
Abstract
The nuclear accident that occurred at the Fukushima Daiichi Nuclear Power Plant on March 11, 2011 was caused by the extremely massive earthquake and gigantic tsunami, which resulted in a severe accident that extended over multiple reactors simultaneously. In the present chapter the current status of the accident is described in terms of basic information, sequences of the accident, fission products (FP) released, and lessons learned. Although some details of the accident are still not well known, the sequences, causes, and consequences of the accidents have been basically clarified by the efforts of several investigation committees in Japan. The fission products released to the environment were estimated by the severe accident analysis code, MELCOR, from inside the reactor core, and also by the atmospheric dispersion simulations code, SPEEDI, by coupling with environmental monitoring data in the reverse estimation method from outside the plant. The estimated release amount of 131I is of the order of 120–160 PBq and that of 137Cs is of the order of 8–15 PBq for both estimations. Lessons learned from the accident identified by the investigation committees cover a wide spectrum of insufficient measures, such as for earthquake and tsunami, station blackout, severe accident management, common cause accident at multiple unit site, education and training, chain of command at the accident, disaster prevention, and safety regulation systems. These lessons should be shared all over the world for the higher level of safety assurance of current reactors, and advanced reactors without the need of evacuation in principle should be developed for future.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The nuclear accident that occurred at the Fukushima Daiichi Nuclear Power Plant (NPP) of Tokyo Electric Power Co. (TEPCO) on March 11, 2011 was caused by an extremely massive earthquake, the Great East Japan Earthquake, and a gigantic tsunami rarely seen in history, which resulted in the severe accident that extended over multiple reactors simultaneously. Although some details of the accident are still not well known, the sequences, causes, and consequences of the accidents have been basically clarified by the efforts of investigation committees, such as Independent Investigation Commission [1], TEPCO’s Investigation Committee [2], National Diet’s Investigation Committee [3] and Government’s Investigation Committee [4]. The fission products (FPs) released to the environment were estimated by the severe accident analysis code from inside the reactor core, and also by atmospheric dispersion simulation code by coupling with environmental monitoring data in the reverse estimation method from outside the plant. Lessons learned from the accident are identified mostly by those investigation committees, which cover the wide spectrum of insufficient measures in hardware, software, management, and regulation [1–4]. In the present chapter, the current status of the accident is described in terms of basic information, sequences of the accident, estimated fission products released, and lessons learned from the accident.
2 Basic Information
The Fukushima Daiichi NPP is located in the towns of Okuma and Futaba, which are in the county of Futaba in Fukushima Prefecture. This NPP consists of six boiling water reactors (BWR) installed, Units 1 through 6, with a total generating capacity of 4,696 MWe (Table 3.1). The reactor model of Unit 1 is BWR3, that of Unit 2 through 4 is BWR4, and that of Unit 5 and 6 is BWR5. The Primary Containment Vessel (PCV) model of Unit 1 through 5 is Mark-1 and that of Unit 6 is Mark-2, respectively. Before the earthquake on March 11, Units 1 through 3 were under operation and Units 4 through 6 were undergoing periodic inspection. Unit 4 was undergoing a major construction for renovations, with all the nuclear fuel in the reactor pressure vessel (RPV) having already been transferred to the spent fuel pool. More details on the plant specifications and initial and boundary conditions are described in 2].
3 Accident Sequences
3.1 Before the Tsunami Attack
The Pacific Coast area of eastern Japan was struck off the Tohoku District by the Pacific Ocean Earthquake, which occurred at 14:46 on March 11, 2011. This earthquake occurred in an area where the Pacific plate sinks beneath the North American plate. The magnitude of the earthquake was 9.0, the greatest in Japan’s recorded history. Within seconds of the earthquake, the reactor was shut down in all three operating units with the insertion of control rods. The turbo-generators also tripped, and main steam isolation valves closed. All power supplied from a total of six external power supply lines connected to the power plant stopped as a result of damage to the breakers and collapse of the power transmission line tower caused by the earthquake. The earthquake thus disrupted the electrical supply from the grid, which resulted in a loss of offsite power for all six units. As designed, the emergency diesel generators (EDGs) started providing essential power for all safety systems, including the residual heat removal system. Up to the present time, major damage to the reactor facilities that are important for safety functions has not yet been identified [1–4].
3.2 After the Tsunami Attack
Fukushima Daiichi was hit by the first enormous tsunami at 15:27 on March 11, and the next enormous wave was around 15:35. The license for the establishment of nuclear reactors at the Fukushima Daiichi was based on the assumption that the maximum design basis tsunami height expected was 3.1 m. The assessment in 2002 based on the “Tsunami Assessment Method for Nuclear Power Plants in Japan” proposed by the Japan Society of Civil Engineers indicated a maximum water level of 5.7 m, and TEPCO raised the height of its Unit 6 seawater pump in response to this assessment. However, the height of the tsunami this time was 14 to 15 m, and all EDGs and the power panels installed in the basements of the reactor buildings and turbine buildings, except one air-cooled diesel generator for Unit 6, were inundated and stopped functioning (Table 3.2): this resulted in a station blackout (SBO) event for Units 1 through 4. All station DC powers (batteries) were also lost at Units 1, 2, and 4 because of the tsunami, but some DC power survived initially at Unit 3. The tsunami also damaged the coolant intake structures, the seawater pumps for auxiliary cooling systems, and turbine and reactor buildings, resulting in a loss of ultimate heat sink for all six units. It took 9 days to restore offsite power to the site.
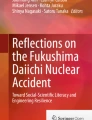
TEPCO’s operators followed their manuals for severe accidents and attempted to secure power supplies to recover equipment within the safety systems, such as core-cooling and water-injection systems, which had automatically started up. However, ultimately power supplies could not be recovered. Because the core-cooling functions using AC power were lost in Units 1 through 3, core-cooling systems without need of AC power were put into operation: the isolation condenser (IC) in Unit 1, reactor core isolation cooling system (RCIC) in Unit 2, and RCIC and high-pressure injection system (HPCI) in Unit 3. Schematics of IC and RCIC systems are shown in Figs. 3.1 and 3.2, respectively. These core-cooling systems, which do not need AC power, stopped functioning thereafter, and were switched to alternative injections of freshwater or seawater by fire-extinguishing lines, using fire engine pumps. In Units 1 through 3, because water injection to each reactor core was impossible to continue for several hours, the nuclear fuels were not covered by water but were exposed to the steam, leading to a core melt situation. It is believed that part of the melted fuel stayed at the bottom of the RPV. The main causes of the damage during the accident are illustrated in Fig. 3.3. More details on the accident sequences of Units 1 through 3 are described in the following sections [3].

Schematic diagram of isolation condenser (IC). RPV, reactor pressure vessel

Schematic diagram of reactor core isolation cooling system (RCIC)

Main causes of damages during the accident
3.3 Accident Sequence of Unit 1
For Unit 1, the emergency core cooling was provided by isolation condensers (ICs). In the primary side of the IC, steam from the main steam line is condensed and the water is returned to the RPV via the recirculation line (see Fig. 3.1). The secondary side of the IC is cooled by the plant demineralizer, with a minimum water supply for 6 h before makeup is required in the design. However, the ICs for Unit 1 ceased operation within an hour of the SBO event. Because the core cooling was lost relatively early after the SBO, the accident sequence was rather simple. It is presumed that the accident resulted in core melting, RPV failure, and core melt drop on the containment vessel floor at the shortest time of the accident sequence. With little core cooling expected in these situations, at about 2.5 h after the SBO, the core water level dropped to the upper core location as a result of overheating of the core, at about 4 h zirconium water chemical reaction heavily progressed, and at about 4.5 h core melt probably initiated. With the progression of the core melt, the core melt temperature increased above 2,500°C; rare gas and volatile fission products, such as iodine, and cesium, were vaporized from the core and were released to the vapor phase in the RPV. It is estimated that RPV failure occurred near the lower head as a result of the relocation of the core melt into the RPV lower plenum. It is estimated that this happened at about 02:45 on March 12 when RPV pressure and containment drywell (D/W) pressure became nearly the same value, as shown in Fig. 3.4; this resulted in releases of high-temperature and high-pressure steam and volatile fission products into the containment D/W from RPV. Because this released steam was much higher in temperature and pressure steam than the design temperature and pressure of the containment vessel, gaskets at the flanges, hatches, airlocks, and penetrations of the containment were degraded, resulting in the loss of leak-tightness of the containment. Hydrogen explosions at Unit 1 and Unit 3 indicate that a large amount of hydrogen along with FPs and steam was released into the reactor building from the containment vessel. FPs released into the reactor building were considered to be released to the environment mostly as a result of the hydrogen explosion.

Accident sequence of Unit 1
It is estimated that the most of the core melt dropped on the containment floor at about 04:00 on March 12, and molten core–concrete interaction (MCCI) occurred by abrading the concrete of the containment floor underneath. However, the molten core was finally cooled by the injected cooling water during the accident. It is still quite unknown where and in what state the core debris exists in the containment.
As shown in Fig. 3.4, the pressure of D/W after about 01:00 on March 12 was more than 0.7 MPa, which is much higher than the design pressure of the containment, and this was the critical situation for the containment integrity. At about 14:30 the operators successfully conducted containment suppression chamber (S/C) venting under the poor working conditions. This effort caused drastic decrease of D/W pressure, and containment rupture at the initial stage of the accident could be avoided. However, more than 13 h was required to actually conduct S/C venting. This large delay in S/C venting is one of the reasons that hydrogen explosion and FP release to the environment could not be prevented. Because the pressure of RPV decreased to about 0.8 MPa at about 02:45 on March 12, it was possible to inject water into the RPV by using fire engines. However, it took some more time for preparing the water injection because of the equipment damages and chaos caused by the earthquake and tsunami. The water injection was actually conducted at 05:46 on March 12. The water injection rate was not adequate, only about 1 t/h until about 07:00. However, it is estimated that if this water had not been injected, the core melt would probably have abraded through the containment vessel bottom and the core melt might directly interact with groundwater.
3.4 Accident Sequence of Unit 2
After the SBO, RCIC of Unit 2 was functioning. However, until about 10:00 on March 14, more than 3 h earlier than the RCIC stop time, the water level of the RPV was decreasing and the pressure of RPV was increasing. It is believed that this trend shows that RCIC was losing its core-cooling capability. At the central control room, operators tried to rapidly depressurize RPV by opening the safety relief valves, and it was only possible after 5 to 6 h because of the delay for preparing batteries. The reason of this delay was the immediate chaos caused by the hydrogen explosion at Unit 3, resulting in much time needed to prepare the large amount of batteries. When the depressurization was initiated by opening the safety valves, the RPV water level was almost half of the core. The water level then reached to the bottom of the core, resulting in the loss of water in the core region.
As shown in Fig. 3.5, the increase of D/W pressure initiated after about 19:00 on March 14, and it showed almost the same value as the RPV pressure, which indicates the occurrence of the RPV failure. After the RPV pressure and D/W pressure increased with values similar to each other, they remained at the high values of 0.6 to 0.7 MPa for more than 7 h, which is much higher than the design pressure (0.427 MPa). Around this time, FPs in the RPV were released into D/W, which is indicated by the rapidly increased dose rate in D/W (Fig. 3.5). Through the flanges, hatches, airlocks, and penetrations with gaskets degraded by the high temperature and high pressure of the containment, hydrogen and volatile fission products, such as iodine, and cesium, were released to the reactor building, a similar phenomenon as the hydrogen explosion process in Units 1 and 3. It is believed that the opening of the blowout panel on the roof of the reactor building caused by the impact of the hydrogen explosion of Unit 3 prevented the occurrence of the hydrogen explosion of Unit 2.

Accident sequence of Unit 2
The pressures of D/W and RPV both rapidly decreased from 0.65 MPa from about 07:00 to 11:00 on March 15. Especially, the pressure of D/W decreased to atmospheric pressure. This rapid decrease indicates that a relatively large failure occurred in D/W. It is therefore shows that a large amount of gases including a high level of radioactive materials in D/W was released into the reactor building in a short period because of the loss of containment leak-tightness. Also, sharp synchronized peaks were observed for both RPV and D/W pressures after the immediate decrease of D/W pressure. RPV pressure decreased and then rapidly increased to 0.65 MPa, which is almost before the rapid decrease, and then it rapidly decreased. The peak value of D/W pressure is about half of the RPV pressure spike, but they are almost synchronized and the shape is similar. This rapid increase and decrease of RPV pressure shows that the large amount of steam was generated in a very short period in RPV, and it was released to the D/W side and then released to reactor building through failure location of D/W. It is considered that the large amount of steam generated was the result of direct contact of core melt relocated to the lower plenum of RPV with the remaining water there. It is assumed that a new rupture of relatively large size was formed at the lower head of the RPV. It should be noted that containment venting was tried three times to depressurize the containment, but all attempts were unsuccessful.
3.5 Accident Sequence of Unit 3
In Unit 3, RCIC was operated using surviving DC power at 16:03 on March 11 after SBO. This RCIC was stopped at 11:36 on March 12. HPCI was automatically activated by the signal of “RPV low water level” at 12:35 on March 12. After the HPCI operation the PRV pressure, which once reached about 7.5 MPa, decreased to 4.8 MPa at 12:05, and 3.5 MPa at 14:25, 0.8 MPa at about 20:00, and 0.58 MPa at 2:42 on March 13 when HPCI was stopped (Fig. 3.6). The RPV pressure increased again to 4.0 MPa at 1 h and 7.38 MPa at 2 h after HPCI stopped. The RPV pressure rapidly decreased from 7.3 to 0.46 MPa at 8:55 on March 13 from opening of safety relief valves. At the same time, D/W pressure rapidly increased to 0.537 MPa, which is nearly the same as the RPV pressure, because of the inflow of high-temperature and high-pressure coolant. Because the D/W pressure was higher than the design pressure of the containment, 0.427 MPa, containment S/C venting was immediately conducted. D/W pressure decreased rapidly, but the opening of the venting was unstable and the opening began closing in a short time. Opening and closing of the venting were thus iterated five times. During this period RPV pressure and D/W pressure rapidly increased and decreased. Rapid increase of RPV pressure indicates a large amount of steam generation, which implies the existence of the core melt. The rapid decrease of both RPV pressure and D/W pressure clearly indicates the effectiveness of the S/C containment venting for the depressurization of the containment. In contrast to Unit 2, the containment pressure of Unit 3 did not remain above 0.6 MPa for a long time because of the multiple depressurizations. Just after the fourth venting at 11:01 on March 14, the hydrogen explosion occurred at the reactor building. This explosion indicates that a large amount of hydrogen along with radioactive materials and steam was released to the reactor building, and the radioactive materials were released to the environment.

Accident sequence of Unit 3
3.6 Spent Fuel Pools
In Unit 4, all core fuels had been transferred to the spent fuel pool for periodic inspection before the earthquake. The urgent task at the site, along with recovery of the power supply and the continuation of water injection into reactor vessels, was injection of water into the spent fuel pools. In the spent fuel pool in each unit, the water level continued to drop because of evaporation of the water caused by the heat of the spent fuel in the absence of the pool water cooling caused by the loss of power supply. Water injection to the spent fuel pool was conducted by the Self-Defense Forces, the Fire and Disaster Management Agency, and the National Police Agency, using helicopters and water cannon trucks. Concrete pump trucks were ultimately utilized, which led to stable water injection using freshwater from nearby reservoirs after the initial seawater injection. It is confirmed that the water level was never lower than the top of the fuel in any of the pools, and none of the pools suffered any significant structural damage [2], in contrast to concerns raised during the weeks following the accident. The spent fuel pool, storing 1,500 fuel assemblies, was designed such that the fuel elements would retain integrity for 30 days without active cooling.
4 Release of Fission Products
The Nuclear and Industrial Safety Agency (NISA) and the Nuclear Safety Commission (NSC) estimated the total amount of radioactive materials released to the environment. NISA estimated the total discharged amount from reactors on the basis of the analytical results with severe accident analysis code, MELCOR, by Japan Nuclear Energy Safety Organization (JNES) [5, 6], as typically shown in Fig. 3.7. The NSC estimated the amount of nuclides discharged into the atmosphere with the assistance of the Japan Atomic Energy Agency (JAEA) [7, 8] through inverse calculations, based on the data of environmental monitoring and atmospheric diffusion calculation code, SPEEDI, as shown in Fig. 3.8. The estimated values summarized in Table 3.3 range between 1.2 and 1.6 × 1017 Bq for iodine-131 and 8 and 15 × 1016 Bq for cesium-137. Values estimated by TEPCO are also shown in Table 3.3. Estimated release of iodine-131 by TEPCO is about three times larger than values by NISA or NSC. It is also noted that the estimated releases of iodine-131 and cesium-137 of the Chernobyl accident [9] are about one order of magnitude larger and about 6 to 10 times larger than those estimated by NISA and NSC as shown in Table 3.3.

Estimated fission products (FP) release ratio to the environment with MELCOR code (Unit 2). Solid lines and dotted lines represent cumulative release fraction and release rate, respectively [6]

Estimated FP release to the environment with SPEEDI code
It may be noted that the containment S/C venting is conducted through several meters of water depth in a suppression chamber, and the effectiveness of this pool scrubbing for FP aerosols is usually very high, of the order of 103 as a decontamination factor. The estimation of FP release during S/C venting by TEPCO for Units 1 and 3 is not necessarily high compared with other periods [2].
5 Lessons Learned
After the accident at Fukushima Nuclear Power Plant, several investigation committees have been established, such as by the Independent Investigation Commission, TEPCO’s Investigation Committee, National Diet’s Investigation Committee, and Government’s Investigation Committee. They have issued investigation reports on the causes of the disaster, major lessons learned from the accident, and recommendations for the future [1–4]. Most of those reports judged that although the accident was triggered by a massive force of nature, it showed existing weaknesses regarding defense against natural hazards, regulatory oversight, and insufficient accident management, emergency response, and emergency training that allowed the occurrence and escalation of the accident [10].
For example, the Independent Investigation Commission [1] mentioned that the Fukushima accident is a “man-made disaster–unprepared nuclear severe accident” because of ambiguous private corporate management by TEPCO under the national nuclear policy. It states that the main cause of the accident is complete lack of crisis management and leadership in both the Government and TEPCO. It also emphasized the utmost importance for resilience to be greatly enhanced for the future. TEPCO’s Investigation Committee [2] mentions that enhanced accident measures both in hardware and in software are to be prepared, and recommends that the Government clearly establishes the standards of the emergency offsite center and guidelines of external events that have extremely low probabilities and high consequences. It emphasized the importance of the company-wide enhancement of risk management systems. National Diet’s Investigation Committee [3] raises several recommendations, such as monitoring of the nuclear regulatory body by the National Diet, reform of the crisis management system, Government’s responsibility for public health and welfare, and development of a system of independent investigation commissions in the National Diet. The Government’s Investigation Committee [4] points out several important recommendations, such as establishment of a basic stance for safety measures and emergency preparedness, safety measures regarding nuclear power generation, nuclear emergency response systems, harmonization with international practices in nuclear safety, and continued investigation of the accident causes and damage of the Fukushima accident.
Several measures, such as enhanced power supply capabilities, improved severe accident management policies, and strengthened emergency preparedness capabilities, have already been put in place based on the identified causes and lessons learned from the accident, and some mid-/long-term measures, such as a filtered containment venting system and increased seawall, are being implemented at nuclear power plant sites. Also, it is pointed out that professional leadership in nuclear organizations that manage potentially hazardous activities to maintain the risk to people and the environment as low as reasonably achievable without compromise is of utmost importance, thereby assuring stakeholder trust [10].
The underlying essential lesson will be that a sense of crisis and tension toward a possible severe accident were completely lacking, and groundless overconfidence against nuclear safety covered all nuclear sectors in Japan. Also it is evident that fully flexible resilience by the maximum use of existing hardware and software with enhanced knowledge, experience, monitors, predictive capability, exercises, and management is the only possible way to effectively cope with “unexpected” events that are largely beyond design base. We should learn these important lessons with humility, share them among all throughout the world, and reflect on them to a future even higher level of safety for current nuclear reactors. Because long-term relocation completely destroys local communities, advanced reactors without the need of evacuation, in principle, should be developed and deployed for the future. Associated important severe accident research items are being systematically identified, for example, by the efforts of the Atomic Energy Society of Japan [11].
Lastly, it may be noted that the Nuclear Regulation Authority (NRA) has been newly established in September 2012, as an independent commission body that solely exercises regulatory authority in the field of nuclear safety and security in Japan. As of July 2013, only 2 units of about 50 units are in operation, although the Government is expecting the restart of the operation of idling nuclear power plants, after satisfying new safety regulation rules [12] in force by the NRA in July 2013, as an important power source.
6 Summary
-
1.
Although some details of the accidents of Fukushima Daiichi Nuclear Power Plant are still not well known, the sequences, causes, and consequences of the accidents have been basically clarified by the efforts of several investigation committees established in Japan.
-
2.
The fission products released to the environment were estimated by the severe accident analysis code from inside the reactor core, and also by the atmospheric dispersion simulations code by coupling with environmental monitoring data in the reverse estimation method from outside the plant. The estimated release amount of 131I is of the order of 120–160 PBq, and that of 137Cs is of the order of 8–15 PBq for both estimations.
-
3.
Lessons learned from the accident identified by investigation committees cover a wide spectrum of insufficient measures, such as for earthquake and tsunami, station blackout, severe accident management, common cause accident at multiple unit sites, education and training, chain of command at the accident, disaster prevention, and safety regulation system. These lessons should be shared all over the world for the higher level of safety assurance of current reactors, and advanced reactors without the need of evacuation in principle should be developed for the future.
References
Independent investigation commission on the Fukushima daiichi nuclear accident (Feb. 2012) investigation and verification report
The Tokyo Electric Power Company Inc. (June 2012) Fukushima nuclear accident analysis report (Final Report)
The National Diet of Japan (July 2012) The Official Report of the Fukushima Nuclear Accident Independent Investigation Commission
Government of Japan (July 2012) Final report of the investigation committee on the accident at Fukushima nuclear power stations of Tokyo Electric Power Company
Nuclear and Industrial Safety Agency (2011) Discharge of radioactive materials to the environment (Chapter VI). Report of Japanese government to the IAEA ministerial conference on nuclear safety
Hoshi H et al. (April 2011) Computational analysis on accident progression of Fukushima Dai-ichi NPS. PSAM topical conference in Tokyo, Japan
Chino M et al (2011) Preliminary estimation of release amounts of 131I and 137Cs accidentally discharged from the Fukushima Daiichi Nuclear Power Pplant into the atmosphere. J Nucl Sci Technol 48:1129–1134
Terada H et al (2012) Atmospheric discharge and dispersion of radionuclides during the Fukushima Dai-ichi Nuclear Power Plant accident. Part II: Verification of the source term and analysis of regional-scale atmospheric dispersion. J Environ Radioact 112:141–154
OECD NEA (1995) The Chernobyl reactor accident source term—development of a consensus view. OECD NEA/CSNI/R(95)24.
Kondo S (April 2013) Lessons learned from Fukushima for PSAM community: Leadership and responsibility to assess and inform risk for safety assurance. In: PSAM topical conference in Tokyo, Japan
Sugimoto J (July 2013) Important severe accident research issues after accident at Fukushima Daiichi Nuclear Power Station. 21st international conference on nuclear engineering. Chengdu, China
Fuketa T (March 2013) Proposed regulatory requirements in Japan. Regulatory Information Conference, Bethesda
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Copyright information
© 2014 The Author(s)
About this chapter
Cite this chapter
Sugimoto, J. (2014). Accident of Fukushima Daiichi Nuclear Power Plant: Sequences, Fission Products Released, Lessons Learned. In: Takahashi, S. (eds) Radiation Monitoring and Dose Estimation of the Fukushima Nuclear Accident. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54583-5_3
Download citation
DOI: https://doi.org/10.1007/978-4-431-54583-5_3
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54582-8
Online ISBN: 978-4-431-54583-5
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)