
Abstract
Background
Anal fissure is one of the most common proctological complaints. If the fissure persists for more than 6–8 weeks, it is termed a chronic fissure and will most likely need surgical intervention. Surgical partial transection of the internal sphincter muscle, lateral internal sphincterotomy (LIS), is still seen as the gold standard procedure for chronic anal fissure in many parts of the world, especially in the Anglo-American community. In contrast, the German-speaking surgical community favors fissurectomy ± application of Botox, as some studies report high postoperative incontinence rates after LIS.
Objective
This paper aims to give an overview of the literature on LIS and its outcomes and answer the question, “Is LIS still the gold standard surgical approach for chronic anal fissure?”
Material and methods
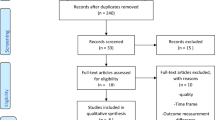
A literature search for “sphincterotomy,” “internal sphincter,” and “anal fissure” was performed in PubMed. For the purpose of this overview article, randomized controlled trials (RCTs), meta-analyses, up-to-date guidelines, and retrospective cohort studies were taken into account.
Results and conclusion
LIS produces excellent rates of fissure healing (~95%), quick symptom relief, and high patient satisfaction. Incontinence after LIS is mostly described as mild and transient. In the authors’ view, open LIS is therefore rightfully still the gold standard procedure for treatment of chronic anal fissure in the majority of patients. A conservative approach with limited division of internal sphincter muscle is preferred. For patients with preexisting sphincter weakness and an increased risk of incontinence, further preoperative diagnostic assessment (anal manometry, endoanal ultrasound) is recommended. In this high-risk group, alternative surgical options might be preferred.
Zusammenfassung
Hintergrund
Die Analfissur ist eine der häufigsten proktologischen Diagnosen. Besteht sie länger als 6–8 Wochen wird sie zur chronischen Fissur, welche in der Regel eine operative Intervention benötigt. Vor allem im englischsprachigen Raum wird die chirurgische Durchtrennung eines Teils des internen Sphinktermuskels, die laterale Internus Sphinkterotomie (LIS), nach wie vor als „Goldstandard“ in der chirurgischen Behandlung angesehen. Dies steht im Kontrast zur deutschsprachigen chirurgischen Gemeinschaft, welche der Fissurektomie ± Botoxinjektion den Vorzug gibt, da nach LIS zum Teil eine hohe Inkontinenzrate beschriebenen wird.
Ziel
Aufbereitung der aktuellen Literatur rund um LIS – ist der Status von LIS als Goldstandard-Therapie in der chronischen Analfissur nach wie vor vertretbar?
Material und Methoden
Aktuelle Literatur rund um LIS wurde in „pubmed“ identifiziert. Dabei wurden sowohl RCT, Metaanalysen, aktuelle Guidelines, sowie retrospektive Kohortenstudien berücksichtigt.
Ergebnisse und Diskussion
Die Vorteile von LIS bestehen in einer ausgezeichneten Heilungsrate (~95 %), einer prompten Symptomlinderung und dementsprechend hoher Patientenzufriedenheit. Postoperative Inkontinenz nach LIS wird meist als mild und transient beschrieben. Die Autoren vertreten daher die Meinung, dass eine offene, laterale Sphinkterotomie nach wie vor dem „Gold Standard“ der chirurgischen Fissurbehandlung entspricht. Dabei wird ein „konservativer Approach“ mit limitierter Muskeldurchtrennung bevorzugt. Bei Patienten mit Verdacht auf bereits bestehende Sphinkterschwäche werden weitergehende präoperative Abklärungen (Manometrie, endoanaler Ultraschall) empfohlen. Bei dieser „Risikogruppe“ kann ein Ausweichen auf alternative chirurgische Techniken sinnvoll sein.


Similar content being viewed by others


References
Cross KL, Massey EJ, Fowler AL, Monson JR (2008) The management of anal fissure: ACPGBI position statement. Colorectal Dis 10(Suppl3):1–7
Dykes SL, Madoff RD (2007) Benign anorectal: anal fissure. In: The ASCRS textbook of colon and rectal surgery. Springer, New York, pp 178–191
Aigner F (2008) Letter to the editor: fissurectomy for treatment of anal fissures. Dis Colon Rectum 51:1163
Nelson RL et al (2011) Operative procedures for fissure in ano. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD002199.pub4
Alonso-Coello P et al (2008) Guia de practica clinica sobre el manejo de la fisura anal. Gastroenterol Hepatol 31(10):668–681
Altomare et al (2011) The management of patients with primary chronic anal fissure: a position paper. Tech Coloproctol 15:135–141
Raulf F et al (2008) AWMF, Leitlinien der Deutschen Gesellschaft für Koloproktologie
American Society of Colon and Rectal Surgeons, Stewart D et al (2017) Clinical practice guidelines for the management of anal fissures. Dis Colon Rectum 60:7–14
Wald A et al (2014) ACG clinical guideline: management of benign anorectal disorders. Am J Gastroenterol 109:1141–1157
Eisenhammer S (1959) The evaluation of the internal anal sphincterotomy operation with special reference to anal fissure. Surg Gynecol Obstet 109:583–590
Parks AG (1967) The management of fissure in ano. Hosp Med 1:737
Notaras MJ (1969) Lateral subcutaneous sphincterotomy for anal fissure: a new technique. Proc R Soc Med 62:713
Memon AS, Siddiqui FG, Hamad A (2010) Fissurectomy with posterior midline sphincterotomy for management of chronic anal fissure. J Coll Physicians Surg Pak 20(4):229–223
Nelson RL et al (2017) A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol 21(8):605–625
Ebinger et al (2017) Operative and medical treatment of chronic anal fissures—a review and network meta-analysis of randomized controlled trials. J Gastroenterol 52:663–676
Mousavi S, Sharifi M, Mhedikha Z (2009) A comparison between the results of fissurectomy and lateral internal sphincterotomy in the surgical management of chronic anal fissure. J Gastrointest Surg 13:1279–1282
Hasse et al (2004) Lateral partial sphincter myotomy as therapy of chronic anal fissure: long term outcome of an epidemiological cohort study. Chirurg 75:160–167
Nyam DC, Pemberton JH (1999) Long-term results of lateral internal sphincterotomy for chronic anal fissure with particular reference to incidence of fecal incontinence. Dis Colon Rectum 42(10):1306–1310
Acar T et al (2019) Treatment of chronic anal fissure: is lateral open sphincterotomy a safe and adequate option? Asian J Surg 42:628–633
Vaithianathan R, Panneerselvam S (2015) Randomised Prospective Controlled Trial of Topical 2% Diltiazem Versus Lateral Internal Sphincterotomy for the Treatment of Chronic Fissure in Ano. Indian Surg 77(Suppl 3):1484–1487
Hancke E, Schwaner S (2003) Chronische Analfissur – Operative Behandlung mit Analdilatation, Exzision der Analfissur versus laterale Sphinkterotomie. coloproctology 25:95–105
Garg P, Garg M, Menon G (2013) Long-term continence disturbance after LIS for chronic anal fissure: a systematic review and meta-analysis. Colorectal Dis 15:e104–e117
Hyman N (2004) Incontinence after lateral internal sphincterotomy: a prospective study and quality of life assessment. Dis Colon Rectum 47(1):35–38
Mentes et al (2006) Results of lateral internal sphincterotomy for chronic anal fissure with particular reference to quality of life. Dis Colon Rectum 49(7):1045–1051
Elsebae M (2007) A study of fecal incontinence in patients with chronic anal fissure: prospective, randomized, controlled trial of the extent of internal anal sphincter division during lateral sphincterotomy. World J Surg 31:2052–2057
Wiley et al (2004) Open vs. closed lateral internal sphincterotomy for idiopathic fissure-in-ano: a prospective, randomized, controlled trial. Dis Colon Rectum 47(6):847–852
Rosa et al (2005) Calibrated LIS for chronic anal fissure. Tech Coloproctol 9(2):127–131
Mentes et al (2005) Extent of lateral internal sphincerotomy: up to the dentate line or up to the fissure apex. Dis Colon Rectum 48(2):365–370
Garcea G et al (2003) Results following conservative lateral sphincterotomy for the treatment of chronic anal fissures. Colorectal Dis 5(4):311–314
Alawady M, Emile S, Abdelnaby M, Elbanna H, Farid M (2018) Posterolateral versus lateral internal anal sphincterotomy in the treatment of chronic anal fissure: a randomized controlled trial. Int J Colorectal Dis 33:1461–1467
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Holzgang and D. Jayne declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Rights and permissions
About this article

Cite this article
Holzgang, M., Jayne, D. Lateral internal sphincterotomy (LIS)—still top gun in chronic anal fissure treatment?. coloproctology 42, 478–484 (2020). https://doi.org/10.1007/s00053-020-00454-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00053-020-00454-9
Keywords
- Postoperative incontinence
- Conservative sphincterotomy
- Anorectal surgery
- Fissurectomy
- Botulinum toxin injection