
Abstract
The protozoal and helminthic parasites that traverse the respiratory tract during their life cycles can cause lung diseases, though the most common habitats of these parasites are the gastrointestinal tract and the blood or lymphatic circulations. These diseases are commonly encountered in the tropical regions of the world. However, parasitic lung diseases are increasingly being reported from other parts of the world due to an increase in the occurrence of immunosuppression (acquired immunodeficiency syndrome, organ transplantations, the use of immunosuppressive drugs) and transcontinental travel. The lung diseases that may result from these infections range from asymptomatic phase to life-threatening acute respiratory distress syndrome. These diseases can also mimic common respiratory diseases such as bacterial pneumonias, pulmonary tuberculosis, lung cancer, bronchial asthma, interstitial lung disease, and pulmonary hypertension. The diagnosis of parasitic lung diseases is a challenge to physicians, if they are not aware of the entity or these diseases are not investigated properly. The diagnosis of these diseases is based on the identification of the causative organism in the stool, sputum, other body fluids, or tissue specimens. Radiological imaging studies of the thorax including chest radiographs, high-resolution computerized tomograms, and ultrasonograms may aid in the diagnosis. In certain situations, invasive investigations such as fiberoptic bronchoscopic evaluation (transbronchial lung biopsies and bronchoalveolar lavage studies) and thoracic surgical procedures (thoracoscopy and open lung biopsy) may be required for a diagnosis and also to exclude other lung diseases. Serologic and molecular diagnostic methods are being developed for accurate diagnosis of the parasitic diseases.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Idiopathic Pulmonary Fibrosis
- Visceral Leishmaniasis
- Cystic Hydatid Disease
- Alveolar Echinococcosis
- Echinococcus Multilocularis
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1.1 Introduction
Pulmonary parasitic lung diseases are commonly diagnosed in countries where the prevalence of parasitic infection is high. However, there is an increase in the number of patients diagnosed as parasitic lung diseases recently, even in countries of low prevalence of parasitic infection which demands an awareness of such diseases in these countries. This increase in diagnosis in countries with low prevalence with parasitic infections has been attributed to an increase in the numbers of immunosuppressed individuals due to various reasons, organ transplantations and global travel [1]. The parasites can cause a wide spectrum of lung diseases varying from mild self-limiting bronchitis to life-threatening acute respiratory distress syndrome [2]. In addition, parasitic lung diseases may mimic diseases such as bacterial pneumonias, pulmonary tuberculosis, bronchial asthma, lung cancer, interstitial lung disease, and pulmonary hypertension. Both protozoal and helminthic parasites can cause lung diseases and helminthic lung infections are important causes of eosinophilic lung diseases [3]. Though the treatment of parasitic lung diseases is with specific antiparasitic drugs, the physicians treating such diseases should be competent in tackling the specific issues related to lung injury and sequel that may follow such infections. The lung diseases that may result from infections with parasites are listed in Table 1.1 [4].
1.2 Protozoal Parasites
The important protozoal parasites that cause pulmonary diseases are Entamoeba histolytica, Leishmania donovani, malarial parasites (Plasmodium vivax, P. falciparum, P. malaria, P. ovale, and P. knowlesi), Babesia spp. (Babesia microti and Babesia divergens), and Toxoplasma gondii.
1.2.1 Pulmonary Amebiasis
1.2.1.1 Clinical Diagnosis
Amebiasis results from ingestion of mature Entamoeba histolytica cysts in fecally contaminated food, water or from hands. Infection with Entamoeba histolytica can lead to intestinal colonization, colitis or extraintestinal manifestations resulting from the hematogenous spread of infection from the intestine. About 90 % of intestinal colonization is with nonpathogenic species, Entamoeba dispar and Entamoeba moshkovskii. Invasive amebiasis occurs in 10 % of persons colonized with E. histolytica. Patients with amebic colitis present with several-week history of cramping abdominal pain, weight loss, and watery or bloody diarrhea. Extraintestinal amebic infection can manifest as amebic liver abscess, splenic abscess, brain abscess, empyema, and pericarditis. Nearly 80 % of cases of amebic liver abscesses occur in the right lobe. The most common complication of amebic liver abscess is rupture into the pleural space resulting in pleuropulmonary amebiasis [5]. The main symptoms in pleuropulmonary amebiasis are fever, cough, hemoptysis, right upper quadrant abdominal pain, and chest pain. Some patients may present with respiratory distress and shock. Lung abscess, hepatobronchial fistula, and bronchopleural fistula with pyopneumothorax have also been reported. Expectoration of anchovy sauce-like pus indicates amebiasis [6]. The findings of elevated hemidiaphragm, tender hepatomegaly, pleural effusion, and basal pulmonary involvement are suggestive of pleuropulmonary amebiasis. Amebiasis can be suspected in patients with a history of immigration from or travel to developing countries and many patients give history of dysentery and alcoholism.
1.2.1.2 Laboratory Diagnosis
Amebiasis is commonly diagnosed by microscopy and cysts or motile trophozoites can be identified on a saline wet mount of a stool specimen [7]. Microscopic examination of fresh stools, sputum or pleural pus, rectal smears or rectosigmoidoscopy materials, pus from liver abscesses, and colonic biopsy samples may reveal motile trophozoites, even though it is a relatively specific test but is not sensitive for the identification of E. histolytica. The presence of ameba in the stool does not indicate that the disease is due to pathogenic E. histolytica as two other nonpathogenic species found in humans (E. dispar and E. moshkovskii) are indistinguishable morphologically [8, 9]. This method can, therefore, give false-positive results if Entamoeba dispar or Entamoeba moshkovskii infection is present. However, it has been reported recently that several different genotypes of E. dispar can be potentially responsible for tissue damage similar to that observed with E. histolytica [10]. A nonpathogenic Entamoeba gingivalis which is present in the oral cavity has to be differentiated from Entamoeba histolytica in sputum samples. A combination of serological tests with identification of the parasite by antigen detection by PCR is the best approach to diagnosis.
In vitro culture by inoculation of portions of stool, liver abscess, or empyema fluid into sterile culture media and incubating it at 37 °C is also useful in the diagnosis of amebiasis. The culture media is examined for the growth of amebic trophozoites, which, if present, can be seen on the walls of test tubes or in debris [11]. Antibody detection and antigen detection are other important immunodiagnostic methods. Indirect hemagglutination (IHA) test is used for routine serodiagnosis of amebiasis. Antigen consists of a crude soluble extract of axenically cultured organisms. The enzyme immunoassay (EIA) test detects antibody specific for E. histolytica in approximately 95 % of patients with extraintestinal amebiasis, 70 % of patients with active intestinal infection, and 10 % of asymptomatic persons who are passing cysts of E. histolytica. Detectable E. histolytica-specific antibodies may persist for years after successful treatment, so the presence of antibodies does not necessarily indicate acute or current infection. Specificity is 95 % or higher and false-positive reactions rarely occur. E. histolytica-specific antigen detection may be useful as an adjunct to microscopic diagnosis in detecting parasites and to distinguish between pathogenic and nonpathogenic infections. Detection of circulating antigens in the serum has been found to be an important advancement in the diagnosis [12]. Polymerase chain reaction (PCR) assays are useful for the differentiation of E. histolytica, E. dispar, and E. moshkovskii and for genetic typing of isolates [13, 14]. However, these tests are time-consuming and expensive and, hence, are not practical in areas endemic for amebiasis.
1.2.2 Pulmonary Leishmaniasis
1.2.2.1 Clinical Diagnosis
Infection with Leishmania donovani causes visceral leishmaniasis and is transmitted by various species of Phlebotomus, the sand fly [15]. There are no clinical symptoms and signs that are pathognomonic of visceral leishmaniasis (VL) or kala-azar. The symptoms and signs suggestive of visceral leishmaniasis are irregular fever, weight loss, enlargement of liver and spleen, and anemia. Pneumonitis, septal fibrosis, pleural effusion, and mediastinal adenopathy are reported in patients coinfected with human immunodeficiency virus (HIV) [16]. Leishmaniasis has also been reported in lung transplant patients [17]. Leishmania amastigotes can be found in the alveoli, pulmonary septa, and bronchoalveolar lavage (BAL) fluid. Diagnosis of leishmaniasis is by the demonstration of the parasites in bone marrow aspirates and by the identification of specific DNA sequences in tissues by molecular biology techniques [18]. The differential diagnosis of leishmaniasis includes malaria, cirrhosis with portal hypertension, miliary tuberculosis, brucellosis, histoplasmosis, lymphoma, and leukemia [19].
1.2.2.2 Laboratory Diagnosis
The diagnosis of leishmaniasis is based on the microscopical demonstration of Leishmania amastigotes in the relevant tissue aspirates or biopsies such as bone marrow, spleen, lymph nodes, or liver, skin slit smears, or in the peripheral blood buffy coat [19]. The smears can be stained with Romnowsky’s, hematoxylin-eosin, or immunoperoxidase stains. The amastigote stage seen in clinical samples is known as Leishman-Donovan (LD) bodies. The amastigotes observed in the smears have to be differentiated from “dot”-like structures (e.g., Histoplasma spp., platelets) by looking for the characteristic size (2–4 mm in diameter), shape (round to oval), and the internal organelles (the nucleus and kinetoplast). Culture of these specimens on solid NNN medium will demonstrate promastigotes. Immunological methods of diagnosis include indirect fluorescent test (IFA), direct agglutination test (DAT), and enzyme-linked immunosorbent assay (ELISA) to detect antibodies against Leishmania [20]. Antigen detection tests are better means of diagnosis of active leishmaniasis [21]. The antigen detection is the ideal test in immunocompromised patients, where antibody response is very poor. PCR is found to be the most sensitive and specific molecular test and is useful in molecular epidemiological studies besides diagnosis [22].
1.2.3 Pulmonary Malaria
1.2.3.1 Clinical Diagnosis
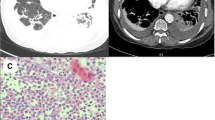
Malaria is caused by the obligate intraerythrocytic protozoa of the genus Plasmodium and is primarily transmitted by the bite of an infected female Anopheles mosquito. Five species of malarial parasites (Plasmodium vivax, P. falciparum, P. malariae, P. ovale, and P. knowlesi) infect man [23]. The main symptoms of malaria are periodic fever, chills, malaise, headache, abdominal pain, and vomiting, usually manifesting 10–15 days after mosquito bite. Anemia and splenomegaly are other important findings in malaria. Falciparum malaria is the most deadly type. The pulmonary manifestations range from cough to severe and rapidly fatal non-cardiogenic pulmonary edema and acute respiratory distress syndrome (ARDS) (Fig. 1.1) [24]. Acute lung injury and ARDS have also been reported to occur in infection with P. vivax and P. ovale [25, 26]. There has been no convincing evidence for the existence of true malarial pneumonitis, and if it occurs, it may be due to viral and secondary bacterial infections. Diffusing capacity was significantly impaired in patients with severe malaria. In addition to ARDS, falciparum malaria can cause many other severe complications such as cerebral malaria, acute renal failure, severe anemia, thrombocytopenia, bleeding, and gastrointestinal, hepatic, and metabolic complications [27].

Chest skiagram showing bilateral fluffy shadows in a patient presenting with acute respiratory distress syndrome due to severe falciparum malaria (Adapted from Vijayan and Kilnai [2])
1.2.3.2 Laboratory Diagnosis
Microscopic examination of the Giemsa-stained blood smears is the gold standard for the diagnosis of malaria. Microscopic diagnosis is based on staining thick and thin blood films on a glass slide to visualize the malaria parasite [28]. It is inexpensive, able to differentiate malaria species and quantify parasites. The detection threshold in Giemsa-stained thick blood film has been estimated to be 4–20 parasites/μL. Plasmodium species can be correctly recognized in thin blood film. Sometimes malarial parasites cannot be detected in peripheral blood smear, but malaria pigments may be seen in circulating phagocytic leukocytes. This is a pathognomonic sign of recent infection. The parasite count, number of circulating pigment-containing phagocytes, and the presence of late asexual stages of the parasite observed in the blood smear are all positively correlated with a fatal outcome. Bone marrow aspirate can also demonstrate malarial parasites, if thin smears of the peripheral blood do not show the parasites. Quantitative buffy coat (QBC) method involves staining parasite deoxyribonucleic acid (DNA) in micro-hematocrit tubes with fluorescent dyes (e.g., acridine orange) and its subsequent detection by epifluorescent microscopy. The parasite nuclei fluoresces bright green and the cytoplasm appears yellow-orange [29].
Rapid diagnostic test (RDT) is a device that detects malaria antigen in a small amount of blood, usually 5–15 μL, by immunochromatographic assay with monoclonal antibodies directed against the target parasite antigen and impregnated on a test strip [30, 31]. The result, usually a colored test line, is obtained in 5–20 min. Histidine-rich protein 2 (HRP-2) which is specific for P. falciparum is the most common malaria antigen targeted [32]. Plasmodium lactate dehydrogenase (PLDH) enzyme is the other group of targeted antigens. Monoclonal antibodies against pLDH and aldolase enzymes are available for the detection of Plasmodium spp. (pan malaria). HRP-2 often persists in the patient’s blood for weeks after successful treatment.
Molecular methods such as PCR allow the specific amplification of a selected region of the malarial genome. This is a specific and sensitive method and permits genotyping. Drug-resistant parasites and mixed infections can be detected by PCR using single nucleotide polymorphism. A PCR-based detection of Plasmodium falciparum in human urine and saliva samples has been described. The antibodies against asexual blood stages of malaria parasite can be detected by the immunofluorescence assay (IFA). Serological tests are useful in epidemiology surveys and are not suitable for the acute diagnosis of malaria [32].
1.2.4 Pulmonary Babesiosis
Babesiosis is caused by hemoprotozoan parasites, Babesia microti and Babesia divergens [33]. Man gets the infection by the bite of an infected tick, Ixodes scapularis, and can also be infected from a contaminated blood transfusion [34]. The parasites attack the red blood cells and can be misdiagnosed as Plasmodium. The symptoms are fever, drenching sweats, tiredness, loss of appetite, myalgia, and headache. Acute respiratory distress syndrome occurring a few days after initiation of medical therapy is the important pulmonary manifestation [35]. Chest radiological features include bilateral infiltrates with an alveolar pattern and thickening of the septa. The peripheral blood smears may show, in addition to ring forms, tetrads inside the red blood cells. These tetrads, known as Maltese cross formations, are pathognomonic of babesiosis because they are not seen in malaria [36]. Specific diagnosis is made by examination of a Giemsa-stained thin blood smear, DNA amplification using PCR, or detection of specific antibody [33].
1.2.5 Pulmonary Toxoplasmosis
Toxoplasmosis is caused by one-celled protozoan parasite, Toxoplasma gondii. Cats are the primary carriers of the organism [37]. Man gets the infection by eating parasitic cyst-contaminated raw or undercooked meat, vegetables, or milk products. The symptoms of toxoplasmosis are flu-like syndrome, enlarged lymph nodes, or myalgia. Chronic toxoplasmosis can cause chorioretinitis, jaundice, encephalitis, and convulsions. Pulmonary toxoplasmosis has been reported with increasing frequency in patients with HIV infection. Toxoplasma pneumonia can manifest as interstitial pneumonia/diffuse alveolar damage or necrotizing pneumonia [38]. Diagnosis of toxoplasmosis is based on the detection of the protozoa in body tissues. Antibody levels can be increased without active disease. A real-time PCR-based assay in BAL fluid has been reported in immunocompromised HIV-positive patients [39].
1.3 Helminthic Parasites
The important helminthic parasites that cause lung diseases include cestodes (Echinococcus granulosus and Echinococcus multilocularis), trematodes (Schistosoma haematobium, Schistosoma mansoni, Schistosoma japonicum, and Paragonimus westermani), and nematodes (Ascaris lumbricoides, Ancylostoma duodenale, Necator americanus, Strongyloides stercoralis, Wuchereria bancrofti, Brugia malayi, Brugia timori, Dirofilaria immitis, Dirofilaria repens, Toxocara canis or cati, and Trichinella spiralis).
1.3.1 Pulmonary Hydatid Disease
The parasite species that cause hydatid disease in man are Echinococcus granulosus and Echinococcus multilocularis.
1.3.2 Cystic Hydatid Disease
The adult E. granulosus resides in the small intestine of the definitive hosts, mainly dogs. The intermediate hosts including man are infected by ingestion of eggs excreted in the feces of the dogs. Primary pulmonary cystic hydatid disease is usually single. Multiple cysts may be seen in 20 % of cases and may be unilateral or bilateral [2]. Secondary metastatic pulmonary cystic hydatid disease may occur by the rupture of a liver cyst in vena caval circulation or a heart cyst in the right ventricular cavity. Patients are asymptomatic in the initial stages of infection. Pulmonary symptoms include cough, fever, dyspnea, and chest pain [40]. Signs and symptoms can occur due to compression of adjacent tissue by the cysts. Rupture of the cysts into a bronchus may result in hemoptysis and expectoration of cystic fluid containing parasite membrane and can cause anaphylactic shock, respiratory distress, asthma-like symptoms, persistent pneumonia, and sepsis [41, 42]. Rupture of the cyst into the pleural space can result in hydropneumothorax, pleural effusion, and empyema. Diagnosis of pulmonary hydatid cyst is based on thoracic imaging studies (chest radiography, thoracic computerized tomography (CT), and thoracic ultrasonography) [43] and an uncomplicated cyst presents as a well-defined homogenous round (cannonball) opacity that may be lobulated by contiguous bronchovascular axes (Fig. 1.2) [2]. Chest radiographs show solitary or multiple round opacities that may mimic lung tumors. CT is helpful in doubtful cases, because the internal structure of the cyst can be analyzed and its density measured. CT is also useful to assess the state of the neighboring parenchyma and to evaluate the whole thorax and abdomen for associated cystic lesions or anomalies. Ultrasonography using a portable ultrasound scanner has been found as reliable, inexpensive, and rapid technique in community-based screening surveys for cystic hydatid disease. The crescent sign, Cumbo’s sign (onion peel sign), water lily sign, and air-fluid level are seen on chest radiography and computed tomography (CT) [41]. Inverse crescent sign, signet ring sign, and serpent sign are recognized as features of pulmonary hydatid cysts in computerized tomogram.

Bilateral typical “cannon ball” images of non-complicated hydatid cysts on chest X-rays (Adapted from Vijayan and Kilnai [2])
Laboratory tests are complementary to clinical and imaging investigations. Eosinophilia and elevated immunoglobulin E (IgE) levels are seen when the hydatid cyst ruptures [40]. Serologic tests are less sensitive in patients with lung hydatid disease than in those localized in liver. False-positive tests may be observed in patients suffering from other helminthic infections. Immunologic tests may be helpful to confirm the hydatid origin of a cystic lesion and permit the serologic monitoring of medically or surgically treated patients [44, 45].
1.3.3 Pulmonary Alveolar Echinococcosis
Pulmonary alveolar echinococcosis (AE) is due to hematogenous dissemination from hepatic lesions. The liver is the first target of the parasite, with a silent and long incubation period (5–15 years). Exogenous proliferation causes infiltration of adjacent tissues and pressure necrosis. It can metastasize to distant organs mainly to lungs, brain, and bones [46]. Lung involvement results from metastatic dissemination or direct extension through the diaphragm of hepatic echinococcosis with intrathoracic rupture into the bronchial tree, pleural cavity, or mediastinum. Direct extension to the right atrium through the inferior vena cava with recurrent episodes of pulmonary embolism has also been reported. Imaging studies with radiography, ultrasonography, CT, and magnetic resonance imaging (MRI) may help in the diagnosis of metastatic lung disease [2]. Biopsy may be needed to confirm the diagnosis [47]. Serologic tests (ELISA, indirect hemagglutination assay [IHA]) are available and are of great value for early detection in endemic areas to confirm the diagnosis and to plan early surgery. Immunodiagnostic tests using purified E. multilocularis antigens have good diagnostic sensitivity and specificity for the diagnosis of AE [48].
1.3.4 Pulmonary Schistosomiasis
1.3.4.1 Clinical Diagnosis
The schistosomes that cause human disease are Schistosoma haematobium, Schistosoma mansoni, and Schistosoma japonicum. The final habitat of S. haematobium is urinary bladder vesicle beds and of S. mansoni and S. japonicum is the mesenteric beds. The schistosome eggs are passed in urine (S. haematobium) or in feces (S. mansoni and S. japonicum) by the infected humans. The parasites can cause Schistosoma dermatitis at the site of skin penetration. Pulmonary schistosomiasis can manifest clinically as an acute form and a chronic form [49]. Acute symptoms can develop 3–8 weeks after skin penetration [50]. The acute form, also known as Katayama syndrome, presents with fever, chills, weight loss, diarrhea, abdominal pain, myalgia, and urticaria and is seen in nonimmune patients [51]. Pulmonary manifestations include shortness of breath, wheezing and dry cough. Patients with chronic schistosomiasis present with features of pulmonary hypertension and cor pulmonale [52]. Massive hemoptysis and lobar consolidation and collapse have been reported in schistosomiasis [53]. Hepatosplenomegaly due to portal hypertension has been reported in patients infected with S. mansoni or S. japonicum [49]. Chest radiographic abnormalities range from multiple nodules to diffuse interstitial infiltrates. Small pulmonary nodules in CT have been described in acute schistosomiasis [54].
1.3.4.2 Laboratory Diagnosis
Diagnosis of chronic schistosomiasis is based on the demonstration of eggs in stool or urine by direct microscopy or rectal/bladder biopsy [55]. Multiple examinations of specimens are required in mild and chronic infections. In active infections, eggs contain live and mature miracidia. The incubation period of the infection is usually 3 months and hence eggs can be detected after 3 months of last known contact with fresh water. Peripheral blood eosinophilia with mild leukocytosis, abnormal liver function test results and elevated IgE levels are reported in acute schistosomiasis. Hyperglobulinemia is observed in chronic schistosomiasis. Serological tests with ELISA are available, but cannot differentiate active from past infections [56]. Bronchoscopy and transbronchial biopsy may reveal eosinophilic pneumonitis.
1.3.5 Pulmonary Paragonimiasis (Lung Fluke)
1.3.5.1 Clinical Diagnosis
Paragonimiasis is a food-borne zoonoses and is caused by infection with Paragonimus species and manifests as subacute or chronic inflammation of the lung. Though more than 50 species are known to cause paragonimiasis in man, the main species that cause paragonimiasis is Paragonimus westermani. Adult worms live in the lungs and the eggs are voided in sputum or feces. The man gets infection, when raw or undercooked crabs or crayfishes infected with infective metacercariae are ingested. The parasite from the human gut passes through several organs and tissues to reach the lung. Pulmonary paragonimiasis manifests as fever, chest pain, chronic cough, and blood-tinged sputum [57]. The cough is dry at first and later productive with blood-stained, rusty-brown tenacious sputum. Occasionally, there is profuse hemoptysis. Pulmonary paragonimiasis is confused with tuberculosis as the symptoms in both diseases are similar. Chest radiographs may show infiltrative, nodular, and cavitating shadows. Pleural effusion or pneumothorax is an important finding in paragonimiasis [58, 59]. CT scan may show single or multiple nodules in the lung parenchyma, calcified spots and pleural thickening with interlobar pleuritis, and pleural effusion. MRI may show conglomerated lesions with hemorrhage or tunnel signs.
1.3.5.2 Laboratory Diagnosis
Definitive diagnosis is based on the demonstration of eggs in sputum samples, BAL fluid, or lung biopsy specimens. Eggs are not present until 2–3 months after infection. Eggs or juvenile forms or adult worms can also be demonstrated in a subcutaneous lump or aspirated pleural effusion. Peripheral blood eosinophilia and elevated serum IgE levels are seen in >80 % of patients with paragonimiasis. A variety of immunological methods including ELISA, Dot immunogold filtration assay (DIGFA), indirect hemagglutination, and indirect fluorescence antibody tests have been used for diagnosis with variable results [2, 60].
1.3.6 Pulmonary Ascariasis
1.3.6.1 Clinical Diagnosis
Ascaris lumbricoides is the most common intestinal helminthic infection. Respiratory symptoms in ascariasis are due to larval pulmonary migration, airway hyper-reactivity, and bronchospasm. Symptomatic pulmonary disease may range from mild cough to Loffler’s syndrome [61]. Loffler’s syndrome is a self-limiting inflammation of the lungs and is associated with blood and lung eosinophilia. This syndrome can occur as a result of parasitic infestations (especially ascariasis in children) and exposure to various drugs. Patients may present with general symptoms of malaise, loss of appetite, fever lasting 2–3 days, headache, and myalgia. The respiratory symptoms include chest pain, cough with mucoid sputum, hemoptysis, shortness of breath, and wheezing [62]. There may be rapid respiratory rate and rales can be heard on auscultation. Leukocytosis particularly eosinophilia is an important laboratory finding. Chest radiographs demonstrate unilateral or bilateral, transient, migratory, and non-segmental opacities of various sizes. These opacities are often peripherally situated and appear to be pleural based [63]. The severity of symptoms will depend upon the larval burden. Rarely chronic eosinophilic pneumonia or symptoms of upper airway obstruction can occur.
1.3.6.2 Laboratory Diagnosis
A diagnosis of pulmonary disease due to ascariasis can be made in an endemic region in a patient who presents with dyspnea, dry cough, fever, and eosinophilia. Sputum may show Charcot-Leyden crystals and the chest radiograph may reveal fleeting pulmonary infiltrates. Because of the occurrence of respiratory symptoms during larval pulmonary migration, stool examination usually does not show Ascaris eggs and stool samples may be negative until 2–3 months after respiratory symptoms occur, unless the patient was previously infected. However, larvae can sometimes be demonstrated in respiratory or gastric secretions [64]. It has been suggested that measurement of Ascaris-specific IgG4 by ELISA may be useful in the serodiagnosis of ascariasis [65].
1.3.7 Pulmonary Ancylostomiasis
1.3.7.1 Clinical Diagnosis
Hookworm disease in humans results from infections with two species, Ancylostoma duodenale and Necator americanus. During pulmonary larval migration, patients may present with fever, cough, wheezing, and transient pulmonary infiltrates in chest radiographs. This is associated with blood and pulmonary eosinophilia [3]. The other characteristic feature is iron deficiency anemia due to chronic blood loss [66]. In severe hookworm anemia, patients may present with fatigue, exertional dyspnea, poor concentration, and cardiac murmurs. During massive infection from oral ingestion of hookworm larvae, patients can present with nausea, vomiting, cough, dyspnea, and eosinophilia, and this condition is termed as Wakana disease. Prominent gastrointestinal symptoms in hookworm disease are abdominal pain, nausea, anorexia, and diarrhea.
1.3.7.2 Laboratory Diagnosis
A direct microscopical examination of stool demonstrates the presence of characteristic hookworm eggs. Concentration method may be used when the infection is light. Eosinophilia in the peripheral blood is a prominent finding. A peripheral blood smear examination will reveal microcytic hypochromic anemia. A polymerase chain reaction (PCR) to differentiate between A. duodenale and N. americanus has been developed [67].
1.3.8 Pulmonary Strongyloidiasis
1.3.8.1 Clinical Diagnosis
Strongyloides stercoralis is seen worldwide and the unique feature of the life cycle of S. stercoralis is that it can complete its life cycle either in the human host or in the soil. It has been observed that 15–30 % of chronically infected people may be asymptomatic. Although symptoms in individuals with chronic Strongyloides stercoralis infection are usually mild, it can persist for many years due to autoinfection. This may occasionally progress to the hyperinfection syndrome with high mortality especially in immunosuppressed individuals [68, 69]. The relative risk of S. stercoralis infection is increased in elderly men and patients who had recently used corticosteroids, had a hematologic malignancy, and had prior gastric surgery. Other risk factors include chronic lung disease, use of histamine blockers, or chronic debilitating illness. Strongyloidiasis is a chronic relapsing illness of mild to moderate severity characterized by gastrointestinal complaints (diarrhea, pain, tenderness, nausea, vomiting), peripheral blood eosinophilia, and hypoalbuminemia.
Pulmonary signs and symptoms include cough, shortness of breath, wheezing, and hemoptysis. In patients at high risk for strongyloidiasis, adult respiratory distress syndrome and septicemia due to intestinal transmural migration of bacteria can occur as a result of hyperinfection or disseminated strongyloidiasis [70, 71]. In addition, acute anemia, acute renal failure, and systemic inflammatory response syndrome are also reported in hyperinfection. Strongyloidiasis can manifest as eosinophilic pleural effusion in both immunocompetent and immunocompromised individuals. Rare pulmonary manifestations include acute respiratory failure due to respiratory muscle paralysis, granulomatous reaction in the lung with interlobular septal fibrosis, and pulmonary microcalcifications. A paradoxic therapeutic response of asthma to glucocorticosteroids, in which bronchial asthma symptoms worsened after treatment with parenteral corticosteroids, has been described in patients with strongyloides superinfections [72]. Exacerbations of chronic obstructive pulmonary disease and worsening of symptoms in idiopathic pulmonary fibrosis have also been reported in Strongyloides stercoralis infection.
1.3.8.2 Laboratory Diagnosis
In immunocompetent patients with strongyloidiasis, the parasite load is usually low and the larval output is irregular. As a result, the diagnosis of strongyloidiasis by examination of a single stool specimen using conventional techniques usually fails to detect larvae in up to 70 % of cases [73]. The diagnostic yield can be increased by examination of several stool specimens on consecutive days. Examination of stool by agar plate culture method was found to be superior to direct smear and modified Baermann technique [74, 75]. Strongyloides stercoralis larvae can be demonstrated in duodenal aspirate. In disseminated disease, larvae and adult parasites can be seen in sputum, urine, bronchoalveolar lavage fluid, and other body fluids [76]. A serological test using Centers for Disease Control (CDC) enzyme immunoassay (EIA) for detection of antibodies to strongyloidiasis was found to have a sensitivity of 94.6 % in patients with proven infection [77].
1.3.9 Tropical Pulmonary Eosinophilia
1.3.9.1 Clinical Diagnosis
Tropical pulmonary eosinophilia (TPE) results from immunologic hyper-responsiveness to human filarial parasites, Wuchereria bancrofti and Brugia malayi [78–80]. TPE is a systemic disease involving mainly the lungs, but other organs such as liver, spleen, lymph nodes, brain, and gastrointestinal tract may also be involved. The disease occurs predominantly in males, with a male to female ratio of 4:1, and is mainly seen in older children and young adults between the ages 15 and 40 years. The systemic symptoms include fever, weight loss, and fatigue. Patients with TPE usually present with respiratory symptoms that include paroxysmal cough, breathlessness, and wheeze and chest pain [81, 82]. The symptoms occur predominantly at night, but can persist during the day. Severe cough can lead to fractured ribs. Sputum is usually scanty, viscous, and mucoid. The sputum often shows clumps of eosinophils, and rarely Charcot-Leyden crystals are observed. On examination, patients are often breathless. Bilateral scattered rhonchi and rales may be heard on auscultation [61, 78].
1.3.9.2 Laboratory Diagnosis
Leukocytosis with an absolute increase in eosinophils in the peripheral blood is the hallmark of TPE. Spontaneous fluctuations in the eosinophil count can occur. Absolute eosinophil counts are usually more than 3,000 cells/mm3 and may range from 5,000 to 80,000 [83]. Microfilariae are rarely seen in the peripheral blood. As patients with TPE especially from endemic areas can be simultaneously infected with other helminthic parasites, stool examination may reveal ova or larvae of other helminthes (Ascaris, Ancylostoma, whipworm, and Strongyloides) in 20 % of patients with TPE. This observation does not deter the physician from making a diagnosis of TPE, if other conditions for diagnosis are fulfilled.
The chest radiological features of TPE include reticulonodular shadows predominantly seen in mid and lower zones and miliary mottling of 1–3 mm in diameter often indistinguishable from miliary tuberculosis (Fig. 1.3). Twenty percent of patients have a normal chest radiograph. In patients with a long-standing history, a few patients have honeycomb lungs. Radiological improvement occurs on specific therapy with DEC, but some degree of radiological abnormality persists in some patients. Lung function tests reveal mainly a restrictive ventilation defect with superimposed airway obstruction [84, 85]. Single breath carbon monoxide transfer factor (TLCO) is reduced in 88 % of untreated patients with TPE. The reduction in TLCO is due to reduced pulmonary membrane diffusing capacity (Dm) [86]. The criteria suggested for the diagnosis of TPE are (a) appropriate exposure history (mosquito bite) in an endemic area of filariasis, (b) a history of paroxysmal nocturnal cough and breathlessness, (c) chest radiographic evidence of pulmonary infiltrations, (d) leukocytosis in blood, (e) peripheral blood eosinophils more than 3,000 cells per cu mm, (f) elevated serum IgE levels, (g) elevated serum antifilarial antibodies (IgG and/or IgE), and (h) a clinical response to diethylcarbamazine citrate [87, 88].

HRCT scan of a patient with TPE showing bilateral nodular shadows (Adapted from Vijayan and Kilnai [2])
1.3.10 Pulmonary Dirofilariasis
Pulmonary dirofilariasis is a zoonotic infection caused by filarial nematodes, Dirofilaria immitis and Dirofilaria repens. Humans are accidental hosts of this parasite which is transmitted to man by the mosquito. The parasites are usually seen in the pulmonary artery where they produce an embolism ultimately leading to the formation of a pulmonary nodule or “coin lesion” [89]. Nearly 50 % of subjects infected with dirofilariasis are asymptomatic. Clinical symptoms are chest pain, cough, fever, hemoptysis, and dyspnea. CT scan may show a well-defined nodule with smooth margin connected to an arterial branch [90]. Positron emission tomography scan can demonstrate hypermetabolic activity in a pulmonary infarct secondary to dirofilariasis [91]. A PCR-based diagnosis of D. repens in human pulmonary dirofilariasis has been reported [92]. A definitive histopathological diagnosis of pulmonary dirofilariasis can be made in tissue specimens obtained by wedge biopsy, by video-assisted thoracoscopy, or rarely by fine needle biopsy.
1.3.11 Visceral Larva Migrans
Toxocara larva migrans syndromes are important zoonotic infections. Certain nematode parasites entering into an unnatural host (e.g., man) may not be able to complete their life cycle and their progress is arrested in the “unnatural host.” The common parasites that cause visceral larva migrans (VLM) and eosinophilic lung disease in man are a dog ascarid (Toxocara canis) and less commonly a cat ascarid (Toxocara cati) [93]. Human toxocariasis occurs in all parts of the world wherever there is a large pool of infected dogs.
Visceral larva migrans (VLM) is characterized by leukocytosis and eosinophilia. The larva induces a granulomatous reaction in the tissues containing eosinophils and multinucleated giant cells. Larvae can get encapsulated within the granuloma where they are either destroyed or persist for many years in a viable state. Granulomata are found in the lungs, liver, central nervous system, and eyes. Later fibrosis and calcification occur. Larval antigens can cross-react with human A and B blood group antigens.
1.3.11.1 Clinical Diagnosis
Visceral larva migrans is usually reported in young children with a history of pica. A history of exposure to puppies or dogs supports the diagnosis of VLM. These children usually present with fever, cough, wheezing, eosinophilia, and hepatomegaly. However, most of the children infected with Toxocara spp. are asymptomatic. The main symptoms in patients with visceral larva migrans are fever, cough, wheezing, seizures, anemia, and fatigue. Pulmonary manifestations are reported in 80 % of cases and patients may present with severe asthma [94]. Scattered rales and rhonchi are heard on auscultation. There will be intense blood eosinophilia. Skiagram chest may reveal focal patchy infiltrates. In some cases, severe eosinophilic pneumonia may lead to respiratory distress [95]. Other clinical features include generalized lymph node enlargement, hepatomegaly, and splenomegaly.
1.3.11.2 Laboratory Diagnosis
Skiagram chest may show patchy infiltrates. Nonspecific changes include hypergammaglobulinemia and elevated isohemagglutinin titers to A and B blood group antigens. Serological tests by ELISA method using excretory-secretary proteins obtained from cultured T. canis may be useful in the diagnosis. Cross reactivity with other helminths limits the usefulness of this test in endemic areas. Detection of IgE antibodies by ELISA and toxocara excretory-secretary antigens by Western blotting procedure have also been reported for diagnosis [96, 97]. However, serodiagnostic procedures cannot distinguish between past and present infections. Histopathological examination of lung or liver biopsy specimens may demonstrate granulomas with eosinophils, multinucleated giant cells, and fibrosis. Since man is not the definitive host of Toxocara sp., eggs or larvae cannot be demonstrated in the feces.
1.3.12 Pulmonary Trichinellosis
Human trichinellosis is an important food-borne zoonosis. The most important species that infect man is Trichinella spiralis. The parasite has a direct life cycle with complete development in one host (pig, rat, or man). Man gets infection from raw and partially cooked pork, when infected pig’s muscle containing larval trichinellae is eaten by man. The common symptoms of trichinellosis are muscle pain, periorbital edema, fever, and diarrhea [98]. Pulmonary symptoms include dyspnea, cough, and pulmonary infiltrates. Dyspnea may be due to the involvement of diaphragm [99]. Leukocytosis, eosinophilia, and elevated levels of serum muscle enzymes (creatine phosphokinase, lactate dehydrogenase, aldolase, and amino transferase) are important laboratory findings. An enzyme-linked immunosorbent assay (ELISA) for detection of anti-Trichinella antibodies using excretory-secretary antigens may be useful in the diagnosis. A definitive diagnosis can be made by muscle biopsy (usually deltoid muscle) that may demonstrate larvae of T. spiralis [99].
References
Vijayan VK. Is the incidence of parasitic lung diseases increasing, and how may this effect modern respiratory medicine? Expert Rev Respir Med. 2009;3:339–44.
Vijayan VK, Kilani T. Emerging and established parasitic lung infestations. Infect Dis Clin North Am. 2010;24:579–602.
Vijayan VK. Immunopathogenesis and treatment of eosinophilic lung diseases in the tropics. In: Sharma Om P, editor. Tropical lung disease (lung biology in health and disease), vol. 211. New York: Marcel Dekker Inc; 2006. p. 195–239.
Vijayan VK. Parasitic lung infections. Curr Opin Pulm Med. 2009;15(3):274–82.
Ackers JP, Mirelman D. Progress in research on Entamoeba histolytica pathogenesis. Curr Opin Microbiol. 2006;9:367–73.
Shamsuzzaman SM, Hashiguchi Y. Thoracic amoebiasis. Clin Chest Med. 2002;23:479–92.
Gonzalez-Ruiz A, Haque R, Aguirre A, et al. Value of microscopy in the diagnosis of dysentery associated with invasive Entamoeba histolytica. J Clin Pathol. 1994;47:236–9.
Haque R, Petri Jr WA. Diagnosis of amebiasis in Bangladesh. Arch Med Res. 2006;37:273–6.
Haque R, Ali IKM, Akther S, et al. Comparison of PCR, isoenzyme analysis and antigen detection for diagnosis of Entamoeba histolytica infection. J Clin Microbiol. 1998;36:449–52.
Ximénez C, Cerritos R, Rojas L, et al. Human amebiasis: breaking the paradigm? Int J Environ Res Public Health. 2010;7:1105–20.
Diamond LS. A new liquid medium for xenic cultivation of Entamoeba histolytica and other lumen-dwelling protozoa. J Parasitol. 1982;68:958–9.
Tanyuksel M, Petri Jr WA. Laboratory diagnosis of amebiasis. Clin Microbiol Rev. 2003;16:713–29.
Tannich E, Horstmann RD, Knobloch J, et al. Genomic DNA differences between pathogenic and non pathogenic Entamoeba histolytica. Proc Natl Acad Sci U S A. 1989;86:5118–22.
Hamzah Z, Petmitr S, Mungthin M, et al. Development of multiplex real-time polymerase chain reaction for detection of Entamoeba histolytica, Entamoeba dispar, and Entamoeba moshkovskii in clinical specimens. Am J Trop Med Hyg. 2010;83:909–13.
Piscopo TV, Mallia AC. Leishmaniasis. Postgrad Med J. 2006;82:649–57.
Marshall BG, Kropf P, Murray K, et al. Bronchopulmonary and mediastinal leishmaniasis: an unusual clinical presentation of Leishmania donovani infection. Clin Infect Dis. 2000;30:764–9.
Antinori S, Cascio A, Parravicini C, et al. Leishmaniasis among organ transplant recipients. Lancet Infect Dis. 2008;8:191–9.
Guddo F, Gallo E, Cillari E, et al. Detection of Leishmania infantum kinetoplast DNA in laryngeal tissue from an immunocompetent patient. Hum Pathol. 2005;36:1140–2.
Singh S. New developments in diagnosis of leishmaniasis. Indian J Med Res. 2006;123:311–30.
Boelaert M, Rijal S, Regmi S, et al. Comparative study of the effectiveness of diagnostic tests for visceral leishmaniasis. Am J Trop Med Hyg. 2004;70:72–7.
Attar ZJ, Chance ML, el-Safi S, et al. Latex agglutination test for the detection of urinary antigens in visceral leishmaniasis. Acta Trop. 2001;78:11–6.
Tavares CA, Fernandes AP, Melo MN. Molecular diagnosis of leishmaniasis. Expert Rev Mol Diagn. 2003;3:657–67.
Freedman DO. Malaria prevention in short-term travelers. N Engl J Med. 2008;359:603–12.
Talwar A, Fein AM, Ahluwalia G. Pulmonary and critical care aspects of severe malaria. In: Sharma OP, editor. Lung biology in health and disease: tropical lung diseases. 2nd ed. New York: Taylor & Francis; 2006. p. 255–77.
Tan LK, Yacoub S, Scott S, et al. Acute lung injury and other serious complications of Plasmodium vivax malaria. Lancet Infect Dis. 2008;8:449–54.
Rojo-Marcos G, Cuadros-Gonzalez J, Mesa-Latorre JM. Acute respiratory distress syndrome in a case of Plasmodium ovale. Am J Trop Med Hyg. 2008;79:391–3.
World Health Organization. Guidelines for the treatment of malaria. Geneva: World Health Organization; 2006. p. 1–266.
Chotivanich K, Silamut K, Day NPJ. Laboratory diagnosis of malaria infection-a short review of methods. Aust J Med Sci. 2006;27:11–5.
Tanpukdee N, Duangdee C, Wilairatana P, Krudsood S. Malaria diagnosis: a brief review. Korean J Parasitol. 2009;47:93–102.
Moody A. Rapid diagnostic tests for malaria parasites. Clin Microbiol Rev. 2002;15:66–78.
Murray CK, Bell D, Gasser RA, et al. Rapid diagnostic testing for malaria. Trop Med Int Health. 2003;8:876–83.
Wongsrichanalai C, Barcus MJ, Muth S, et al. A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT). Am J Trop Med Hyg. 2007;77:119–27.
Krause PJ. Babesiosis. Med Clin North Am. 2002;86:361–73.
Swanson SJ, Neitzel D, Reed KD, et al. Co-infections acquired from Ixode ticks. Clin Microbiol Rev. 2006;19:708–27.
Boustani MR, Lepore TJ, Gelfand JA, et al. Acute respiratory failure in patients treated for babesiosis. Am J Respir Crit Care Med. 1994;149:1689–91.
Noskoviak K, Broome E. Babesiosis. N Engl J Med. 2008;358:e19.
Dodds EM. Toxoplasmosis. Curr Opin Ophthalmol. 2006;17:557–61.
Petersen E, Edvinsson B, Lundgren B, et al. Diagnosis of pulmonary infection with Toxoplasma gondii in immunocompromised HIV-positive patients by real time PCR. Eur J Clin Microbiol Infect Dis. 2006;25:401–4.
Contini C. Clinical and diagnostic management of toxoplasmosis in the immunocompromised patient. Parassitologia. 2008;50:45–50.
Savani DM, Sharma OP. Eosinophilic lung disease in the tropics. Clin Chest Med. 2002;23:377–96.
Kuzucu A. Parasitic diseases of the respiratory tract. Curr Opin Pulm Med. 2006;12:212–21.
Fanne RA, Khamaisi M, Mevorach D, et al. Spontaneous rupture of lung echinococcal cyst causing anaphylactic shock and respiratory distress syndrome. Thorax. 2006;61:550.
Brunetti E, Kern P, Vuitton DA. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114:1–16.
Hernandez-Gonzalez A, Muro A, Barrera L, et al. Usefulness of four different Echinococcus granulosus recombinant antigens for serodiagnosis of unilocular hydatid disease (UHD) and postsurgical follow-up of patients treated for UHD. Clin Vaccine Immunol. 2008;15:147–53.
Santivanez S, Garcia HH. Pulmonary cystic echinococcosis. Curr Opin Pulm Med. 2010;16:257–61.
Craig P. Echinococcus multilocularis. Curr Opin Infect Dis. 2003;16:437–44.
Ozkok A, Gul E, Okumus G, et al. Disseminated alveolar echinococcosis mimicking a metastatic malignancy. Intern Med. 2008;47:1495–7.
Carmena D, Benito A, Eraso E. The immunodiagnosis of Echinococcus multilocularis infection. Clin Microbiol Infect. 2007;13:460–75.
Schwartz E. Pulmonary schistosomiasis. Clin Chest Med. 2002;23:433–43.
Schwartz E, Rozenman J, Perelman N. Pulmonary manifestations of early Schistosoma infection in nonimmune travelers. Am J Med. 2000;109:718–22.
Doherty JF, Moody AH, Wright SG. Katayama fever; an acute manifestation of schistosomiasis. Br Med J. 1996;313:1071–2.
Hovnanian A, Hoette S, Fernandes CJ, et al. Schistosomiasis associated pulmonary hypertension. Int J Clin Pract Suppl. 2010;165:25–8.
Sera SI, Abulmaaty RA, Elnahas HA, et al. A diagnostic dilemma of right lower lobe collapse caused by pulmonary bilharsiasis. Heart Lung Circ. 2006;15:50–2.
Nguyen LQ, Estrella J, Jett EA, et al. Acute schistosomiasis in nonimmune travelers: chest CT findings in 10 patients. AJR Am J Roentgenol. 2006;186:1300–3.
Elliott DE. Schistosomiasis. Pathophysiology, diagnosis, and treatment. Gastroenterol Clin North Am. 1996;25:599–625.
Hassan MM, Medhat A, Makhlouf MM, et al. Detection of circulating antigens in patients with active Schistosoma haematobium infection. Am J Trop Med Hyg. 1998;9:295–301.
Xu ZB. Studies on clinical manifestations, diagnosis and control of paragonimiasis in China. Southeast Asian J Trop Med Public Health. 1991;22 Suppl 1:345–8.
Suwanik R, Harinasuta C. Pulmonary paragonimiasis: an evaluation of roentgen findings in 38 positive sputum patients in an endemic area in Thailand. Am J Roentgenol. 1959;81:236–44.
Mukae H, Taniguchi H, Matsumoto N, et al. Clinicoradiologic features of pleuropulmonary Paragonimus westermani on Kyushu Island, Japan. Chest. 2001;120:514–20.
Wongkham C, Intapan PM, Maleewong W, et al. Evaluation of human IgG subclass antibodies in the serodiagnosis of Paragonimus heterotremus. Asian Pac J Allergy Immunol. 2005;23:205–11.
Vijayan VK. Tropical parasitic lung diseases. Indian J Chest Dis Allied Sci. 2008;50:49–66.
Liu LX, Weller PF. Strongyloidiasis and other intestinal nematode infections. Infect Dis Clin North Am. 1993;7:655–82.
Citro LA, Gordon ME, Miller WT. Eosinophilic lung disease (or how to slice PIE). Am J Roentgenol Radium Ther Nucl Med. 1973;117:787–97.
Sarinas PS, Chitkara RK. Ascariasis and hookworm. Semin Respir Infect. 1997;12:130–7.
Bhattacharya T, Santra A, Mazumdar DN, et al. Possible approach for serodiagnosis of ascariasis by evaluation of immunoglobulin G4 response using Ascaris lumbricoides somatic antigen. J Clin Microbiol. 2001;39:2991–4.
Roche M, Layrise M. Nature and causes of hookworm anemia. Am J Trop Med Hyg. 1996;15:1031–102.
Howdon JM. Differentiation between the human hookworm Ancylostoma duodenale and Necator americanus using PCR-RFLP. J Parasitol. 1996;82:642–7.
Neva FA. Biology and immunology of human strongyloidiasis. J Infect Dis. 1986;153:397–406.
Lessman KD, Can S, Talavera W. Disseminated Strongyloides stercoralis in human immunodeficiency virus-infected patients: treatment failure and review of literature. Chest. 1993;104:119–22.
Wehner JH, Kirsch CM. Pulmonary manifestations of strongyloidiasis. Semin Respir Infect. 1997;12:122–9.
Ghoshal UC, Ghoshal U, Jain M, et al. Strongyloides stercoralis infestation associated with septicemia due to intestinal transmural migration of bacteria. J Gastroenterol Hepatol. 2002;17:1331–3.
Sen P, Gil C, Estrellas B, Middleton JR. Corticosteroid- induced asthma: a manifestation of limited hyperinfection syndrome due to Strongyloides stercoralis. South Med J. 1995;88:923–7.
Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040–7.
Hernadez-Chavarria F, Avendano L. A simple modification of the Baermann method for diagnosis of strongyloidiasis. Mem Inst Oswaldo Cruz (Rio de Janeiro). 2001;96:805–7.
De Kaminsky RG. Evaluation of three methods for laboratory diagnosis of Strongyloides stercoralis infection. J Parasitol. 1993;79:277–80.
Williams J, Ninley D, Dralle W, et al. Diagnosis of pulmonary strongyloidiasis by bronchoalveolar lavage. Chest. 1988;94:643–4.
Loutfy MR, Wilson M, Keystone JS, et al. Serology and eosinophil count in the diagnosis and management of strongyloidiasis in a non-endemic area. Am J Trop Med Hyg. 2002;66:749–52.
Vijayan VK. Tropical pulmonary eosinophilia. Curr Opin Pulm Med. 2007;13:428–33.
Pinkston P, Vijayan VK, Nutman TB, et al. Acute tropical pulmonary eosinophilia: characterization of the lower respiratory tract inflammation and its response to therapy. J Clin Invest. 1987;80:216–25.
Nutman TB, Vijayan VK, Pinkston P, et al. Tropical pulmonary eosinophilia: analysis of antifilarial antibody localized to the lung. J Infect Dis. 1989;160:1042–50.
Udwadia FE. Tropical eosinophilia. In: Herzog H, editor. Pulmonary eosinophilia: progress in respiration research. Basel: S. Karger; 1975. p. 35–155.
Ottesen EA, Nutman TB. Tropical pulmonary eosinophilia. Ann Rev Med. 1992;43:417–24.
Cooray JH, Ismail MM. Re-examination of the diagnostic criteria of tropical pulmonary eosinophilia. Respir Med. 1999;93:655–9.
Poh SC. The course of lung function in treated tropical eosinophilia. Thorax. 1974;29:710–2.
Vijayan VK, Kuppurao KV, Sankaran K, et al. Diffusing capacity in acute untreated tropical eosinophilia. Indian J Chest Dis Allied Sci. 1988;30:71–7.
Vijayan VK, Kuppurao KV, Sankaran K, et al. Pulmonary membrane diffusing capacity and capillary blood volume in tropical eosinophilia. Chest. 1990;97:1386–9.
Rom WN, Vijayan VK, Cornelius MJ, et al. Persistent lower respiratory tract inflammation associated with interstitial lung disease in patients with tropical pulmonary eosinophilia following treatment with diethylcarbamazine. Am Rev Respir Dis. 1990;142:1088–92.
Vijayan VK. How to diagnose and manage common parasitic pneumonias? Curr Opin Pulm Med. 2007;13:218–24.
Theis JH. Public health aspects of dirofilariasis in the United States. Vet Parasitol. 2005;133:157–80.
Oshiro Y, Murayama S, Sunagawa U, et al. Pulmonary dirofilariasis: computed tomographic findings and correlation with pathologic features. J Comput Assist Tomogr. 2004;28:796–800.
Moore W, Franceschi D. PET findings in pulmonary dirofilariasis. J Thorac Imaging. 2005;20:305–6.
Rivasi F, Boldorini R, Criante P, et al. Detection of Dirofilaria (Nochtiella) repens DNA by polymerase chain reaction in embedded paraffin tissues from two human pulmonary locations. APMIS. 2006;114:567–74.
Magnaval JF, Glickman LT, Dorchies P, et al. Highlights of human toxocariasis. Korean J Parasitol. 2001;39:1–11.
Feldman GJ, Parker HW. Visceral larva migrans associated with the hypereosinophilic syndrome and the onset of severe asthma. Ann Intern Med. 1992;116:838–40.
Bartelink AK, Kortbeek LM, Huidekoper HJ, Meulenubelt J, Van Knapen F. Acute respiratory failure due to toxocara infections. Lancet. 1993;342:1234.
Magnaval JF, Fabre R, Maurieres P, et al. Evaluation of an immunenzymatic assay detecting specific anti-Toxocara immunoglobulin E for diagnosis and post treatment follow up of human toxocariasis. J Clin Microbiol. 1992;30:2269–74.
Magnaval JF, Fabre R, Maurieres P, et al. Application of the Western- blotting procedure for the immunodiagnosis of human toxocariasis. Parasitol Res. 1991;77:697–702.
Capo V, Despommier DD. Clinical aspects of infections with Trichinella spp. Clin Microbiol Rev. 1996;9:47–54.
Bruschi F, Murrell K. Trichinellosis. In: Guerrant RL, Walker DH, Weller PF, editors. Tropical infectious diseases: principles, pathogens and practice, vol. 2 (Elsevier Science Health Science Div). Philadelphia: Churchill Livingstone; 1999. p. 917–25.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Vijayan, V.K. (2013). Diagnosis of Pulmonary Parasitic Diseases. In: Barrios, R., Haque, A. (eds) Parasitic Diseases of the Lungs. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-37609-2_1
Download citation
DOI: https://doi.org/10.1007/978-3-642-37609-2_1
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-37608-5
Online ISBN: 978-3-642-37609-2
eBook Packages: MedicineMedicine (R0)