
Abstract
Purpose
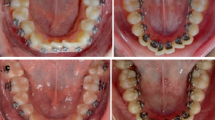
In this parallel, three-arm, single-center randomized trial, the dental and basal arch dimensions after orthodontic treatment using conventional brackets and passive and active self-ligating (SL) brackets were compared.
Methods
Patients needing comprehensive orthodontic treatment were randomly allocated to the active SL, passive SL, or conventional brackets (control) group. All patients were treated with a standardized arch wires sequence. Eligibility criteria included class I malocclusion in the permanent dentition, crowding (4–6 mm), and adequate oral hygiene. The primary outcome was intermolar width, based on cone beam computed tomography (CBCT) scans. Secondary outcomes were maxillary and mandibular widths in the canines and premolars regions, dental arch depth, buccolingual inclination, and alignment duration. Blinding of outcome assessment was implemented. Patients were followed every 4 weeks until insertion of the stainless steel 0.019 × 0.025 wire. Mean values were computed from CBCT sections, and data were analyzed using a one-way analysis of variance.
Results
In all, 66 patients (ages 18–25 years) were randomized into a 1:1:1 ratio; 7 patients dropped out before treatment initiation. Examining dental arch dimensions in the canine and premolar regions showed that expansion of the maxillary dental arch was greatest in the passive SL brackets group, less in the active SL brackets group, and lowest in the control group (P < 0.01). Changes in maxillary intermolar width between the three groups were not significant, and changes in basal arch dimensions, depth of dental and basal arches, buccolingual inclination, and alignment duration were similar in the three groups.
Conclusions
Self-ligating brackets were not more effective than conventional brackets when examining intermolar width, basal transverse dimensions, depth of the arch, and alignment duration.
Zusammenfassung
Zielsetzung
In dieser parallelen, dreiarmigen, randomisierten Studie wurden die dentalen und basalen Bogendimensionen nach kieferorthopädischer Behandlung mit konventionellen Brackets sowie passiven und aktiven selbstligierenden (SL) Brackets verglichen.
Methoden
Patienten, die eine umfassende kieferorthopädische Behandlung benötigten, wurden nach dem Zufallsprinzip der aktiven SL-, der passiven SL- oder der konventionellen Bracketgruppe (Kontrollgruppe) zugewiesen. Alle Patienten wurden mit einer standardisierten Sequenz von Bogendrähten behandelt. Zu den Zulassungskriterien gehörten eine Klasse-I-Malokklusion im bleibenden Gebiss, Engstand (4-6 mm) und eine angemessene Mundhygiene. Der primäre Endpunkt war die intermolare Breite, basierend auf DVT(digitale Volumentomographie)-Scans. Sekundäre Endpunkte waren die Ober- und Unterkieferbreite im Bereich der Eckzähne und Prämolaren, die Tiefe des Zahnbogens, die bukkolinguale Inklination und die Dauer der Nivellierung. Die Bewertung der Ergebnisse wurde verblindet durchgeführt. Die Patienten wurden alle 4 Wochen bis zum Einsetzen des Edelstahldrahtes 0,019 × 0,025 nachuntersucht. Die Mittelwerte wurden aus den DVT-Schnitten berechnet, und die Daten wurden mit einer einseitigen Varianzanalyse analysiert.
Ergebnisse
Insgesamt wurden 66 Patienten (im Alter von 18 bis 25 Jahren) in einem Verhältnis von 1:1:1 randomisiert; 7 Patienten schieden vor Beginn der Behandlung aus. Die Untersuchung der Zahnbogenmaße im Eckzahn- und Prämolarenbereich zeigte, dass die Erweiterung des Oberkieferzahnbogens in der Gruppe mit passiven SL-Brackets am größten, in der Gruppe mit aktiven SL-Brackets kleiner und in der Kontrollgruppe am geringsten war (p < 0.01). Die Veränderungen der intermolaren Breite im Oberkiefer zwischen den 3 Gruppen waren nicht signifikant, und die Veränderungen der Dimensionen des Basalbogens, der Tiefe der Zahn- und Basalbögen, der bukkolingualen Neigung und der Ausrichtungsdauer waren in den 3 Gruppen ähnlich.
Schlussfolgerungen
Selbstligierende Brackets waren bei der Untersuchung der intermolaren Breite, der transversalen Dimension, sowie der Tiefe des Kieferbogens und der Nivellierungsdauer nicht effektiver als konventionelle Brackets.


Similar content being viewed by others


References
Miles PG (2009) Self-ligating brackets in orthodontics: do they deliver what they claim? Aust Dent J 54(1):9–11
Almeida MR, Futagami C, Conti AC, Oltramari-Navarro PV, Navarro Rde L (2015) Dentoalveolar mandibular changes with self-ligating versus conventional bracket systems: a CBCT and dental cast study. Dental Press J Orthod 20(3):50–57
Atik E, Akarsu-Guven B, Kocadereli I (2018) Mandibular dental arch changes with active self-ligating brackets combined with different archwires. Niger J Clin Pract 21(5):566–572
Atik E, Akarsu-Guven B, Kocadereli I, Ciger S (2016) Evaluation of maxillary arch dimensional and inclination changes with self-ligating and conventional brackets using broad archwires. Am J Orthod Dentofacial Orthop 149(6):830–837
Atik E, Ciger S (2014) An assessment of conventional and self-ligating brackets in class I maxillary constriction patients. Angle Orthod 84(4):615–622
Atik E, Taner T (2017) Stability comparison of two different dentoalveolar expansion treatment protocols. Dental Press J Orthod 22(5):75–82
Lineberger MB, Franchi L, Cevidanes LH, Huanca Ghislanzoni LT, McNamara JA Jr (2016) Three-dimensional digital cast analysis of the effects produced by a passive self-ligating system. Eur J Orthod 38(6):609–614
Shook C, Kim SM, Burnheimer J (2016) Maxillary arch width and buccal corridor changes with Damon and conventional brackets: a retrospective analysis. Angle Orthod 86(4):655–660
Brown MW, Koroluk L, Ko CC et al (2015) Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am J Orthod Dentofacial Orthop 148(6):1067–1074
Fleming PS, DiBiase AT, Lee RT (2010) Randomized clinical trial of orthodontic treatment efficiency with self-ligating and conventional fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 137(6):738–742
Fleming PS, Lee RT, McDonald T, Pandis N, Johal A (2014) The timing of significant arch dimensional changes with fixed orthodontic appliances: data from a multicenter randomised controlled trial. J Dent 42(1):1–6
O’Dywer L, Littlewood SJ, Rahman S et al (2016) A multi-center randomized controlled trial to compare a self-ligating bracket with a conventional bracket in a UK population: part 1: treatment efficiency. Angle Orthod 86(1):142–148
Songra G, Clover M, Atack NE et al (2014) Comparative assessment of alignment efficiency and space closure of active and passive self-ligating vs conventional appliances in adolescents: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop 145(5):569–578
Stasinopoulos D, Papageorgiou SN, Kirsch F et al (2018) Failure patterns of different bracket systems and their influence on treatment duration: a retrospective cohort study. Angle Orthod 88(3):338–347
Damon DH (1998) The Damon low-friction bracket: a biologically compatible straight-wire system. J Clin Orthod 32(11):670–680
Damon DH (1998) The rationale, evolution and clinical application of the self-ligating bracket. Clin Orthod Res 1(1):52–61
Eberting JJ, Straja SR, Tuncay OC (2001) Treatment time, outcome, and patient satisfaction comparisons of Damon and conventional brackets. Clin Orthod Res 4(4):228–234
Harradine NW (2001) Self-ligating brackets and treatment efficiency. Clin Orthod Res 4(4):220–227
Berger J, Byloff FK (2001) The clinical efficiency of self-ligated brackets. J Clin Orthod 35(5):304–308
Sifakakis I, Pandis N, Makou M, Eliades T, Bourauel C (2010) A comparative assessment of the forces and moments generated at the maxillary incisors between conventional and self-ligating brackets using a reverse curve of Spee NiTi archwire. Aust Orthod J 26(2):127–133
Kim H, Kim KY, Kang YG, Kim SH, Kook YA (2006) Clinical considerations with self-ligating brackets. Korean J Orthod 36(6):474–482
Forsberg CM, Brattstrom V, Malmberg E, Nord CE (1991) Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of streptococcus mutans and lactobacilli. Eur J Orthod 13(5):416–420
Paduano S, Cioffi I, Iodice G, Rapuano A, Silva R (2008) Time efficiency of self-ligating vs conventional brackets in orthodontics: effect of appliances and ligating systems. Prog Orthod 9(2):74–80
Shivapuja PK, Berger J (1994) A comparative study of conventional ligation and self-ligation bracket systems. Am J Orthod Dentofacial Orthop 106(5):472–480
Morina E, Eliades T, Pandis N, Jager A, Bourauel C (2008) Torque expression of self-ligating brackets compared with conventional metallic, ceramic, and plastic brackets. Eur J Orthod 30(3):233–238
Suk KE, Park JH, Bayome M et al (2013) Comparison between dental and basal arch forms in normal occlusion and class III malocclusions utilizing cone-beam computed tomography. Korean J Orthod 43(1):15–22
Lundstrom A (1925) Malocclusion of the teeth regarded as a problem in connection with the apical base. Int J Orthodon Oral Sur Radiogr 11(9):793–812
Fleming PS, DiBiase AT, Sarri G, Lee RT (2009) Comparison of mandibular arch changes during alignment and leveling with 2 preadjusted edgewise appliances. Am J Orthod Dentofacial Orthop 136(3):340–347
Pandis N, Polychronopoulou A, Makou M, Eliades T (2010) Mandibular dental arch changes associated with treatment of crowding using self-ligating and conventional brackets. Eur J Orthod 32(3):248–253
Buschang PH, Stroud J, Alexander RG (1994) Differences in dental arch morphology among adult females with untreated class I and class II malocclusion. Eur J Orthod 16(1):47–52
da Silva Filho OG, Ferrari Junior FM, Okada Ozawa T (2008) Dental arch dimensions in class II division 1 malocclusions with mandibular deficiency. Angle Orthod 78(3):466–474
Al-Thomali Y, Mohamed RN, Basha S (2017) Torque expression in self-ligating orthodontic brackets and conventionally ligated brackets: a systematic review. J Clin Exp Dent 9(1):e123–e128
Acknowledgements
The trial was approved by the Scientific Research Committee of the University of Damascus.
Funding
The University of Damascus funded this project. The funders had no role in study design, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
MMA carried out the data analysis and manuscript editing. MMA, ASB, and AN participated in the data acquisition. MMA, ASB, AN, FN, and HS participated in the manuscript correction. MMA, ASB, AN, FN, and HS participated in the design of the study. MMA, ASB, AN, FN, and HS authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
M.M. Alabdullah, A.S. Burhan, A. Nabawia, F. Nawaya and H. Saltaji declare that they have no competing interests.
Ethical standards
The trial was approved by the Ethics Committee of the University of Damascus; the protocol of this trial was also registered as NCT02996292 in ClinicalTrials.gov. Written informed consent was obtained from the participants before their recruitment.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author (HS). The data are not publicly available for containing information that could compromise research participant privacy/consent.
Rights and permissions
About this article

Cite this article
Alabdullah, M.M., Burhan, A.S., Nabawia, A. et al. Comparative assessment of dental and basal arch dimensions of passive and active self-ligating versus conventional appliances. J Orofac Orthop 84 (Suppl 2), 74–83 (2023). https://doi.org/10.1007/s00056-022-00407-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-022-00407-5
Keywords
- Fixed orthodontic appliances
- Randomized clinical trial
- Self-ligating brackets
- Treatment efficacy
- Class I malocclusion