtes Aufbohren der Kortikalis und Eindrehen der Schrauben. Röntgendokumentation.
Weiterbehandlung
Klinisch-radiologische Nachuntersuchungen nach 12 Wochen, 12 und 24 Monaten mit Röntgenaufnahmen in anteroposteriorem und lateralem Strahlengang sowie Inlet/Outlet-Aufnahmen.
Ergebnisse
Von Oktober 2011 bis Oktober 2016 wurden 52 Patienten (48 Frauen, 4 Männer, Durchschnittsalter 76 ± 10 [Spannweite: 36–90] Jahre) mit insgesamt 124 sakralen Frakturen (S1, S2) mittels 120 navigiert eingebrachter Schrauben versorgt. Die Schraubenplatzierungsgenauigkeit betrug 99,2 % (119/120 korrekt platzierte Schrauben). Komplikationen erforderten Revisionsoperationen bei subfaszialem Hämatom (n = 1) und Schraubenlockerung nach 12 Wochen (n = 2). Nach 2 Jahren waren 4 Patienten verstorben. Im verbliebenen Kollektiv hatte sich das Schmerzniveau von 8,9 ± 1,1 (präoperativ) auf 3,6 ± 1,7 (postoperativ) bis auf 1,8 ± 1,9 (2-Jahres-Nachuntersuchung) VAS-Punkte (visuelle Analogskala), der ODI (Oswestry-Disability-Index) von 86,2 ± 4,9 % (präoperativ) über 28,5 ± 9,5 % (postoperativ) auf 23,3 ± 13,7 % (zum 2‑Jahres-Nachuntersuchungszeitpunkt) gebessert.



















Similar content being viewed by others


References
Balling H (2018) Time demand and radiation dose in 3D-fluoroscopy-based navigation-assisted 3D-fluoroscopy-controlled pedicle screw instrumentations. Spine 43(9):E512–E519. https://doi.org/10.1097/BRS.0000000000002422
Behrendt D, Mütze M, Steinke H, Koestler M, Josten C, Böhme J (2012) Evaluation of 2D and 3D navigation for iliosacral screw fixation. Int J Comput Assist Radiol Surg 7(2):249–255. https://doi.org/10.1007/s11548-011-0652-7
van den Bosch EW, van Zwienen CM, van Vugt AB (2002) Fluoroscopic positioning of sacroiliac screws in 88 patients. J Trauma 53:44–48
Gänsslen A, Hüfner T, Krettek C (2006) Percutaneous iliosacral screw fixation of unstable pelvic injuries by conventional fluoroscopy. Oper Orthop Traumatol 18:225–244
Gardner MJ, Routt ML Jr (2011) Transiliac-transsacral screws for posterior pelvic stabilization. J Orthop Trauma 25(6):378–384. https://doi.org/10.1097/BOT.0b013e3181e47fad
German Federal Department for Radiation Control (2010) Announcement on updated diagnostic reference levels for diagnostic and interventional radiologic examinations
Lucas JF, Routt ML Jr, Eastman JG (2017) A useful preoperative planning technique for transiliac-transsacral screws. J Orthop Trauma 31(1):e25–e31. https://doi.org/10.1097/BOT.0000000000000708
Mendel T, Noser H, Wohlrab D, Stock K, Radetzki F (2011) The lateral sacral triangle—a decision support for secure transverse sacroiliac screw insertion. Injury 42:1164–1170
Richter PH, Gebhard F, Dehner C, Scola A (2016) Accuracy of computer-assisted iliosacral screw placement using a hybrid operating room. Injury 47(2):402–407. https://doi.org/10.1016/j.injury.2015.11.023
Routt ML Jr, Simonian PT, Mills WJ (1997) Iliosacral screw fixation: Early complications of the percutaneous technique. J Orthop Trauma 11:584–589
Takao M, Nishii T, Sakai T, Sugano N (2013) CT-3D-fluoroscopy matching navigation can reduce the malposition rate of iliosacral screw insertion for less-experienced surgeons. J Orthop Trauma 27(12):716–721. https://doi.org/10.1097/BOT.0b013e31828fc4a5
Thakkar SC, Thakkar RS, Sirisreetreerux N, Carrino JA, Shafiq B, Hasenboehler EA (2017) 2D versus 3D fluoroscopy-based navigation in posterior pelvic fixation: review of the literature on current technology. Int J Comput Assist Radiol Surg 12(1):69–76. https://doi.org/10.1007/s11548-016-1465-5
Tonetti J, Cazal C, Eid A, Badulescu A, Martinez T, Vouaillat H, Merloz P (2004) Neurological damage in pelvic injuries: a continuous prospective series of 50 pelvic injuries treated with an iliosacral lag screw. Rev Chir Orthop Reparatrice Appar Mot 90(2):122–131
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H. Balling declares that he has no competing interests.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 (in its most recently amended version). Informed consent was obtained from all patients included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Additional information
Editor
D. Krappinger, Innsbruck
Illustrator
R. Himmelhan, Mannheim
The device (O‑arm) is U.S. Food and Drug Administration (FDA) approved or approved by a corresponding national agency for this indication.
This research was not sponsored by an organization. The author declares that he has full control of all primary data and allows the journal to review the data if requested.
Rights and permissions
About this article

Cite this article
Balling, H. 3D image-guided surgery for fragility fractures of the sacrum. Oper Orthop Traumatol 31, 491–502 (2019). https://doi.org/10.1007/s00064-019-00629-8
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00064-019-00629-8