
Abstract
This chapter focuses on the “Vivre-Leben-Vivere” (VLV) research and explains how the team in charge has dealt with the issue of representing old people in Switzerland and the vulnerable persons within this population. For this purpose, we draw inspiration from the “total survey error” perspective and discuss the procedures that were used to collect the information, but also the quality of the information itself. We present some of VLV’s methodological choices, such as the contact procedures that were designed to “capture” the most vulnerable individuals, especially in a context where refusal rates for participation in surveys are increasing. We also consider the missing values in responses to some “complex” topics. Results show that participation rates are highly related to the effort that was made in order to recruit the individuals. This is critical for the VLV project, where people can show different degrees of vulnerability related to age, health, and/or poverty. In this sense, efforts such as repeated calls, home visits, and the proxy procedure were successful both in a general perspective and more specifically for a fair inclusion of vulnerable persons in the survey. At the same time, the non-response rates show to what extent it is difficult to explain the personal decision not to respond to a survey or to a question. We can find some traces of “interviewer effects” in the analysis of item non-responses, which we have done by using a logistic regression for one of the psychological tests included in VLV. Some aspects relate to interviewer and respondent characteristics, but others relate to the interview context, all highlighting the complex social interactions at stake.
This paper has been made possible by the support of the Sinergia project, n° CRSII1_129922/1 and the IP 13 of the National Centre of Competences in Research “LIVES—Overcoming Vulnerability: Life course perspectives,” both financed by the Swiss Science Foundation (SNF). The authors express their gratitude to the SNF. They are also happy to acknowledge the support of Pro Senectute Schweiz as well as the universities of Geneva and Bern.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
1 Surveying the Elderly, Surveying Vulnerability
As its title suggests, this chapter takes inspiration from the literature on survey methodology, including the “total survey error” framework, and mainly deals with the different dimensions of its first component, which is the challenge of accurately representing a given population (Groves and Lyberg 2010, 856). The second component, minimizing the measurement errors, will only be touched briefly. Consequently, this contribution is about issues like coverage error, unit and item non-responses, and influences of the questionnaire design, of contact procedures, of interviewers’ and respondents’ characteristics and their interactions on response. They are crucial to dealing with a real challenge: the impact of low and continuously declining rates of participation in large-scale surveys.
Major European comparative research has clearly established the special position of Switzerland, where the rates of refusals of inhabitants to participate in surveys are among the highest in Europe. By using the calculation standards of the American Association for Public Opinion Research, Table 1 shows that in the SHARE survey (Survey on Health, Ageing and Retirement in Europe), during the 2004 round, the acceptance rate varied from a maximum of 69 % in France to a minimum of 33 % in Switzerland (De Luca and Peracchi 2005, 90). The results for the European Social Survey the same year are similar although a bit better everywhere. Moreover, in most developed countries the trend in participation is declining (Rindfuss et al. 2015; Groves 2011). In Switzerland, more specifically in the cantons of Geneva and Valais, where surveys about living conditions among the elderly were done successively in 1979 and 1994 (see Betemps et al. 1997); then in 2011/2012, we observe a dramatic change: the refusal rate grew from 25 to 37 %, then to 47 %.
As we see from this evidence, participation has been decreasing in the long run and is especially low in studies about older adults as well as in Switzerland. It has already had a lot of effects on the costs of survey operations, an issue which is not trivial at all. Moreover, regardless of the studied population, the scientific implications are also of the utmost importance. Indeed, it is well known that standard procedures tend to over represent middle-class participants and to exclude people from the lower classes, who are more likely to not understand or not adhere to the survey project (Groves and Couper 1998). The problem is even bigger with the so-called “hard-to-reach,” “hard-to-survey” groups (see Marpsat and Razafindratsima 2010; Tourangeau et al. 2014). So, all the individuals that could be labelled as vulnerable are disproportionately at risk of being missed. And low, decreasing rates of participation should increase those selective processes (Lessler and Kalsbeck 1992). Non-response is a particular challenge when surveying people affected by economic hardship, health problems, or life accidents.
The following sections of this chapter show how we have coped with this challenge in a survey named VLV (acronym of Vivre-Leben-Vivere, meaning “to live” in the three main languages of Switzerland) and devoted to the health and living conditions of the elderly in Switzerland. Our team conceived and managed this data collection in 2011 and 2012. First some design choices are discussed, including how the questionnaires were constructed and how some questions were designed to identify both latent and manifest states of vulnerability among the participants. We follow with the contact strategy before studying the reasons for refusal. Then we show that some procedures have been efficient in terms of including vulnerable persons in the sample of participants and have reduced the potential bias that would have been associated with a higher rate of refusal by the vulnerable. We also address this question through a comparison of the prevalence of poverty and health problems’ in VLV and in the literature, and in other surveys. At this stage, from the response units we move to the response items; more precisely the non-response, the questions participants did not want to answer. The explanatory logic differs depending on the two modes of data collection that were used on the survey: the self-administered and the face-to-face questionnaires. For the former, we provide a full analysis to identify points of misunderstanding or reluctance to respond. For the latter, we consider two significant variables, household income and psychometric tests of cognitive abilities, in a model that takes into account interviewer and respondent characteristics as well as the context of the interview. A final discussion concludes.
2 Design Choices
2.1 VLV Objectives
The VLV research objective is to explore well-being among the elderly and the conditions for its maintenance throughout the ageing process. From a theoretical point of view, those conditions are constructed all along the life course, beginning early in life with a later accentuation of initial inequalities through processes of accumulation of advantages or disadvantages (Dannefer 2003) or under the impact of critical events (Bak and Larsen 2014). It is to capture those life course dynamics that life calendars have been implemented in VLV. This tool is discussed in this volume in the chapter of Davide Morselli and colleagues. Life trajectories result in a system of resources the aged person has at his or her disposal for ageing. The survey has to identify health, personality, cognition, social and human capital, lodging conditions, income, and wealth, which are some of those many resources. But to be effective, resources need to be used since it often happens that people do not make use of the assets they have. That is why we also surveyed the various practices of the elderly, especially social participation (Bickel 2014). In case of a deficit of crucial resources, in a society like Switzerland, the family and the welfare institutions are supposed to compensate, to take care. Their actions consequently need to be documented too, but from the point of view of the aged person who receives the care (Masotti and Oris 2015). Similarly, the final judgment can only come directly from the men and women themselves, who are the only ones who can tell us about their subjective well-being. Many of us define subjective well-being following Amartya Sen and his famous statement, “to lead the kind of lives they value—and have reason to value” (Sen 1999, 18). Psychologists of course have different references and make a distinction between cognitive (Diener et al. 1985) and affective (Girardin et al. 2008) components of well-being.
2.2 Approaching Vulnerability
Vulnerability, a central concept for the research pole LIVES and consequently for VLV too, could indeed be defined as low levels of well-being. However, in the following lines we emphasize another approach, very simple in its principle. We focus on a breakdown of the possible conditions, that is to say, a breakdown that goes beyond the “vulnerable versus invulnerable” dichotomy, which from the outset appeared unrealistic. The basic idea is simply to differentiate visible, evident, or realized situations of vulnerability from states of latent vulnerability, which are trickier to detect and assess but which are absolutely crucial for any policy, since it is there that useful measures of prevention can be applied. These latent conditions are linked to situations similar to those of realized conditions, but the evidence is no longer obvious, though the threat (or exposure to risk) is clearly present.
The above short development conceptualizes what has appeared, in fact, for two or three decades in several fields of study. Indeed, this idea applies to the distinction between poverty and precariousness that has become commonplace in sociology (Paugam 2000). Since we are here dealing with the aged, the field of gerontology sheds even more light. Between autonomy and dependency, the condition of facing “difficulties” is now the subject of a considerable number of studies. It has been developed and theorized through the concept of “frailty”.Footnote 1 Up to a certain point, this is echoed in demography through the notion also named frailty, which describes more generically differential fragilities linked to phenomena of selection, in particular among the survivors, that is to say the aged, especially those of a very advanced age (Vaupel et al. 1979).
To study vulnerability, we cannot remain with simple opposition between, for example, included and excluded persons, autonomous or dependent persons, etc. Adding more modalities, at least one, we must try to identify those who are at risk, we have to recognize that at the bottom of the scale but above obvious conditions, there is an ambiguous area that must be considered. As soon as it is accepted, the issue of choosing a “border”, as with the definition of a threshold of poverty, becomes less important. Indeed, the border does not become entirely meaningless but much less crucial, since it is no longer a question of “isolating” a subpopulation (of poor people in this example) and comparing it with a global, undifferentiated “remainder.” Concretely, in VLV, a bit <20 % of the participants have monthly incomes of <2400 SFr per individual, which is (almost) the official poverty threshold in Switzerland, but more than 30 % are located in the category just above (2400–3600). Those people are living above the poverty line but are very close and thus are vulnerable to economic stress, meaning they have an increased risk of falling below the threshold should they experience unfavorable circumstances (Gabriel 2015, 117). In his PhD, Rainer Gabriel (2015) considered various explanatory variables or factors associated with poverty, precariousness (the 2400–3600 income category), and the “secured” (3600 and above). Often, but not always, he identifies similar patterns for poor and precarious, such results being instructive for both science and policy.
In the questionnaires used in the VLV survey, tools were systematically selected, sometimes reconsidered, to support an approach that tends to spread the multiple dimensions to be taken into account in the identification and construction of human realities of vulnerabilities. The latter include material difficulties, as we have just seen above, but also health. For instance, Swiss researchers used the test of depression initially developed by Wang and his colleagues in 1975 and proposed a classification where the presence of four symptoms or more indicate a state of depression, while the presence of fewer than two symptoms is an indication of good mental health, and in between they also defined the ambiguous situation of people who are “worried” when two or three symptoms are observed (Lalive d’Epinay and Spini 2008, 90). This example shows that an “obvious” state of vulnerability is time- and context-dependent, since not everywhere is depression socially and institutionally recognized, but what is important here is that the proposed typology includes an intermediate latent state.
In this chapter, we will also illustrate our point by using another scale that is famous in gerontology and also well known to demographers of ageing (Robine and Jagger 2004), that of activities of daily living developed by Sydney Katz and his colleagues (1963). We have opted for the version with five assessments completed for three items on mobility. This tool very concretely indicates whether a given individual autonomously carries out elementary activities of his daily life (such as getting dressed, eating, etc.), whether the person can still do this but with difficulty, or whether, at this very basic level of daily life, he or she has become dependent on external assistance. These measurements, which are, after all, very human measurements of ageing, define in technical terms three statuses of functional health, the first reflecting an absence of vulnerability, the second a latent vulnerability, and the third an obvious one.
2.3 A Context-Dependent Survey
The development of the questionnaires for VLV raised another challenge related to the issue of vulnerability. As it is implicitly said above and has to be made explicit here, the aim was to consider the whole population aged 65 and over, whatever their conditions or characteristics, and to identify the vulnerable persons only in a second stage on the basis of the collected information. This approach reflects changes in gerontological research that have been associated with objective evolutions of life expectancy as well as health and living conditions. The above-mentioned 1979 survey in Geneva and Valais was titled “Isolation and dependency of older people.” On one side, after several governmental reports for which only experts were interrogated, a “knowledge from the bottom,” was finally constructed on the basis of the old persons’ answers. On the other side, such a title expressed the dominant view in the Western world after the Second World War that was still prevalent at the end of the Seventies: a quite negative perception of ageing and of the conditions of the elderly (see Bourdelais 1997). When this survey was repeated in 1994, the title became “The autonomy of elderly persons in their socio-cultural environment,” and the comparison of the two waves revealed a “quiet revolution,” i.e., significant socioeconomic and health improvements (Lalive d’Epinay et al. 2000). Both scientists and the public changed their vision of ageing, but only partially; now there was a distinction between a “third age” of freedom and self-realization versus a “fourth age” marked by senility and dependency, as well as new age stratification like the young-old, old-old, or oldest-old (Dannefer 2001). A research focus on the latter is reflected in the Swiss study of the oldest old that longitudinally followed a sample of octogenarians among the participants of the 1994 survey, and demonstrated that frailty is now, by far, much more the fate of the oldest old than dependency (Lalive d’Epinay and Spini 2008; Guilley and Lalive d’Epinay 2008).
In 2011, VLV considered first the other side of the coin, the young old. The project was named “Old age democratization? Inequalities within progress in Switzerland.” This title expressed the ambition to assess (dis)continuation of the improvements observed in 1979 (see more in Ludwig et al. 2014) and the idea that in a country that has the second- or third-highest life expectancy in the world, even people from the lower classes, with a low level of education, with an immigrant background, etc., are now much more able to reach the age of retirement, and even a very old age, than they were 15 or 30 years ago. This perspective implies that progress indeed produces inequalities in the elderly population; more precisely, we expect a maximal inter-individual variability from retirement until an advanced age, where differential mortality reduces this diversity (Oris and Lerch 2009). This is congruent with our objectives mentioned above and explains our motivation to survey a large and highly heterogeneous population (aged 65–103), our rejection of a vision of all old adults as a vulnerable population, and the need for tools that can assess the variety of health and living conditions experienced within this population. Concretely, it implied applying the same procedures and questionnaires to as many people as possible, without which we would find differential rates of unit response and item response according, for example, to level of education or health status, which would create a biased sample of respondents. The only exception was a specific procedure for persons with cognitive impairments or serious physical problems who did not have the capacity to answer by themselves and had to be included through a proxy, to avoid skewing the results. Otherwise, the same questionnaires were applied to all the participants, regardless of their status or age.
2.4 Questionnaires
Constructing questionnaires is always about playing with constraints to create opportunities. The requirement to be able to study evolution over the last three decades imposed the obligation to keep enough questions from the 1979 to 1994 surveys (Ludwig et al. 2014), but offered the advantage that those old tools usually avoid academic jargon and are easy to understand. In addition, a holistic perspective on ageing implied the mobilization of several disciplinary competencies, which for VLV included geriatrics, psychiatry, psychology, sociology, social policy, and socioeconomics. All the disciplinary demands together imposed difficult challenges, requiring strict selection criteria. Selection criteria included coherence and comparability with other surveys worldwide like SHARE, internal coherence with the general and specific research objectives, interdisciplinary potential, and the desire to not make people feel uncomfortable. Questions on sexuality or tests of psychiatric troubles have been excluded for this reason, though of course those decisions were not undisputed. We reached a compromise between shortening the questionnaires and maintaining a minimal cohesion within the multidisciplinary research team.
The many questions that were left in the questionnaires have been regrouped in thematic chapters (for a description, see Ludwig et al. 2014, and Table 9 and Fig. 7). Following a general model (De Leeuw 2008) that has been applied for SHARE (Börtsch-Supan 2005) and the Berlin Aging Study (Baltes and Mayer 1999), the burden was distributed between a self-administered questionnaire and a standardized interview using the CAPI method. Intimate questions that were selected because of their importance were located in the former and some tests requiring vignettes, exercises and a trained interviewer were located in the latter. Within each questionnaire, the sequence was thought to deal with the old population heterogeneity; asking a question about incontinence to someone aged 67 could seem absurd, but if it is at the end of a series on medical problems the participant can understand the rationale and just answer “no.” Also, some questions, especially some psychological tests where a positive formulation is systematically tested against a negative one, could appear heavy or boring and had to be alternated with more “funny” or attractive questions.
The self-administered questionnaire contained 150 questions and theoretically required one to one and a half hours to be properly filled out by the participant. The face-to-face questionnaire contained no <459 questions! Fortunately, they were never all asked, since several filters were used to identify widows or widowers, divorcés, foreigners, and other categories that called for specific sets of questions. Nevertheless, pre-test estimations of 90′–120′ for the interview duration were definitely too optimistic. Considering those lengths, researchers were concerned about the position of “their” questions to avoid loss of attention and non-answers. However, the following analyses will show us that those worries were not justified.
Finally, another problem was translation. We do not evoke here the immigrant oversamples, but the extension of the survey in two German-speaking areas (Bern and Basel) and an Italian-speaking one (Ticino). Running a survey in Switzerland implies a multicultural, multi-linguistic journey with the related challenges of translation validity and result comparability. As far as our central question here (capturing vulnerable persons) is concerned, we used the formal French, Italian, or German and not the dialects; although they are highly popular, especially in the German-speaking part of the country, but they are too diverse. This made the burden for the respondents even higher as standard German often makes the interaction very formal, administrative.
3 Fieldwork
VLV data have been harvested in five cantons representing the linguistic, political, and socioeconomic diversity of Switzerland. The objective was to question 3600 individuals aged 65 and over living in private households or in nursing homes (in Switzerland, “établissement médico-social,” or EMS).
The individuals were randomly selected from the official lists of inhabitants, stratified by sex and according to six age groupsFootnote 2 in each concerned canton in order to ensure the representativeness of our sample within each stratum, but also to have sufficient numbers for each sub-group. Table 2 shows the distributions of the completed interviews.
VLV has been a homemade product not only in its conception but also in its concrete realization. The research team recruited interviewers, organized their training, and supervised the fieldwork from the headquarters in Geneva, with two or three young researchers delegated to each of the five cantons to be in charge of the daily management of a little enterprise, attributing the sample units, controlling the quality of the work done by the employees, saving and transferring the various collected data, etc. This decision not to outsource to a private company was rooted in a tradition and justified with three reasons. Indeed, the 1979 and 1994 surveys were done the same way with approximately the same justifications: transparency, costs, and ideology. First, the idea was to keep complete control over the entire process of data collection from the first to the final stages. The statistics shown in this chapter are byproducts of this will. Second, it is likely that outsourcing would have been more costly, as will be illustrated through the insistence strategy discussed below. Third, from 1979 until now it has always been the fundamental choice of the teams to refuse the distinction between the “noble” intellectual stages of research and the “lowest” ones, those stages concerning the hands-on technical and logistic aspects of carrying out a survey (see Bétemps et al. 1997; Nicolet and Oris (forthcoming). Simply said, managing an in-house survey is carried by the belief that researchers should not limit themselves to analyzing and theorizing about social science data; they should also go out and get their hands dirty while collecting it.
In the following, we discuss the survey procedures and contact strategy, the coverage errors, the refusals and their causes, and to what extent the procedures and their adaptations were efficient to “capture” vulnerable persons in the sample of participants, and we conclude with a comparison of the prevalence of socioeconomic and health vulnerability in VLV and in other data sources.
3.1 Procedures and Contact Strategy
To ensure data quality, a clear approach procedure that could be translated into the three languages was put together. The procedure took into consideration a number of situations that the interviewers would encounter:
-
EgoFootnote 3 is apt (has the capacity to answer) and lives at home;
-
Ego is apt and lives in a nursing home;
-
Ego is unapt (at home or in a nursing home);
-
Ego does not speak French, German, or Italian.
Before the procedure was launched, the sample members had to be allocated to the interviewers. For that purpose, the interviewers were given contact sheets that contained confidential information concerning ego (surname, forename, address, and phone number). The interviewers had to indicate each contact attempt, the date, whether there had been a visit or phone call, with whom the interviewer had spoken, the result, and in the case of a refusal, the reason(s) (Fig. 1).

Approach procedure
The most concrete aspect of the approach procedure was making contact. The two first stages were common to all procedures, with small variations. First, ego received a leaflet presenting the study and a personalized contact letter announcing that an interviewer would phone. In the event that the respondent lived in a nursing home, the first letter was sent to the nursing home direction to inform that one of their residents had been selected to take part in the VLV survey and that an interviewer would contact the management before any other step was taken.
The question arose of which was the best solution for the first contact with ego: to phone or to make a visit at home? For the entire survey with its five regional fields, our team decided on an initial phone contact to ensure the best comparability with the 1994 survey and for other very pragmatic reasons. In some cantons, the distances to be covered for each visit, especially if ego was living in a mountain village, could be long. This would have led to a substantial increase in the costs and would also have increased the time devoted to the survey by the interviewer who would have been reluctant to make such an effort with uncertain rewards.
A home visit was done in only two cases: firstly, when ego had no phone number and, secondly, when ego could not be contacted by phone for 2 weeks. It emerged that 5–26 % of elderly people do not have a phone number indicated in public phone directories, the proportion reaching its maximum in villages in the mountains of Valais, Ticino, and Bern Oberland. In Switzerland, for a population of eight million inhabitants, some four million phone solicitations are made each year for surveys, very often for marketing purposes. Combined with aggressive selling and the increased use of mobile phones, this creates an increasingly difficult environment for scientific surveys (Joye et al. 2012). In this respect, the initial letter was crucial in allaying certain fears.
When contact was made with ego, the interviewer could have been confronted with two situations: the person was apt, i.e. able to answer, and could therefore decide whether he or she agreed or refused to participate in the study, or ego was non-apt. During the phone call, the interviewer could already be able to detect whether ego had cognitive problems by asking simple spatial orientation or temporal questions:
-
“Could you suggest a date for the appointment?”
-
“Is there an entry code for where you live?”
-
“Could you explain how to get to where you live?”
-
“Could you remind me of your address?”
If ego appeared not to have the capacity to answer, the interviewer had to activate the so-called proxy procedure, asking the assistance of a close friend, relative, or caregiver to answer a short questionnaire of some 60 questions. Similarly, if ego was living in a nursing home, when the interviewer contacted the management, he or she would obtain information on ego’s health, that is to say his or her ability to participate in the survey. If the reply was affirmative, a first contact letter was sent to ego to provide the person, just as the other sample members, with information on VLV and to allow him or her to express informed acceptance or refusal to take part. Otherwise, the proxy procedure was applied.
If ego was no able to answer, it was rare that the person could be directly contacted, but contact was made with a spouse, family member, guardian, or the nursing home. In such a case, the interviewer would suggest to one of the aforesaid to participate in the survey by replying to a limited number of questions on ego. This “proxy” procedure, as indicated above, was initially the only procedure to diverge from the standard one. It was essential to avoid the trap, still too frequent in gerontology surveys, of not gathering data on individuals who are in very bad physical health and/or suffering from cognitive problems. It was all the more crucial to ensure correct comparability with the 1994 survey, since the weight of diseases such as Parkinson’s or Alzheimer’s has constantly increased in the causes of death of the very old (80 years and more), in Switzerland as elsewhere (Berrut and Junker 2008). This procedure allowed us to interview 555 close friends, relatives, or caregivers, which represents somewhat more than 15 % of all the interviews collected (Table 3). Without this special procedure and its adapted questionnaire, an entire segment of the population would have been excluded and the sample of respondents seriously biased.
In the framework of the standard procedure, once contact had been made with ego or a proxy, several situations could arise:
-
1.
Ego had died. The file was then closed for reason of death;
-
2.
Ego was no longer living in the same place, with three possible situations:
-
Ego had moved outside the territory concerned by the survey; his or her file was closed under the category “no reply” (NR),
-
Ego had moved but had remained in the area of the survey; the first letter was forwarded to the new address,
-
Ego had moved into a nursing home; the contact letter was sent to the director of the nursing home,
-
-
3.
Ego had not received the first letter, so it therefore had to be sent again and ego had to be called a few days later;
-
4.
Ego had received the letter.
When the interviewer was finally in situation 4, he/she was faced by one of three situations:
-
(a)
Ego refused. The file was closed due to refusal;
-
(b)
Ego hesitated and wished to see the questionnaire before deciding;
-
(c)
Ego accepted and an appointment was made with the interviewer.
In cases b and c, a second letter was sent to ego. It contained:
-
the self-administered questionnaire (SAQ)
-
the personalized life history calendar (LHC)
-
the information leaflet explaining in greater detail the survey and the confidentiality of personal data
-
If an appointment was made, a letter of confirmation was sent.
Following the second letter, ego may:
-
refuse by calling the interviewer or the cantonal office;
-
in situation b, accept and set up an appointment with the interviewer.
3.2 Coverage Errors and Mistakes in the Samples
Figure 2 shows the concrete results of the procedures described above. We will discuss the refusals in the next section. Here, we deal with the coverage errors that affected no <13 % of the original sample.

Distribution of the four types of individual outcomes, VLV, five cantons, 2011
People who cannot be found at the address provided by the cantonal and federal population or statistical offices reflect discrepancies between the target population and the sampling frame. These problems can be explained by the length of the VLV field and consequently a growing temporal duration between the samples extracted from the lists of inhabitants, but also because the latter are theoretically updated every 3 months, and obviously less often in some municipalities. Other discrepancies are due to the very nature of ageing, such as risks of dying or moving to an institution between the date of the population enumeration and the date of a contact attempt by a VLV collaborator.
On the ground, it was decided that a home visit would be a last resort when unable to contact ego by telephone. Therefore, if there was no phone number and no reply after 2 weeks, the interviewer contacted the relevant commune (municipality) to find out whether ego was still living in the same place, had moved or had died. The communes and post offices (sometimes the priests also, and neighbors) proved to be very helpful throughout the data collection stage. Another source of coverage error appeared during the fieldwork. In Geneva, it happens that people have a postal box in the canton but in reality live in France, the former being their formal address, explaining why they were on the lists of inhabitants and were included in our sample. This comes from a law regarding civil servants that was abrogated some years ago, but the practice survived. In Valais, several persons have their formal residence in a chalet in the mountains while it is in fact a secondary residence. Usually this is for fiscal purposes. At the end, in 14.1 % of the 4105 files opened in Geneva and Valais, it was impossible to make contact with the person. For the five cantons altogether, 10 % of the files were in this situation, which is a bit less than the average proportion observed in European countries in the 2004 round of the Survey on Health, Ageing and Retirement (De Luca and Peracchi 2005, 94).
Those cases were costly in terms of management time. From the attribution of the contact sheet to the interviewer to the transfer of the complete interview to the headquarters, it took on average some 40 days for a full participation in the survey; the length was 60 days in cases of non-contact (NR in Fig. 2), to harvest nothing at the end. It was consequently also very negative for the motivation of the interviewers who had to deal with those cases.
3.3 Many Refusals
Figure 2 shows that we ended with 54 % refusals against 33 % acceptances. For Groves and Couper (1998), individuals who refuse to take part in a survey are more likely to be uninterested in the topics of the survey; not have the time; or find it difficult to understand the language of the questionnaire, which would indicate a low level of education, or different origins and partial learning of the host society’s language, or both. Analysis of the reasons for refusals bears out their first judgments (see Fig. 3, which reports the percentage of men and women citing each reason). For Geneva and Valais in 2011, the refusals “without reason” dominated, but among those who gave some justification, a lack of interest was top of the list, which justified more than one refusal in five. This was followed by health problems, being “too tired,” or being “too old,” with around 14 %; and inversely, being too busy with 8/9 %. Personal and family reasons, which often expressed a desire to protect one’s intimacy, varied between 6 and 8 %; and a clear rejection of surveys (“I don’t want to be a guinea pig”) was manifested by 7/8 %. Men were somewhat more likely to refuse without explanation, while women more frequently indicated their absence of interest or desire. Globally, however, an obvious gender pattern does not emerge.

Reasons for refusal to participate in the VLV survey, by sex, Geneva–Valais, 2011
As we can see in Table 4, the two main causes are not particularly affected by age, but among the oldest old, 31 % of the nonagenarians refused without explanation. As we could expect, health problems or feeling tired or too old is a reason that increases with age. Personal and family reasons show the same pattern, being a marginal factor among those aged 65–69, then growing in importance. Protecting intimacy is more of a concern for the oldest old. Interestingly, the rejection of the survey appears as more “modern”; it is more of a reason in the recent cohorts that in the older ones. Refusing “to be a guinea pig” and similar expressions reached 11 % among the 65–69 cohort and then continuously fall to 4 % among those aged 90 and more. As we could expect, being busy with work, holidays, or other activities was also important among those who had just retired and strongly decreased, becoming marginal from the age of 80.
This issue is crucial, since the credibility—and consequently, the survival—of surveys as a tool for the social sciences seems to be engaged when so many potential participants refuse to contribute. However, it is difficult to go deeper into this issue right now, because we know very little about these persons, aside from the little data provided by the administrative files when the samples were delivered. Some logistic regressions on refusals and acceptances, respectively, are not shown because they only brought limited additional information: higher participation of men and people living in urban areas, and those aged 80–84 showing the lowest propensity to contribute. In terms of interactions, the sex of the interviewer (whatever the sex of the sample member) and his or her age had no impact. While an initial recruitment condition to work for VLV was to have a bachelor’s degree in social sciences (in a broad sense), it appears that the interviewer’s level of education had no effect. Only the interviewer’s accumulated experience increased the probability of obtaining an acceptance from the sample members, but this is a tautological result, since those with few successes were discouraged and gave up.
3.4 Adaptations and the Inclusion of Vulnerable Populations
Faced with so many refusals, the VLV team decided against using standard ‘refusal conversion’ efforts (see Groves and Lyberg 2010, 872) for ethical (ideological) reasons. A “no” has to be respected. However, to reduce the number of negative answers as much as possible, we chose to have some interviewers specialize; they were requested to make the first phone contact, not only for themselves but for the entire team. The crucial nature of this first interaction has been studied for some 15 years (see Snijkers et al. 1999; Durrant et al. 2010) and now appears to be an explanation for national variations, as well as being likely to affect the comparability of results (Blom et al. 2011). In our case, certain interviewers clearly proved to be more effective than others in obtaining the cooperation of potential participants. Figure 4 shows the success rates per interviewer in Valais. A similar distribution was observed in the other four cantons. With a large majority of collaborators showing an average level of efficiency, with approximately one in every four being clearly less efficient, several champions emerge. In each field, they became famous as heroes of the survey journey. By distributing the appointments obtained by the more persuasive collaborators throughout the entire team, we managed to prevent any increase in interviewer effect. This is a typical illustration of our initial compromise: combining maximum flexibility to obtain as many acceptances to participate as possible, but applying the same questionnaires and interview mode to all of the participants, apart from those unable to answer, as rigorously as possible.

Rates of acceptance per interviewer, VLV, Valais, 2011
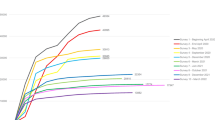
A second strategy was to show endurance and accept large extensions in the duration of the fieldwork. It was our wish to never force an individual to take part in the survey, but also to insist as much as possible until having a clear reply directly from ego. This obstinacy was costly, both in time and money. When the fieldwork was launched, it was estimated that we would need around 3 months per canton to gather the data—in the end, it took us 8 months per canton. Table 5 explains why. In Geneva and Valais, 4105 people were contacted to obtain 1428 acceptances (including both proxies and “normal” interviews). Roughly 25 % of the latter were obtained following five or more attempts to contact ego by phone or by a visit to the home to request his or her agreement. Generally, in surveys repeated calls is a well-known strategy to reduce noncontacts, while home visits are barely part of the procedures. Indeed, Groves and Lyberg (2010, 872) rightly insist on the costs of obstinacy. Take the example of a car drive through a mountain village with uncertain results. However, without those home visits and knocking directly on the door of ego, we would have lost almost 8 % of the final participants, and without calling five times and more (until 23), we would have missed 17 %. The potential related biases are assessed below.
This question of bias is important and less obvious that it seems at first glance. Indeed, if certain sub-populations reply less than others and efforts to increase the general response rate are made without taking this into account, such efforts would potentially result in an increase in the selective bias (Peytchev et al. 2009, 786; Roberts et al. 2014). However, when walking the tightrope between ethical evidence of respect for refusals and the wish to obtain a reply directly from ego, whatever this reply may be, could we consider that our procedures worked? Can we conclude that insistence and recourse to proxies allowed more vulnerable individuals to be included in the survey? Of course, we assume that the risk of capturing too many vulnerable people is illusionary.
To provide initial replies to this question, Figs. 5 and 6 represent the distribution of interviews obtained by age group, for men and for women. By differentiating the different procedures according to age and gender, we are able to conduct a more detailed analysis on the impact of our perseverance. We also take into account the proxies and individuals who were contacted by the standard procedure. We therefore have five categories: 1 or 2 calls to obtain participation, 3 or 4 calls, 5 calls and more, a visit (to ego’s home), and proxy. In addition, Table 6 shows the statuses of functional health and each of the respective depression categories, which in both cases are distributed according to the type of procedure that allowed information to be obtained.

Distribution of respondents by approach procedure and age group, Geneva–Valais, women, 2011

Distribution of respondents by approach procedure and age group, Geneva–Valais, men, 2011
Among the participants, women aged 75–79 and men aged 75–84 were the most difficult to contact by phone. The 75–84 cohort required the heaviest procedure of a home visit most often. An initial explanation is linked to the availability of a phone number. In Valais, we had no phone numbers to contact roughly 22 % of the women in this stratum. Both men and women aged 75–84 were also the groups in which the rates of refusal to participate in the survey were the highest, with reasons that mixed those of the oldest old and the young old (Table 4). Taking into account the evidence collected in another study (Duvoisin et al. 2012), we put forward the hypothesis that a fair proportion of individuals aged 75–84 tend to live their experience of ageing negatively. They are affected by biological changes, realize that their losses exceed their gains, and suffer from this evolution, which leads them to refuse useful offers from associations working for the elderly; similarly, they are also more likely to refuse to participate in a survey “on the old” (Duvoisin et al. 2012). This interpretation requires more research, of course, but all elements at this stage point in this direction. In any event, the complicated and costly procedure of home visits allowed the survey to include relatively isolated individuals in borderline age groups between what is widely referred to as the 3rd and 4th ages, that is to say, between 75 and 84.
In the same order of ideas, repeated phone calls—from 5 to as many as 23—mainly appeared useful for contacting and convincing the “young old,” exactly those whose refusals were largely explained by a lack of time, holidays, or work. This is all coherent, and we must also give credit to obstinacy. Whilst this observation is valid for both sexes, the greatest effort had to be made to reach the men. Participation was obtained after five or more phone calls in around 15 % of the cases, versus a little <9 % among women for this type of recruitment. This originates from two phenomena. One is mechanical, since the number of proxies is lower on the male side (16.5 %, against 21.3 % for women). This confirms the well-known health–gender paradox, according to which women live longer than men but age with worse health (see Van Oyen et al. 2013). Another explanation has more of a psychosocial nature, since experience in the field showed that wives often blocked phone calls, feeling the need to protect their husband (who were generally older than they were) from aggressive phone canvassing or suspected risks of invasion of privacy. This does not emerge very clearly on Fig. 3, for which we wished to avoid overly subjective coding.
The proxy procedure obviously centers on the oldest individuals. Initially, it may appear less heavy than a standard procedure (shorter questionnaire, fewer letters to be sent), but the Valais figure for the time spent on each case shows that this approach required great perseverance to obtain the desired result, since it required just as much time, if not more, depending on the strata. An average of 43 days was needed to close a proxy file for the men, whereas 38 days were needed for a normal procedure. It could take time to discover that ego was non-apt (and/or moved into a nursing home), and contacting a close friend, relative, or caregiver of ego and making an appointment was more complicated than with the retired sample members, since at least 50 % of the proxies had a job.
With Table 6, we touch even more directly the central question: the inclusion of vulnerable people. Whilst we could have hoped that our insistence on contacting the sampled individuals by repeated phone calls would allow us to capture more vulnerable individuals, the results on functional health, in fact, point in the other direction: when we repeatedly insisted on participation by calling repeatedly, there were more independent individuals than those among the files obtained easily (after 1–4 calls), as many people in difficulty, and fewer dependents. This can be explained by what Figs. 5 and 6 showed—that is to say, the relative youth of the respondents recruited in this way. In their case, by seeking out dynamic seniors in this way, we tended to avoid a negative bias that would have underestimated their global good health and numerous activities.
Home visits, on the other hand, allowed significantly more people to be recruited whose functional status was described as “in difficulty,” which can be considered a latent state of vulnerability. But the proxy procedure—although requiring great insistence—turned out to be even more important in accounting for the vulnerable aged than we expected. As a reminder, somewhat less than one file out of six was obtained in this way, but no <70 % of the individuals included in this way were in a situation of dependency.
When we look at the second panel of Table 6, which describes categories of mental health, we find confirmation that repeated calls did not help to capture more vulnerable people, when compared with those whose participation was obtained easily, which already included some 15 % of persons who were depressed but participated anyway. Home visits were once again—and in fact, much more clearly than for functional health—useful for obtaining the contributions of those in a latent state of vulnerability—the “worried”—to the survey. Additionally, the proxy procedure confirmed its usefulness for including people who were obviously vulnerable, with 4 or more symptoms of depression. However, Table 6 also shows a trade-off: in 32 % of the cases, we were not able to establish the category of mental health because of item non-response. Indeed, the questions that constitute the Wang test of psychic health were the only ones about ego’s feelings in the proxy questionnaire, due to the importance of this dimension in any assessment of well-being among the elderly. But we can understand that approximately one in three proxies refused or were unable to guess ego’s pleasure, sadness, etc.
At this stage, it is fair to note that the inclusive approach based on recourse to a proxy was recently criticized. In this critical perspective, an individual whose cognitive capacities have deteriorated should be excluded from the process; indeed, such an individual cannot really give his or her informed consent and someone who ego has not necessarily designated replies to questions concerning ego. Depending on how close this person is to ego, the social situation, socioeconomic status, and, a fortiori, past life of ego will be documented with some degree of uncertainty. It is this “silence by proxy” (Fillit et al. 2010) that is thus being denounced. An answer could be that the absence of impaired elderly in the survey, the scientific results, and ultimately the citizen debates about the social and political management of ageing would be another form of highly negative silence. At the same time, the ethical question, i.e. the point at which the individual’s consent was informed, cannot just be rejected.Footnote 4 We face here a real tension.
3.5 Prevalence of Vulnerabilities in VLV and Other Data Sources
To the instructive but indirect evidence discussed above, this section adds the results of a benchmark approach, comparing the prevalence of forms of vulnerability in the VLV’s final sample of respondents with the numbers that can be found in other data sources.
Being poor is an obvious state of vulnerability, since the poverty line is fixed by a confederation of Swiss institutions of social help and applied all across the country. This threshold is set at a monthly income of 2450 SFr. per person. In VLV, we used 2400 to simplify, and the poverty rate in the sample reached 17.9 % for men and 23.3 % for women.Table 7 offers a comparison with four other studies. Variations can generally be explained with the use of different sources, definitions, and temporal differences. However, between the SILC use of the 60 % median income level and the SKOS/CSIAS (2013) threshold, the difference is marginal (2450 versus 2500 SFr. in 2012). It can also be pointed out that there is no significant evidence that the “Great Recession” from 2008 has affected the economic well-being of the Swiss elderly, as it did in many other European countries (Cavasso and Weber 2014). Globally, we can conclude that VLV faced the challenge of fair inclusion of the poor in the survey with success.
For functional health, the VLV estimates can be compared with two recent reports from the Swiss Federal Statistical Office on the elderly living in private households (Bundesamt für Statistik [OFS/BFS] 2014) and in institutions (Bundesamt für Statistik 2012). According to the findings of the VLV survey, 86.9 % of people aged 65 and more were found to be independent, as opposed to the 91 % claimed by the first OFS/BFS study. Moreover, VLV estimates that 6.9 % of elderly people are in a situation of difficulty, meaning that they are generally able to accomplish all activities of daily living themselves but uneasily for at least one of them. Additionally, an estimated 6.1 % are no longer capable of performing their daily activities independently, meaning that they require external help with at least one activity. Contrasting these results, the BFS/OFS report found 7 % of elderly people in Switzerland with difficultiesFootnote 5 and 2 % being completely dependent. Based on the comparison with this first report, VLV seems to have slightly over-reported the prevalence of dependence in the population. The differences between the VLV data and the aforementioned report, however, are most likely due to differences in their samples: whereas VLV also included people living in nursing-homes, the OFS/BFS study exclusively considered those living in private households.
In the second report that focused exclusively on elderly people living in care institutions (Bundesamt für Statistik 2012) the numbers change drastically: 96 % of individuals were found to have trouble accomplishing at least 1 activity of daily living; thus, only 4 % of individuals were completely independent. The analysis was restricted to a population that was no longer living in their own households due to the importance of their restrictions in managing their daily lives, which explains these very high percentages. Given these two selective and therefore biased sources, however, it seems plausible that VLV generally captured a relatively representative sample of the general population, in terms of functional health, especially thanks to the proxy procedure.
Finally, comparing the mental health findings in VLV with those from other sources was not a straightforward task, since there are many indicators to measure depressive symptoms, different classifications to determine the actual categories and statuses of psychic health or to measure the intensity of depressive disturbances, and generally very little research on the topic of elderly people with depression. A relatively exhaustive report on depression among the Swiss population by the Swiss Health Observatory (OBSAM) estimated the prevalence of depressive symptoms among the elderly population (Baer et al. 2013). The results are summarized and contrasted with VLV figures in Table 8.
Despite the cautiousness needed when comparing these findings, it can be seen that depression was reported more often in the VLV data. Both studies found that roughly 75 % of the population was free from any symptoms of depression in the 65–74 age group. VLV, however, lowered the estimation of persons with minor signs of depression and suggested that there were more than three times as many people suffering from intermediary to strong depressive symptoms in this age group, compared to the OBSAN report. Among those aged 75 or higher, individuals who are not vulnerable or in a latent state of vulnerability were proportionally less represented in the VLV data, where we once again find much higher estimates for people who were obviously vulnerable, from a mental health point of view.
The challenge was to avoid or at least limit the risk of differential rates of answers between vulnerable and secure sample members leading to the exclusion of the former. Although the rate of participation for VLV was low and although it is not really possible to provide a strict, definite answer with the comparisons discussed above, all of the evidence is clearly positive and suggests a fair inclusion of the vulnerable elderly in the survey.
4 Responses and Non-response in the Questionnaires
The last part of this chapter considers item non-response, revealing questions that participants were unable to understand or that made them uncomfortable, if not reluctant to answer. In this perspective, we assume that non-answers are not equally distributed among the participants and could reflect vulnerabilities. Since we are not intrinsically vulnerable but vulnerable to something, through an analysis of non-response, we have a chance to identify some perturbing factors that have affected VLV respondents and could ultimately affect the validity of the measures based on this material (Groves and Lyberg 2010, 856).
Concretely, in the VLV leaflets as well as at the beginning of the interview, the participants were instructed that they could refuse to answer at any time, without justification, and move to the next question, or interrupt the process and renounce their participation.Footnote 6 Of course, the use of this freedom does not adhere to the same logic when the old person is confronted with the self-administered questionnaire, what it means with him- or herself, compared with the face-to-face interaction with the interviewer. This is why we made a distinction between the two tools in the following, starting with a section on item non-responses in the first questionnaire, based on a systematic analysis. Then, we follow with a second section on two non-representative but especially eloquent cases of delicate information collected during the interview: household monthly incomes and the results of the cognition tests.
4.1 Non-responses in the Self-Administered Questionnaire
Table 9 shows the various thematic chapters in their order of appearance in the questionnaire. For the 3080 participants (proxy questionnaires excluded), non-responses represented an average of 11 %, but with a large variability, from 2 %, for the questions on children, to 27 %, when social life is concerned. Coming back to points that have been discussed at the beginning of this chapter, we did not observe a direct effect of the length of the questionnaire. We made the bet that locating the “health and medical problems” topic at the very end would provoke renewed attention, since it is an important concern for the elderly, and it seemed to have worked. Otherwise, the vision offered by Table 9 is too vague. It is clear that the probability of non-response is associated with some thematic chapters, but it does not suggest obvious explanations. To take further steps, we need to look at Fig. 7, which shows the distribution the item nonresponse rate across the 150 questions.

Distribution of non-response in the VLV self-administered questionnaire
Generally, the average is artificially increased, since peaks of non-response are observed for the item “other(s)” all along the questionnaire, concluding long lists of possible answers. While it is easy to understand why the survey designers systematically included this option, many participants obviously did not understand the rationale of choosing this modality. Similarly but also differently, long, repetitive series of items produced misunderstandings. This happened in the “social life” chapter, in which the participants were asked if they were currently members of an association or not and were confronted with a list of 14 items.Footnote 7 Moreover, for obvious reasons of memory mobilization, the same list was asked just afterwards but concerning membership at the age of 45. Several checks showed that older participants ticked off the types of associations that they were or had been members of, but not the others, with an absence of responses meaning “no.” Such behavior explains the high values in the “social life” chapter but also appears all across the self-administered questionnaire from time to time. Significantly, this behavior is not associated with the sex or age of the respondent.
Another logic emerges in chapters E and F on lodging and media, respectively. Indeed, non-responses are concentrated on specific technologies like microwaves, remote alarm, computers, and the Internet. Not surprisingly, this is associated with a strong age effect. It reflects a dis-adjustment process to recent technologies among the oldest old, who do not answer questions they do not understand.
The non-answers in the chapter on “care” call upon all the explanations discussed above. There are relatively moderate (12–16 %), but the value for the “other” item explodes to 43 %. This is a more frequent pattern among the oldest old, who are the more frequent users of care, by far, but who are confronted with a list of various caregivers and another list of various types of help and tick off only positive answers, leaving the unused responses blank.
Finally, people generally answered when asked to express their opinions, although some questions provoked a significant rate of non-response (10–15 %) and a few were rejected by 16–20 % of the participants. A more careful look shows that the second and third categories contain questions formulated in an impersonal way. Instead of engaging the surveyed person directly, they are of a general nature. For example, “Do you agree with the following sentences? ‘Hard blows hurt people by chance.’ ‘Human nature is fundamentally good,’” etc. A fair proportion of the respondents felt unable to take a position and/or did not understand the rationale of such questions. Significantly, those questions were the only ones with significant percentages of non-valid answers (in most of the cases because two modalities of answers were ticked off, instead of only one). When financial issues are concerned,Footnote 8 the rates of non-response grew further still and women were more likely to refuse.
4.2 Non-response in the Face-to-Face Interview
We find a similar pattern when we move to questionnaire 2, which was administered during a face-to-face interview, and more specifically for the question on household monthly income. The delicate aspect of interrogating people on their revenues is well-known. In the 1970 survey in Geneva and Valais, this information was missing in 13.9 % of the cases; this proportion grew to 23.9 % in 1994. However, this trend was interrupted, since the figure for 2011/2012 is 14 % for the two same cantons, and 15 % when we consider the five cantons of the full VLV survey (Gabriel 2015). The participants were not asked to provide a number but just to make a choice between nine categories.Footnote 9 This approach was explicitly chosen to make the respondents’ job easier and increase the answer rate. Generally, people do not answer such questions because they do not want to, but also because they do not know. To go deeper, Table 10 provides the results of a logistic regression on non-response to monthly household income.
First, women had a 51 % higher probability of not answering the question on household monthly income, compared to men, and the oldest old were also much more prone to missing this information. The odd ratios were significantly higher from the age of 80 and continuously increased until reaching 2.29 among the nonagenarians, with 65–69 being the reference category. As far as those demographic groups are concerned, VLV is not different from other surveys in Europe and North America (Groves and Couper 1998; Malter 2013). More specific but difficult to interpret, the participants were more likely to give this information in the canton of Bern, where the poverty rate is low, and were much less likely to do so in the canton of Ticino, where the poverty rate is the highest. More conclusive are the results about education, which proved to be a robust indicator of social class (Gabriel 2015), largely predicting poverty in old age (Gabriel et al. 2015). Compared to those with apprenticeships, which is the reference group and also the largest group, people with low education had a similar probability of giving information on the revenues on their revenues. However, persons with superior diplomas were almost 60 % more likely to refuse to give an indication, even though they quite probably knew their incomes well. While the evidence discussed in the preceding part consistently suggests that poor elderly have been properly included in the VLV survey, we see here that the distribution of non-response cannot result in a measurement error, i.e., in an under-estimation of the socioeconomically vulnerable.
In a second analysis, we consider another crucial dimension that was quite delicate to ask questions about: cognition. It is a key variable when aiming to identify and explain the mechanisms that generate or avoid vulnerability and permit resilience in old age. Cognitive abilities are important resources when coping with developmental tasks and age-related challenges, and have been shown to be a powerful factor that affects successful regulation in the interplay between age, personal, motivational, and social resources, and well-being and functional health (e.g., Baltes and Lang 1993; Köhler et al. 2011). Well-preserved cognitive resources represent a core dimension of well-being and mental health in old age. On the other hand, Lawton et al. (1999) showed that over 60 % of the participants aged 70 and older in a US survey would not wish to live any longer under any condition of cognitive impairment. Cognitive decline was more threatening to older adults’ quality of life than functional impairment or pain. Such fears are both expressed and nourished by the mediatization of the so-called “epidemics” of cognitive impairments, even though Alzheimer’s disease and other diseases sharing the same etiology are not contagious at all. This context makes assessing cognition in large-scale surveys like VLV quite important and delicate at the same time.
To understand the reasons of non-response in the cognition items, we developed a more complete model than that for household incomes. This model indeed takes also the interviewer effect and the context into account.Footnote 10 The premise is that interviews are a complex process of information exchange, in which different elements that could introduce bias into the responses may interfere (Groves et al. 2004). In the existing literature about the interviewer effect, a set of variables is identified that can explain the phenomenon in an operational way and can be categorized into four fields that interfere in the “interviewing act”: (a) aspects related to the interviewer’s characteristics, (b) aspects related to the respondent’s characteristics, (c) the conditions and context of the research, and (d) characteristics related to the research tool (questionnaire). The latter category is mainly related to the questionnaire’s design, clearness of the definitions, terms used, format, etc. Category c) considers the environmental conditions of the interview (e.g., place, presence of other persons), as well as the collection methodology used, the standardization of the interview conditions, the training and supervision of the interviewers, and also the monitoring and observation of these variables by the interviewers and researchers (Durrant et al. 2010; Groves and Lyberg 2010; Marchese 2011; Blom et al. 2011).
The interviewer effect is operationalized for VLV research by three sets of variables regarding the interviewer, respondent, and context, respectively. For the fourth component—the questionnaire—we consider the Trail Making Test (Reitan 1958; Bowie and Harvey 2006), which has two parts: TMT-A, in which the participants are asked to link numbers, and TMT-B, in which the participants have to alternate numbers and letters. More concretely, each participant was asked to complete a short version of the TMT-A as an exercise (and the interviewer noted “fail” or “pass”) and then to pass the full version (the interviewer noted “fail” or “pass” and had to note the duration). Then, the same had to be done for TMT-B. Table 11 simply shows the resulting process of selection. Starting with 3080 participants, 5.1 % refused to complete the first exercise; this initial rejection was the strongest. Only 8, 28, and 10 participants refused at one of the next three steps. While only a small proportion (6 %) failed the TMT-A short or extended and could not continue, the TMT-B appeared to be much harder, with around 30 % failing. Such situations were not uncommon for both the participants and the interviewers. Anecdotally, all of the fieldwork leaders remember collaborators who were all specifically trained but who, after some interviews, expressed concern. Although they explained to the participants that it was not at all a medical examination and that the result was not important, some people who failed were greatly affected and sometimes started to cry. Additionally, the incident with the immigrants is reported in the Kaeser chapter, in this volume. Moreover, we also see on Table 11 that when the test was passed with success, the interviewers forgot to note the duration in no <22 % of the cases for the TMT-A and 5.6 % for the TMT-B. This shows that managing the cognitive tests was also a cognitive exercise for the surveyors, who did not completely deal with the explanations and the interactions with the person, the stopwatch, and the computer.Footnote 11
In Table 12, we analyze the initial refusal through logistic regressions, then the four situations in which participants failed to pass the tests, and finally the two situations in which the interviewer forgot to note the time, all situations described in Table 11. Refusals to complete the cognitive tests were more frequent when the interviewer was experienced. Indeed, this effect suggests that those who had already completed several interviews and faced people who were shocked and/or sad to have failed were not unhappy when a sample member refused to answer their questions and sent implicit messages carrying this feeling. From the respondents’ point of view, older persons and women were more reluctant and more often used their freedom to say “no,” as did people in the French-speaking cantons. Unsurprisingly, depressed persons tended to reject those tests. Inversely, Swiss natives—especially in the German-speaking cantons—were less inclined to refuse; quite obviously, this was also the case for the participants whom the interviewer evaluated as cooperative. Regarding the context, quite expectedly, the interview in the participant’s private lodging was much more favorable to response than when in a tea room or another place.
When we consider the experience of failing, we see a sequence suggesting that the first questions created both a selection and a dynamic. Indeed, for the short and extended versions of the TMT-A, the participant failed more often if the participant was older or, whatever his/her gender, if the participant had to pass the test in front of a young female interviewer. Then, for the TMT-B, the age of the respondent had an impact—which is quite normal—but the impact of the interviewer’s sex disappears, while another characteristic emerges. Indeed, people failed more often when the interviewer was experienced. Once again, this apparently strange result supports the hypothesis of a disaffiliation among the survey collaborators who adhered less and less to those questions. The other protective or risk factors are more obvious (high education, depression, or frailty) and not the topic of this chapter (see Ihle et al. 2015, for an in-depth analysis), but it is worth noting that the context of the interview is not that important by comparison. The presence of another person in the room has a negative effect on the probability of succeeding in the short versions of the TMT-A and TMT-B, but not for the two extended versions.
As we have seen, the situations in which the interviewer forgot to note the time taken by the participant to successfully complete one of the tests were much more frequent for the TMT-A than for the TMT-B, which once again suggests that the collaborator had too many things to manage at the same time and was stressed when reaching this part of the face-to-face questionnaire. The results are somewhat complicated, but three points emerge. First, information on time was more often missing when the interviewer was a woman and older, while interviewers with low level of education more strictly followed the instructions and were, hence, more reliable for that task. Second, the probability of forgetting to record the test time diminished when the participant was old, female, and frail, which could indicate more attention from the surveyor to the persons showing those characteristics. Third, the opposite was true for the TMT-B when the person suffered from depression, which apparently perturbed the interviewer. Still, the more obvious positive impact of the respondent’s cooperative attitude suggests that the atmosphere—the climate of the social interactions between the interviewer and the participant—has a real effect.
5 Conclusion
This contribution addresses the complicated challenge of surveying vulnerabilities and vulnerable persons in a context of decreasing participation rates for surveys, especially in Switzerland and among the elderly. Vivre-Leben-Vivere (VLV) has been a laboratory in which various experiences have been accumulated. It is structured through the frame offered by the total survey error approach, resulting in several lessons of general interest.
The first challenge is related to the costs, a point that must not be definitively neglected, since most social science surveys are funded by public money and reveal resource inequalities within a society. From that point of view, outdated frame information is related to unavoidable problems specific to the elderly (like death) or not (mobility, discrepancy between de jure and de facto addresses). They are costly in financial terms, but for VLV, they also affected the motivations of some interviewers, resulting in non-contacts after many contact attempts. The survey collaborators were required to be resilient, to receive many kind but also aggressive refusals, to insist, and to travel through cities and the countryside, through the plains and the mountains, always with the risk of only finding a closed door or just a postal box. And of course, they had to be paid.
The second challenge is related to the refusals by the sample members who do not want to participate. Here, we face a real problem that moreover appears to be continuously growing. The reasons deserve more attention. Does the constantly increasing refusal rate result from reactions to over-solicitations by survey and market institutes or from a crisis of confidence with respect to research, combined with tendencies to socially withdraw, tendencies which can be related to socio-emotional processes associated with ageing and to the perceptions of the elderly in our societies? All of these aspects were apparent in the causes of refusal observed during the VLV fieldwork. This issue still needs to be more systematically addressed before the challenge becomes impossible to take up. Specifically, in the Vivre-Leben-Vivere survey, notwithstanding a participation rate of only 35 %, no fewer than 45 % of the files were obtained by repeated phone calls, home visits, and resorting to proxies. It is an enormous proportion, and it seems difficult to imagine going beyond this, at least with this mode of data collection.
However, “do low survey response rates bias results?” (Rindfuss et al. 2015). This is a third challenge that also includes the ability to include vulnerable persons in the sample of respondents. Based on the collected data, having quite simple but sound tools make it possible to identify states of vulnerability, in terms of evidence, latency (overexposure to risk), and absence on several dimensions. These indicators have been used to test the survey procedures. The results show contrasting effects linked to widely varying situations and a heterogeneity that is a fundamental characteristic of the aged population. Among the “young old,” obstinacy in phone calls allowed the most dynamic to be surveyed, particularly men. In the intermediary areas between the so-called 3rd and 4th ages (75–84), home visits were somewhat effective in including people that the questionnaire analysis is revealing now as facing latent states of vulnerability. And among those at the most advanced ages, whose health is also the most affected, the approach by proxies effectively incorporated those who are evidently vulnerable, especially women. In the second stage, the prevalence of poverty, functional health problems, and depression in the VLV data was compared with other data sources. Overall, we can conclude that Vivre-Leben-Vivere faced the challenge and that vulnerable elderly are well-represented in its sample of respondents. The low participation rate has not biased the results, at least from our research perspective. Once again and specific to a survey on old adults, home visits and, even more, the recourse to proxies explain this success.
We should fairly consider the recent criticisms made against the proxy method, but also bear in mind that its contribution to studies on the aged is undeniable. More thought should be given to the ethical conditions of its use in the future, since we obviously face a tension between strict respect for what must be an informed consent and the scientific, social, and political relevance of the research. Groves and Lyberg (2010) noted with insistence that relevance is a difficult to assess, although essential, component in the identification of what contributes to the “quality” of a survey. To stay away from this tension, an option may be to refrain from collecting information on subjective measures and to collect only “objective” data on health and material conditions.
A fourth challenge, which is rarely directly related to the preceding one, concerns item non-response, or the refusal by the participants to answer certain questions. It is a reasonable hypothesis to assume negative impacts of both latent and manifest states of vulnerability on such risks. At the same time, saying “no” is also a proper use of the participant’s individual agency and consequently can express the inverse of personal vulnerability. Consequently, estimating the resulting impact on the measurement errors can be delicate. And indeed, the evidence in the VLV data is mixed, both in the self-administered and face-to-face questionnaires, with some situations that reveal dis-affiliation, dis-adjustment, or withdrawal, and others revealing a self-conscience and capacity to decide. Typically, as far as poverty is concerned, non-response to the questions on household monthly income come disproportionately from the oldest old and women, who are groups at risk, but also from people with high levels of education, who are just the opposite. When we come to the assessment of cognition, we reach a point at which the survey’s legitimacy and scientific objectives appear to be contested by the main collaborators—the interviewers. They expressed their doubts on the basis of their fieldwork experience when very concretely dealing with this part of the questionnaire, and the required devices (exercise sheets, stopwatch, computer), at the same time as trying to give clear instructions, and preserving proper social interactions with the respondent. Situations of failure that affected the participants also affected the interviewers’ attitudes, once again with contrasting effects: better attention to frail people but less to depressed persons. Obviously, the climate of the interviews, the quality of the interactions, and more generally the means of maintaining adherence to the survey objectives, and the civic engagement of each participant (both those who answer as well as those who question) must remain central concerns.
Notes
- 1.
With a touch of irony, Jean-Pierre Michel and his colleagues speak of fragility as an “unusual topic in the 1980s (less than 50 articles before 1990), an over-employed topic in the 1990s (1981 times between 1991 and 2000) and which had in 2001 and 2002 already been the subject of 724 publications in newspapers with an editorial policy” (Michel et al. 2005, 230).
- 2.
65–69 years, 70–74 years, 75–79 years, 80–84 years, 85–89 years, and 90 years and over.
- 3.
“Ego” is the word used in the survey to refer to the interviewed person.
- 4.
Dealing with the other point, the validity of the answers given by ego or a proxy, respectively, is part of the ongoing doctoral thesis of Aude Tholomier on octogenarians and nonagenarians.
- 5.
The report distinguishes between “minor” and “major” difficulties, whereas these categories are collapsed in VLV. Thus, the percentages for minor difficulties (6 %) and major difficulties (1 %) are were merged to compare them to the VLV data.
- 6.
The cases of break-off were quite dramatic for the interviewer and took a large role in the team discussions, but they were ultimately statistically rare.
- 7.
Walking clubs; sports associations; political, professional, patriotic, and religious, groups; charities; etc.
- 8.
Question O2 offers a good illustration. Its formulation is “Generally, who—the family or the State—has to be responsible for:—financial help?” The modalities of the answers are only the family, mainly the family, both equally, mainly the State, and only the State.
- 9.
Less than 1200, 1200–2400, 2400–3600, 3600–4800, 4800–6000, 6000–7200, 7200–10,000, 10,000–15,000, 15,000 and more.
- 10.
Note that we applied this model to the non-answers for the question on monthly household income, but we only found a limited gender effect (a female interviewer had somewhat more non-responses, on average); quite obviously, when the interaction was positive (when the interviewer evaluated the respondent as cooperative), the non-answers were halved. For the sake of parsimony, we remained with the simple model shown in Table 10.
- 11.
A confirmation of the difficulty to manage the tasks for the interviewers is that out of the 900 initial missing duration information in the CAPI, more than 300 could be completed thanks to annotations on the exercise sheet. The interviewer simply forgot to introduce the result in the computer.
References
Baer, N., Schuler, D., Füglister-Dousse, S., & Moreau-Gruet, F. (2013). Depressionen in der Schweizer Bevölkerung. Daten zur Epidemilogie, Behandlung und sozial-beruflichen Integration. Neuchâtel: Schweizerisches Gesundheitsobservatorium (OBSAN Bericht 56).
Bak, C. K., & Larsen, J. E. (2014). Social exclusion or poverty individualisation? An empirical test of two recent and competing poverty theories. European Journal of Social Work, 18(1), 1–19.
Baltes, M. M., & Lang, F. R. (1993). Everyday functioning and successful aging: The impact of resources. Psychology and Aging, 12, 433–443.
Baltes, P. B., & Mayer, K. U. (1999). The Berlin Aging Study: Aging from 70 to 100. New York: Cambridge University Press.
Berrut, S., & Junker, C. (2008). D’une génération à l’autre. Evolution des causes de décès en Suisse de 1970 à 2004. Neuchâtel: Office fédéral de Statistique.
Bétemps, C., Bickel, J.-F., Brunner, M., & Hummel, C. (1997). Journal d’une enquête. La récolte de données dans le cadre d’une recherche sur échantillon aléatoire. Lausanne: Réalités sociales.
Bickel, J.-F. (2014). La participation sociale, une action située entre biographie, histoire et structures. In I. Mallon, C. Hummel, & V. Caradec (Eds.), Vieillesses et vieillissements (pp. 207–226). Rennes: Presses universitaires de Rennes.
Blom, A., De Leeuw, E., & Hox, J. (2011). Interviewer effects on nonresponse in the European social survey. Journal of Official Statistics, 27(2), 359–377.
Börsch-Supan, A. (coord.). (2005). Health, ageing and retirement in Europe. First results from the survey of health, ageing and retirement in Europe. Mannheim: MEA.
Börsch-Supan, A., Hank, K., Jürges, H., & Schröder, M. (2008). Longitudinal data collection in continental Europe: Experiences from the survey of health, ageing and retirement in Europe (SHARE). Mannheim: Research Institute for the Economics of Aging.
Bourdelais, P. (1997). L’âge de la vieillesse. Histoire du vieillissement de la population. Paris: O. Jacob.
Bowie, C. R., & Harvey, P. D. (2006). Administration and interpretation of the Trail Making test. Nature Protocols, 1, 2277–2281.
Bundesamt für Statistik. (2012). Gesundheit von Betagten in Alters- und Pflegeheimen. Erhebung zum Gesundheitszustand von betagten Personen in Institutionen (2008/2009), Neuchâtel.
Bundesamt für Statistik. (2014). Die funktionale Gesundheit von älteren Menschen in Privathaushalten, Neuchâtel.
Cavasso, B., & Weber, G. (2014). The effects of the great recession on the wealth and financial distress of 65+ Europeans. In A. Börsch-Supan, M. Brandt, H. Litwin, & G. Weber (Eds.), Active ageing and solidarity between generations in Europe (pp. 27–36). Berlin: De Gruyter.
Cheschire, H., Oftedal, M. B., Scholes, S., & Schroeder, M. (2011). A comparison of response rates in the English Longitudinal Study of Ageing and the Health and Retirement Study. Longitudinal and Life Course Studies, 2(2), 127–144.
Dannefer, D. (2001). Age stratification. In N. J. Smelser & P. Baltes (Eds.), Encyclopedia of the social and behavioral sciences (pp. 278–283). Oxford: Pergamon.
Dannefer, D. (2003). Cumulative advantage/disadvantage and the life course: Cross-fertilizing age and social science theory. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 58(6), 327–337.
De Leeuw, E. (2008). Self-administered questionnaires and standardized interviews. In A. Pertti, L. Bickman, & J. Brannon (Eds.), Handbook of social research methods (pp. 313–327). London: Sage Ltd.
De Luca, G., & Peracchi, F. (2005). Survey participation in the first wave of SHARE. In A. Börsch-Supan & H. Jürges (Eds.), The survey on health, aging, and retirement in Europe–methodology (pp. 88–101). Mannheim: Mannheim Research Institute for the Economics of Aging.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessement, 49, 71–76.
Durrant, G. B., Groves, R. M., Staetsky, L., & Steele, F. (2010). Effects of interviewer attitudes and behaviors on refusal in household surveys. Public Opinion Quarterly, 74, 1–36.
Duvoisin, A., Baeriswyl, M., Oris, M., Perrig-Chiello, P., & Bickel, J.-F. (2012). Pro Senectute : visibilité et usages d’une association bientôt centenaire. Au service des vulnérables ? Genève: CIGEV.
Fillit, H. M., Rockwood, K., & Woodhouse, K. (Eds.). (2010). Brocklehurst’s textbook of geriatric medicine and gerontology. Amsterdam: Elsevier.
Gabriel, R. (2015). Inequalities within progress? Social stratification and the life course among the elderly population in Switzerland between 1979–2011. PhD in Socioeconomics, University of Geneva.
Gabriel, R., Oris, M., Studer, M., & Baeriswyl, M. (2015). The persistence of social stratification? A life course perspective on old-age poverty in Switzerland. Swiss Journal of Sociology, 41(3), 465–487.
Girardin, M., Spini, D., & Ryser, V.-A. (2008). The paradox of well-being in later life: Effectiveness of downward social comparison during the frailty process. In E. Guilley & C. J. Lalive d’Epinay (Eds.), The closing chapters of long lives (pp. 129–142). New York: Nova Science Publishers.
Groves, R. M. (2011). Three eras of survey research. Public Opinion Quarterly, 75(5), 861–871.
Groves, R. M., & Couper, M. P. (1998). Nonresponse in household interview surveys. New York: Wiley.
Groves, R. M., & Lyberg, L. (2010). Total survey error, past, present, and future. Public Opinion Quarterly, 74(5), 849–879.
Groves, R. M., Fowler, F. J., Jr., Couper, M. P., Lepkowski, J. M., Singer, E., & Tourangeau, R. (2004). Survey methodology. New York: Wiley.
Guggisberg, M., Müller, B., & Christin, T. (2012). Pauvreté en Suisse: concepts, résultats et méthodes. Résultats calculés sur la base de l’enquête SILC 2008 à 2010. Neuchâtel: Office fédéral de Statistique.
Guilley, E., & Lalive d’Épinay, C. (Eds.). (2008). The closing chapters of long lives. Results from the 10-year Swilsoo study on the oldest old. New York: Nova Science Publishers.
Ihle, A., Oris, M., Fagot, D., Baeriswyl, M., Guichard, E., & Kliegel, M. (2015). The association of leisure activities in middle adulthood with cognitive performance in old age: The moderating role of educational level. Gerontology (in press).
Joye, D., Pollien, A., Sapin, M., & Ernst Stähli, M. (2012). Who can be contacted by phone? Lessons from Switzerland. In: M. Häder, S. Häder, & M. Kühne (Eds.), Telephone surveys in Europe: Research and practice (pp. 85–102). Heidelberg: Springer.
Katz, S., Ford, A. B., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963). Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychological function. JAMA, 185(12), 914–919.
Köhler, M., Kliegel, M., for the AgeCoDe Study Group, et al. (2011). Malperformance in verbal fluency and delayed recall as cognitive risk factors for impairment in instrumental activities of daily living. Dementia and Geriatric Cognitive Disorders, 31, 81–88.
Lalive d’Épinay, C., & Spini, D. (2008). Les années fragiles: La vie au-delà de quatre-vingts ans. Québec: Les Presses de l’Université Laval.
Lalive d’Épinay, C., Bickel, J.-F., Maystre, C., & Vollenwyder, N. (2000). Vieillesses au fil du temps. 1979–1994: Une révolution tranquille. Lausanne: Réalités sociales.
Lawton, M. P., Moss, M., Hoffman, C., Grant, R., Ten Have, T., & Kleban, M. H. (1999). Health, valuation of life, and the wish to live. Gerontologist, 39, 406–416.
Lessler, J. T., & Kalsbeck, W. D. (1992). Nonsampling error in surveys. New York: Wiley.
Ludwig, C., Cavalli, S., & Oris, M. (2014). ‘Vivre/Leben/Vivere’: An interdisciplinary survey addressing progress and inequalities of aging over the past 30 years in Switzerland. Archives of Gerontology and Geriatrics, 59(2), 240–248.
Malter, F. (2013). Fieldwork monitoring in the survey of health, ageing and retirement in Europe (SHARE). Survey Methods: Insights from the Field. Retrieved from http://surveyinsights.org/?p=1974
Marchese, O. (2011). Questionnaires, enquêteurs et enquêtés. Document de travail Conservatoire nationale des Arts et Métiers, France.
Marpsat, M., & Razafindratsima, N. (2010). Survey-methods for hard-to-reach populations. Introduction to the special issue. Methodological Innovations, 5(2), 3–16.
Masotti, B., & Oris, M. (2015). Il ricorso ai servizi domiciliari e il ruolo della famiglia nella quarta età. In: F. Giudici, S. Cavalli, M. Egloff, & Masotti (Eds.), Fragilità e risorse delle persone anziane residenti in Ticino (pp 87–109). sl, Ufficio di statistica.
Michel, J.-P., Guilley, E., Armi, Fr., & Robine, J.-M. (2005). Les multiples dimensions de la fragilité. In: Ph. Thomas et C.H. Thomas (dir.), Traité de psychogériatrie (pp. 230–239), Med-Line.
Nicolet, M., & Oris, M. (forthcoming). Mesures et capture de la vulnérabilité dans une enquête sur les conditions de vie et de santé des personnes âgées. L’expérience de VLV (Vivre-Leben-Vivere) en Suisse. In Conférence Universitaire de Démographie et d’Etude des Populations, Les Populations vulnérables, Bordeaux, CUDEP.
Nolan, B., & Marx, I. (2009). Economic inequality, poverty, and social exclusion. In S. Wiemer, B. Nolan, & T. M. Smeeding (Eds.), The Oxford handbook of economic inequality (pp. 315–341). New York: Oxford University Press.
Oris, M., & Lerch, M. (2009). La transition ultime. Longévité et mortalité aux grands âges dans le bassin lémanique. In: Transitions dans le parcours de vie et construction des inégalités (pp 407–432). Lausanne: Presses polytechniques et universitaires romandes.
Paugam, S. (2000). Le salarié de la précarité. Paris: Presses Universitaires de France.
Peytchev, A., Baxter, R., & Carley-Baxter, L. (2009). Not all survey effort is equal. Reduction of nonresponse bias and nonresponse error. Public Opinion Quaterly, 73(4), 785–806.
Pilgram, A., & Seifert, K. (2009). Vivre avec peu de moyens. La pauvreté des personnes âgées en Suisse. Zurich: Edition Pro Senectute.
Reitan, R. (1958). Validity of the Trail Making Test as an indicator of organic brain damage. Perceptual and Motor Skills, 8, 271–276.
Rindfuss, R. R., Choe, M. K., Tsuya, N. O., Bumpass, L. L., & Tamaki, E. (2015). Do low survey rates bias results? Evidence from Japan. Demographic Research, 32, 797–828.
Roberts, C., Vandenplas, C., & Ernst Stähli, M. (2014). Evaluating the impact of response enhancement methods on the risk of nonresponses bias and survey cost. Survey Research Methods, 8(2), 67–80.
Robine, J.-M., & Jagger, C. (2004). Allongement de la vie et état de santé de la population. In G. Caselli, J. Vallin, & G. Wunsch (Eds.), Démographie : analyse et synthèse (Population et société, Vol. VI, pp. 51–84). Paris: INED.
Scholes, S., Medina, J., Cheschire, H., Cox, K., Hacker, E., & Lessof, C. (2009). Living in the 21st century: Older people in England. The 2006 English longitudinal study of ageing. Technical Report, National Center for Social Research.
Sen, A. K. (1999). Development as freedom. Oxford: Oxford University Press.
SKOS/CSIAS. (2013). Armut und Armutsgrenze – Grundlagenpapier der SKOS. Bern: SKOS/CSIAS.
Snijkers, G., Hox, J. J., & De Leeuw, E. D. (1999). Interviewers’ tactics for fighting survey nonresponse. Journal of Official Statistics, 15, 185–198.
Tourangeau, R., Edwards, B., Johnson, T., Wolters, K., & Bates, N. (Eds.). (2014). Hard-to-survey populations. Cambridge: Cambridge University Press.
Van Oyen, H., Nusselder, W., Jagger, C., Kolip, P., Cambois, E., & Robine, J. M. (2013). Gender differences in healthy life years within the EU: An exploration of the “health-survival” paradox. International Journal of Public Health, 58(1), 143–155.
Vaupel, J. W., Manton, K. G., & Stallard, E. (1979). The impact of heterogeneity in individual frailty on the dynamics of mortality. Demography, 16(3), 439–454.
Wang, R. I., et al. (1975). A brief self-assessing depression scale. Journal of Clinical Pharmacology, 15(2–3), 163–167.
Wanner, P., Gabadinho, A., & Pecoraro, M. (2008). La situation économique des actifs et des retraités. Berne: Office fédéral des Assurances sociales.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution-NonCommercial 2.5 International License (http://creativecommons.org/licenses/by-nc/2.5/), which permits any noncommercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made. The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2016 The Author(s)
About this chapter
Cite this chapter
Oris, M. et al. (2016). Representation of Vulnerability and the Elderly. A Total Survey Error Perspective on the VLV Survey. In: Oris, M., Roberts, C., Joye, D., Ernst Stähli, M. (eds) Surveying Human Vulnerabilities across the Life Course. Life Course Research and Social Policies, vol 3. Springer, Cham. https://doi.org/10.1007/978-3-319-24157-9_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-24157-9_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-24155-5
Online ISBN: 978-3-319-24157-9
eBook Packages: Social SciencesSocial Sciences (R0)