
Abstract
Aging often leads to decreased social engagement. While technology has the potential to improve the quality of life among older adults, not much is known about effects of new technologies, including virtual reality (VR) applications, on their well-being. This paper reports on a field study conducted with older adults in assisted living communities to understand how use of a VR system may contribute to their emotional and social well-being. During the study, a two-week intervention was done with an experimental group that used a VR system to view contents related to travel and relaxation, and a control group that used a TV to view the same contents. Feedback collected before and after the intervention showed that the VR application provided more benefits compared to the control condition. Participants that used the VR system reported being less socially isolated, being less likely to show signs of depression, experiencing positive affects more frequently, and feeling better about their overall well-being. While the study has limitations to its generalizability, findings show the potential for using VR applications for improving the quality of life among the aging population.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
As people age, they become more likely to experience decrease in social activities. The issue is more severe among older adults living in long-term care communities, since they are often spatially and socially separated from others. Among those in long-term care communities, it has been reported that more than a quarter develop some form of dementia or depression [1]. Currently, technology interventions (e.g. television programs, internet, gaming systems, mobile devices) are often used as a way address issues related to isolation and loneliness, but have shown mixed results in their effectiveness to provide social stimuli and improve social interactions [2,3,4,5].
Among many possibilities for utilizing technology to maintain social and emotional well-being as people age is virtual reality (VR). VR is an emerging technology that immerses a user into an alternate environment, giving a complete sense of presence. With the ability to make its users feel more involved, absorbed, engaged and engrossed [6], VR has been suggested to have possibilities for triggering behavior change [7]. While studies on its potential benefits for the aging population has been limited to those with specific conditions, few studies have found evidence around the benefits of using VR on improving issues related to mental distress, memory function and cognition [8,9,10]. Based on existing research, VR is believed to be beneficial to the older adults due to its immersive interaction capabilities. However, its effects on older adults’ emotional and social well-being, including issues of loneliness and isolation, remains unanswered.
The objective of this study was to look at the impact of the VR experience on older adults’ social and emotional well-being. By introducing older adults to immersive virtual experiences, this study sought to test possibilities for reducing social isolation and improving emotional well-being. In this study, a group of older adults living in selected assisted living communities in the New England region of the US were given opportunities to experience a VR system with contents such as relaxation, travel and cultural experiences. Based on data collected from in-person surveys, this paper presents findings regarding effects of the VR experience on perceived well-being, physical conditions, emotional state and personality, and attitudes toward the system.
2 Related Studies
Existing research have looked at technologies available to the older adults and their effects, as well as how VR applications are used for both the general public and the older population. However, limited research has been done to show the effectiveness of using VR for older adults in terms of isolation, depression and overall well-being.
2.1 Technologies in Long-Term Care Communities
Older adults in long-term care communities are often separated from the general community. A variety of technology interventions have been cited to have the potential to improve social well-being among older adults in such communities. While television program is often considered as a conversation catalyst among older adults, however, recent research suggested that its effectiveness is not promising [3]. Use of the internet, which is also widely adopted in assisted and independent living communities, on the other hand, has been shown to be associated the decrease in loneliness scores [2]. The Wii exergames, with which older adults can use a physical controller on their hands to do exercise games such as bowling or golf, are also used in communities. A pilot study has shown significant improvement on balance using Wii interventions [11]. Tablet is another technology that is broadly used in long-term care communities, and has been shown to have the potential of increasing older adults’ overall social activity [5].
2.2 Virtual Reality as an Intervention
Virtual reality (VR) immerses a user into an alternate environment to give a sense of presence. It is gaining interest as an intervention for improving older adults’ well-being. In a recent study, it was concluded that virtual environments have the potential to influence, and in some cases, change human behavior [7]. A preliminary study have shown the benefits of using VR to address issues related to mental distress and cognition [10]. Another study that focused on cognitive rehabilitation looked at using VR for cognitive training, and found that VR-based systems support procedures for mitigating behavioral and psychological symptoms of mild cognitive impairments and early-stage Alzheimer’s disease [9]. Optale et al. [8] focused on memory issues among older adults, and described VR as a potential solution to discover new approaches to the treatment of memory deficits among older adults.
As summarized, studies have shown that technologies can help older adults by improving physical and mental health, decreasing loneliness, and fostering social interactions. However, discussions around use of VR applications for older adults’ emotional and social well-being are still limited.
3 Study Overview
3.1 System Design and Overview of Intervention
In order to evaluate the effectiveness of a VR intervention in improving older adults’ emotional and social well-being, the VR system shown in Fig. 1 was used. As shown in Fig. 1, the system consisted of a tablet that can control all VR headsets as activity director and multiple VR headsets (Samsung S7 and Samsung GearVR) that play the same contents to multiple older adults in group settings.

VR system used in study
The study intervention included a brief introduction and training at the beginning. During this session, researchers gave instructions regarding how to put the system on correctly, ensured that the headsets had a comfortable fit, and checked that all contents were running correctly and consistently for all participants. After the introduction, participants kept the system for two weeks. During each daily session, an activity director gathered participants, helped them wear the VR headsets, and adjusted the systems so that everyone was getting a clear image. Once setup was completed, the activity director used the tablet to play different categories of content including 360 videos, Google Street View, and guided tours. The 360 images or videos showed up simultaneously on all VR headsets, giving the participants the same view. Contents included images for relaxation, world travel, cultural events, and places the participants have been to or grew up in. Guided tours were provided using scripts that were shown to the activity director. Each viewing session was designed to last about 20 min.
The researchers stayed in constant communication with community staff during the two-week period. After the study intervention period, the researchers returned to the sites to collect the systems and to gather feedback from participants.
3.2 Data Collection
Participants. Residents of selected assisted living communities in Massachusetts and New Hampshire were provided with the VR headsets. A control group with similar characteristics were provided with TV viewing experiences, with the same content, in order to comparatively measure the possible effects of using the VR system.
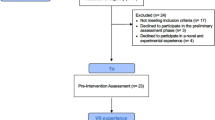
A total of 63 participants from four assisted living communities were involved in the study. The four community sites were all operated by the same organization with comparable living arrangements, facilities and services. Among the four community sites, two were assigned as the experimental group with the VR intervention, and the other two were assigned as the control group that was provided the same contents on TV. Participants’ year of birth ranged from 1918 to 1950, with a median birth year of 1930. Half of them were born between 1928 and 1935. The sample was initially 62% female. Table 1 summarizes sample characteristics by experimental conditions and study sites.
Recruiting was done with help from the staff at the assisted living communities. These employees were familiar with their residents’ conditions and personal preferences, and had frequent contact with them. Based on the study description, employees connected the researchers with residents who they felt would be capable and available to participate. Since the study was not focused on older adults’ cognitive status or performance, residents’ cognitive capabilities were not taken into account during recruitment. Rather, the staff identified those whom they knew would be capable of complying with the instructions around using the VR or TV equipment and participating in the study in a group setting, as well as taking part in interviews and completing questionnaires.
Participation was voluntary and based on informed consent. Potential participants identified by the staff were presented with a study overview and given an informed consent document that outlined potential benefits and risks of participation. Only those who fully understood the study description and provided written consent were enrolled. Participants were reminded that they could withdraw themselves from the study at any time if they wish to do so. For those who had a legal representative or guardian, a copy of the consent form was also given to the person to review and sign upon agreement.
Measures and Questionnaire Design.
A set of measures were selected and defined to gather data on perceived well-being, physical conditions, emotional state and personality, and attitudes toward the system. Most of the measures used in this study were selected from past studies that involved empirical measurement and/or inquiry of health, well-being, technology experience, and perceptions and attitudes toward new systems.
During the study, in-person surveys were administered with all participants before and after the interventions they were assigned to. Questions on health, well-being and emotional state were asked before and after the intervention. Questions about perceptions of and attitudes toward the given system were also asked before and after the system experience, but with the phrasing altered. While the pre-intervention questionnaire included perceptions and attitudes regarding the system based on the first impression, the post-intervention questionnaire asked the same questions but based on actual interactions with the system. The post-intervention questionnaire also asked participants about the actual usage of the system during the given time, as well as their thoughts regarding specific parts of the system. Demographic questions were asked before the intervention. The measures used in this study are described in Table 2.
4 Results
Data gathered from participants’ responses to questions listed in Table 2 were analyzed using paired samples t-test. Using the t-test for mean comparison, responses to corresponding questions in the pre- and post-intervention questionnaires for the two conditions were statistically compared. The results are summarized in Table 3.
4.1 Effects of VR Experience
As shown in Table 3, participants who were provided with the VR experience during the study period reported the following changes: improved overall perceived health, improved perceived social well-being, decreased experience of negative affects, being less reserved, being more relaxed and outgoing, being less likely to find fault with others, being better at handling stress, being less likely to show signs of depression, and feeling isolated less often. While most of these changes were not statistically significant, the overall trend showed a shift in a positive direction.
Participants’ evaluations of the VR system also improved after the study period. While participants were generally satisfied with the VR system at the first introduction (average score of 6.13 on a 10-point scale), the likelihood of using one (average score: 4.96) and recommending it to others (average score: 4.39) were low. These scores increased following the two-week intervention. After the study period, participants indicated that they were more satisfied (average score: 6.74), more likely to use one (average score: 5.52) and more likely to recommend one to others (average score: 5.39).
4.2 Comparison to the Control Group
The control group that viewed the same contents on a TV during the study period also showed few positive changes. They reported increased frequency of positive affects, being better at handling stress, and being less likely to feel lack of companionship. However, most of these changes were not statistically significant. Also, negative changes, although insignificant and possibly random, were reported for more measures including life satisfaction, overall perceived health and well-being, effects of health on social interactions, personality, depression and social isolation.
For the control group, participants’ satisfaction with the TV viewing experience did not change over the course of two weeks. While participants in the control also reported being more likely to use and recommend the system that they have experienced during the study period, the differences in scores were smaller and less significant compared to the experimental group that were given VR systems.
Additionally, an independent samples t-test was carried out to compare the post-study scores between the two groups. Results are summarized in Table 4.
As shown in Table 4, participants in the VR condition rated their perceived well-being to be generally higher compared to those in the TV group. Of these measures, the average scores for overall perceived health and perceived physical well-being were significant higher for the VR group than the TV group. Participants in the VR group also reported their health less interfering with their social lives, and feeling positive affects more and negative affects less than the VR group on average, although the differences were not statistically significant. Participants in the VR condition also reported being less likely to show signs of depression and feeling less socially isolated compared to the TV group. In terms of their evaluations of the systems that they were given, the VR group was significantly more satisfied than the TV group. Those in the VR group were also indicated that they would be more likely to use the system that they have experienced (significant at confidence level α = 0.1), and more likely to recommend others to use the system (not statistically significant) than those who used TV intervention.
5 Discussion and Conclusion
Technologies have the potential to get older adults more socially engaged and to improve their overall well-being. Also, new technologies including virtual reality (VR) applications have been increasingly gaining interest as they show possibilities for impacting human behavior and improving cognitive health. However, use of VR applications for improving the emotional and social well-being remains an area to be explored.
This study focused on understanding the potential effects of using VR on social and emotional well-being of older adults, especially those living in assisted living communities with limited social activities. A field study was conducted with 35 older adults in the VR condition and 28 older adults in a control condition that used TV. Both groups were shown the same contents related to travel, relaxation and familiar places through the given platform. Participants engaged in the intervention for two weeks, and feedback was collected before and after the intervention using a questionnaire.
Results showed that the VR intervention had overall positive effects on participants’ social and emotional well-being. Compared to the control group, those that interacted with the VR system were more likely to feel good about their own health, more likely to feel positive emotions, less likely to be depressed, and less likely to feel socially isolated. Participants in the VR group also reported being more satisfied with and accepting of the technology and its contents compared to the control group. While not all the differences were statistically significant, the overall trend in the findings show possibilities for use of VR applications for improving the quality of life among older adults.
This study was limited to older adults living in selected sites of an assisted living community, and the sample was geographically limited. In order to better understand the generalizability of the findings, future research can be developed in the following directions: (1) evaluating system effects with a larger, geographically dispersed and demographically balanced sample; (2) including older adults living independently in the general community; and (3) obtaining a random sample of older adults. As more VR applications become increasingly available, evaluation of related systems and technologies for improving quality of life will need to be continued.
References
Harris-Kojetin, L., Sengupta, M., Park-Lee, E., Valverde, R.: Long-term care services in the United States: 2013 overview. U.S. Department of Health and Human Services, Washington, DC (2013)
Cotten, S.R., Anderson, W.A., McCullough, B.M.: Impact of internet use on loneliness and contact with others among older adults: cross-sectional analysis. J. Med. Internet Res. 15(2), e39 (2013)
Miyazaki, M., Sano, M., Naemura, M., Sumiyoshi, H., Mitsuya, S., Fujii, A.: A social TV system for the senior community: Stimulating elderly communication using information and communications technology. In: 16th International Conference on Network-Based Information Systems (NBiS), pp. 422–427. IEEE, New York (2013)
Chao, Y.Y., Scherer, Y.K., Montgomery, C.A.: Effects of using Nintendo Wii™ exergames in older adults: a review of the literature. J. Aging Health 27(3), 379–402 (2015)
Burmeister, O.K., Bernoth, M., Dietsch, E., Cleary, M.: Enhancing connectedness through peer training for community-dwelling older people: A person centred approach. Issues Ment. Health Nurs. 37(6), 406–411 (2016)
Lombard, M., Ditton, T.: At the heart of it all: The concept of presence. J. Comput. Mediat. Commun. 3(2) (1997)
Optale, G., Urgesi, C., Busato, V., Marin, S., Piron, L., Priftis, K., Gamberini, L., Capodieci, S., Bordin, A.: Controlling memory impairment in elderly adults using virtual reality memory training: a randomized controlled pilot study. Neurorehabil. Neural Repair 24(4), 348–357 (2010)
García-Betances, R.I., Jiménez-Mixco, V., Arredondo, M.T., Cabrera-Umpiérrez, M.F.: Using virtual reality for cognitive training of the elderly. Am. J. Alzheimer’s Dis. Other Dement. 30(1), 49–54 (2015)
Falconer, C., Rovira, A., King, J., Gilbert, P., Antley, A., Fearon, P., Ralph, N., Slater, M., Brewin, C.: Embodying self-compassion within virtual reality and its effects on patients with depression. Br. J. Psychiatry Open 2(1), 74–80 (2016)
Chao, Y.Y., Scherer, Y.K., Wu, Y.W., Lucke, K.T., Montgomery, C.A.: The feasibility of an intervention combining self-efficacy theory and Wii Fit exergames in assisted living residents: A pilot study. Geriatr. Nurs. 34(5), 377–382 (2013)
Rosenberg, R.S., Baughman, S.L., Bailenson, J.N.: Virtual superheroes: using superpowers in virtual reality to encourage prosocial behavior. PLoS One 8(1), e55003 (2013)
Mackinnon, A., Jorm, A.F., Christensen, H., Korten, A.E., Jacomb, P.A., Rodgers, B.: A short form of the positive and negative affect schedule: evaluation of factorial validity and invariance across demographic variables in a community sample. Personal. Individ. Differ. 27(3), 405–416 (1999)
Rammstedt, B., John, O.: Measuring personality in one minute or less: a 10-item short version of the big five inventory in English and German. J. Res. Pers. 41, 203–212 (2007)
Yesavage, J.A., Sheikh, J.I.: Geriatric depression scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. J. Aging Ment. Health 5(1–2), 165–173 (1986)
Acknowledgment
The authors would like to thank Tom Grape, and the residents and staff at Benchmark Senior Living communities for participation and support.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Lin, C.X., Lee, C., Lally, D., Coughlin, J.F. (2018). Impact of Virtual Reality (VR) Experience on Older Adults’ Well-Being. In: Zhou, J., Salvendy, G. (eds) Human Aspects of IT for the Aged Population. Applications in Health, Assistance, and Entertainment. ITAP 2018. Lecture Notes in Computer Science(), vol 10927. Springer, Cham. https://doi.org/10.1007/978-3-319-92037-5_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-92037-5_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-92036-8
Online ISBN: 978-3-319-92037-5
eBook Packages: Computer ScienceComputer Science (R0)