
Abstract
Infectious diseases is one of the most common cause of the visits to pediatric office and emergency department as well.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
- Prevention of infectious diseases
- Antibiotics
- Antivirals
- Antiparasites
- Antifungal
- Viral infections
- Bacterial infections
- Fungal infections
- Protozoal infection
- Helminths
- Brain abscess
- Meningitis
- Encephalitis
Prevention of Infectious Diseases
Child-Care Center
Risk of acquiring infections in child-care center
-
Poor hygiene increases the risk of young children for recurrent infections and development of antibiotic resistance .
Prevention
-
Good hand washing; wash hands with soap and water, alcohol-based antiseptic is acceptable
-
Disinfecting environmental surfaces
-
Frequent facility cleaning
-
Appropriate food handling
-
Teach children and staff to sneeze or cough into elbow (not hands)
-
Use gloves when contacting body fluids
Common organism in child-care centers:
-
Shigella infection
-
Transmitted from infected feces (person-to-person contact)
-
Do: stool bacterial cultures for any symptomatic contact
-
Know: if Shigella infections are confirmed should receive appropriate antibacterial treatment
-
Return to child-care center
-
◦ If diarrhea has resolved and stool cultures are negative
-
-
-
Nontyphoidal Salmonella species
-
No antibiotic is required except:
-
◦ Infants younger than 3 months of age
-
◦ Immunocompromised host
-
-
Infected individuals should be excluded from child care until symptoms resolve
-
-
Salmonella serotype typhi
-
Treatment is indicated for infected individuals
-
Return to child-care center
-
◦ 5 years of age or younger: 48 h after antibiotic treatment
-
◦ Older than 5 years: 24 h after the diarrhea has resolved
-
-
-
Other risk of infection: e.g., giardia, rotavirus, cryptosporidiosis, respiratory syncytial virus (RSV), parainfluenza virus, adeno, rhino, and corona viruses hemophilus influenza, pneumococcal, hepatitis A and, cytomegalovirus infections
Prevention of Hospital and Office Infection
-
Standard precautions are indicated in the care of all patients including:
-
Hand hygiene before and after each patient contact
-
Protective equipment when needed
Preventive methods
-
Alcohol-based products are preferred because of their superior activity and adherence
-
Soap and water are preferred when hands are visibly soiled or exposed to a spore-forming organism, e.g., ( Clostridium difficile is the most common)
-
Gloves, isolation gowns, masks, and goggles for any exposure to body fluids contaminated materials or sharps
-
Strict aseptic technique for all invasive procedures, and for catheter care
-
Separate well and sick children areas in the medical offices
Examples of infections and agents requiring transmission-based precautions
-
Contact precautions, e.g., RSV, C. difficile, and Staphylococcus aureus
-
Gloves and gowns are required when there is direct patient contact
-
-
Droplet precautions, e.g., Influenza, Neisseria meningitidis, and Bordetella pertussis
-
Use of a surgical mask is required
-
A single room is preferred
Remember all office and hospital staff should receive an annual influenza immunization
-
Airborne precautions, e.g., Mycobacterium tuberculosis, measles, and varicella (with contact precautions)
-
Negative pressure airborne infection isolation room
-
Room needs 6–12 air changes per hour or recirculated through a high-efficiency particulate air (HEPA) filter
-
Tested N95 or similar sealing mask
-
-
Prevention of Infection Through Breast Feeding
-
Exclusive breastfeeding for the first 6 months is recommended by American Academy of Pediatrics (AAP)
Immunologic characteristics of breast milk
-
Postpartum colostrum contains high concentrations of antibodies and other infection-protective elements (natural immunization).
-
The actual antibodies against specific microbial agents present in an individual woman’s milk depends on her exposure and response to the particular agents.
-
Lactoferrin: Limits bacterial growth by iron chelation.
-
Lysozyme: Bacterial cell wall lysis.
-
Lactalbumin: Enhance the growth Bifidobacterium and affects immune modulation.
-
Casein: Limits adhesion of bacteria and facilitates the growth of Bifidobacterium.
-
Carbohydrates: Enhance the growth of probiotics.
-
Lipids: Lytic effect on many viruses and are active against Giardia as well.
-
Absolute contraindication of breast feeding
-
Human immunodeficiency virus 1 (HIV-1) infection (if replacement feeding is acceptable, feasible, affordable, sustainable, and safe)
-
Human T-lymphotropic virus 1 and 2 infection (varies by country; in Japan, breastfeeding is initiated)
-
Tuberculosis (active, untreated pulmonary tuberculosis, until effective maternal treatment for the initial 2 weeks or the infant is receiving isoniazid)
-
Herpes simplex virus infection on a breast (until the lesions on the breast are cleared)
-
-
Medical Evaluation of Internationally Adopted Children
-
Evaluation for tuberculosis (TB) infection and purified protein derivative (PPD) testing
Immunizations
-
Written immunization record is accepted for the number of doses, interval, and appropriate age of immunization
-
Serologic testing to determine protective antibodies: Tetanus antibodies (the test of choice) other antibodies for diphtheria, polio, and hepatitis B can be measured
-
Pertussis titer do not reliably predict protection against infection
-
Measles vaccine should not be administered routinely to children younger than 1 year
Prevention of Vector-Borne Disease
-
Chemoprophylaxis before travelling to endemic areas, e.g., mefloquine for malaria should be given before travelling to endemic areas
-
Use mosquito netting during sleep in tropical areas
-
Use protective clothing and garments
-
Repellents, e.g., DEET ( < 30 %) applied to children as young as 2 years of age and should be used in endemic area
-
DEET can be applied every 6–8 h all over the body areas
-
Insecticide should not applied to children’s hands because of risk of ingestion
-
-
Use of occlusive cloth to prevent tick bite is paramount
-
Immunization against disease when travelling to endemic area 1–2 months before, e.g., dengue, typhus, cholera depending on the country of destination
Recreational Water Use
-
Exposure to contaminated water can cause diarrhea, and other infections, e.g., swimmer’s ear
-
Cryptosporidium is the most common cause of gastrointestinal diseases associated with recreational water
-
People with diarrhea should not participate in recreational water activities
-
Children with diarrhea should avoid swimming for 2 weeks after cessation of diarrhea
-
Avoid ingestion of water
-
Clean the child with soap and water before swimming
-
Diaper change in the bathrooms
Infections in Immunocompromised Hosts
Malnutrition
-
Protein energy malnutrition causes immune deficiency and increase susceptibility to infection
Asplenia
-
e.g., sickle cell anemia, congenital or surgical asplenia
-
Bacteremia and meningitis due to Streptococcus pneumoniae, H. influenzae type b and N. meningitidis
-
Special vaccine consideration
-
Pneumococcal conjugate and polysaccharide vaccines are indicated for all children with asplenia at the recommended age.
-
Following administration of appropriate number of doses of PCV13, pneumococcal polysaccharide vaccine (PPSV23) should be administered starting at 24 months of age.
-
A second dose of PPSV23 should be administered 5 years later.
-
Two primary doses of quadrivalent meningococcal conjugate vaccine should be administered 2 months apart to children with asplenia from 2 years of age through adolescence, and a booster dose should be administered every 5 years.
-
Malignancy
-
Neutropenia ANC < 500 increases the risk of bacterial infection
-
Fever may be the only the manifestation
-
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) (opportunistic infection)
-
Burn injury
Indwelling catheters
-
Central-related catheter infections are common complication e.g.:
-
Coagulase negative staphylococci
-
Vancomycin is therapeutic drug of choice
-
Candida infection is another common cause
Antibiotics
Aminoglycosides, e.g., gentamicin, tobramycin, and amikacin
Mechanism of action
-
Inhibit bacterial protein synthesis by binding to bacterial 30S ribosome
-
Drug activity
-
Against aerobic gram-negative organism, e.g., Yersinia pestis plague, Francisella tularensis
-
It has some activity against Staphylococcal species, Mycobacterium, Entamoeba histolytica, Cryptosporidium parvum
-
Drug toxicity
-
Nephrotoxicity and ototoxicity
Drug Monitoring
-
Indication for monitoring aminoglycosides
-
If the drug to be used 5 days or more
-
If there is renal impairment
-
Trough level is used only but the peak level used in certain circumstances
-
-
Trough level:
-
Serum level of drug obtained just before the fourth or fifth dose
-
Trough concentration for gentamicin or tobramycin that are greater than 2 µg/mL associated with risk of toxicity
-
Prolonging the interval or decreasing the dose can be used to address elevated trough level
-
-
Peak level (not commonly used)
-
Should be measured 30 min after completion of fourth or fifth dose
-
If too low increase the dose by 25 % to reach the desired peak level (e.g., gentamicin peak level 8–10 µg/mL)
-
-
Drug use in serious infections (used in combination with other antibiotics), e.g.,
-
Septicemia
-
Neutropenic fever
-
Nosocomial respiratory infections
-
Complicated intra-abdominal infections
-
Pyelonephritis
-
Beta Lactam Antibiotics
Classes of beta lactam antibiotics
-
Penicillins
-
Cephalosporins
-
Carbapenems
-
Monobactams
Mechanism of action of beta lactams:
-
Inhibit cell wall synthesis by binding and inhibiting cell wall proteins called penicillin-binding proteins (PBPs).
Penicillins, e.g., crystalline penicillin
Indications
-
Periodontal infections
-
Erysipeloid
-
Group A and group B streptococci
-
Syphilis
-
Meningococcal meningitis and meningococcemia
Ampicillin
Bacterial coverage
-
Similar to penicillin but its spectrum extends to some gram-negative bacteria
Indications
-
Listeria monocytogenes meningitis
-
Enterococcal infections
-
Urinary tract infections (UTIs) caused by susceptible strains of Escherichia Coli
Amoxicillin-Clavulanate (Augmentin)
Bacterial coverage
-
Addition of beta-lactamase inhibitors increase coverage to methicillin-sensitive S. aureus (MSSA)
-
Extended coverage for respiratory infections, e.g., sinusitis, otitis media, bronchitis
Drug of choice for bite wounds
-
Pasteurella is susceptible to penicillin
-
Pasteurella and S. aureus are the likely organisms in most of animal bites
Penicillinase Resistant Penicillins, e.g., nafcillin or oxacillin
-
Drug of choice only for staphylococcal infection (MSSA) but the resistance is rapidly expanding.
Anti-Pseudomonal Penicillins, e.g., piperacillin and ticarcillin
Bacterial coverage
-
Extended gram-negative coverage including Pseudomonas species, S. aureus and H. influenzae
-
Addition of beta-lactamase inhibitors:
-
Piperacillin-tazobactam (Zosyn)
-
Ticarcillin-clavulanate (Timentin)
-
-
Drug of choice, e.g., Pseudomonas aeruginosa
Cephalosporins (penicillinase-resistant)
-
First generation cephalosporin, e.g., cefazolin and cephalexin
-
Bacterial coverage
-
◦ Many gram-positive cocci including methicillin-sensitive S. aureus and most Streptococcus
-
◦ No reliable central nervous system (CNS) penetration, do not use for meningitis or arteriovenous (AV) shunts infections
-
-
Indications
-
◦ Skin and soft tissue infection
-
-
-
Second generation cephalosporins, e.g., cefaclor, cefoxitin, cefuroxime, and cefotetan
-
Bacterial coverage
-
◦ Maintains gram-positive activity but less than first generation
-
◦ Greater coverage for gram-negative bacteria than first generation, e.g., ( H. influenzae Enterobacter aerogenes, and some Neisseria)
-
◦ Extend the coverage to respiratory gram negative, e.g., ( H. influenzae and Moraxella)
-
◦ Has variable activity against gut anaerobes except cefuroxime
-
Do not use for meningitis
-
-
Indications
-
◦ Abdominal surgeries
-
◦ Community acquired pneumonia
-
◦ Pelvic inflammatory disease (PID)
-
-
-
Third generation cephalosporins
-
Bacterial coverage
-
◦ Extended gram-negative activity, loss of gram-positive activity
-
◦ Penetrates the cerebrospinal fluid (CSF) well
-
◦ Has greater activity in deep tissue infections and less toxicity than aminoglycosides
-
◦ Only few drugs are active against P. aeruginosa, e.g., ceftazidime
-
-
Ceftriaxone
-
-
◦ Has the longest half-life and effective against most S. pneumoniae
-
◦ Crosses the blood brain barrier and indicated as the primary therapy for meningitis
-
◦ Ceftriaxone can be used as single agent for empiric treatment of meningitis while lab results are pending except neonates ampicillin need to be added to cover for Listeria
-
-
-
Cefotaxime
-
Bacterial coverage is the same as ceftriaxone
-
◦ It is preferred in neonates or < 30 days old
-
-
-
-
Fourth generation cephalosporin, e.g., cefepime
-
Bacterial coverage
-
◦ Equal gram-positive as the first the generation cephalosporins
-
◦ Equal gram-negative as the third generation cephalosporins
-
◦ Excellent Pseudomonas coverage
-
-
Carbapenems, e.g., imipenem/cilastatin and meropenem
-
Imipenem is a very-broad-spectrum carbapenem antibiotic.
-
It is very active against Bacteroides fragilis.
-
It kills most Enterobacteriaceae, pseudomonas, gram-positive bacteria, and is inhibitory for listeria, and Enterococcus faecalis.
-
Imipenem can lower the seizure threshold and should not be used in patients with seizures or renal insufficiency.
-
Meropenem is a similar carbapenem with a longer half-life, less likely than imipenem to cause seizures.
Monobactam, e.g., aztreonam
-
Aztreonam is often used in patients who are penicillin allergic or who cannot tolerate aminoglycosides.
-
Aztreonam has strong activity against susceptible aerobic and facultative gram-negative bacteria, including P. aeruginosa, most Enterobacteriaceae.
-
Aztreonam is not active against gram-positive cocci or anaerobes.
Other Commonly used Antibiotics
Clindamycin
Mechanism of action
-
Inhibit bacterial protein synthesis by binding to 50S ribosomal subunit
Bacterial coverage
-
Active against many strains of methicillin-resistant S. aureus (MRSA)
-
Active against anaerobes
-
Active against most staphylococcal and streptococcal infections
Adverse reaction
-
Diarrhea including C. difficile enterocolitis
Macrolides, e.g., azithromycin and clarithromycin
Mechanism of action
-
Inhibit bacterial protein synthesis by binding to 50S ribosomes
-
Azithromycin does not inhibit cytochrome P-450 as erythromycin or clarithromycin do
Bacterial coverage
-
Azithromycin is the drug of choice for pertussis, Mycoplasma and Chlamydia
Adverse reaction
-
Gastrointestinal irritation
-
Hypertrophic pyloric stenosis if used in children less than 1 month of age
Rifampin
Bacterial coverage
-
Tuberculosis
-
Invasive H. influenzae
Indications
-
Close contacts to a child who has invasive meningococcal infection
-
Combination with vancomycin in certain staphylococcal infections (VP shunt, osteomyelitis, endocarditis)
-
Persistent group A streptococcal pharyngitis in combination with beta-lactam antibiotics
-
MRSA carriage eradication attempt
Fluoroquinolones, e.g., ciprofloxacin
AAP recommendation of fluoroquinolones use in children
-
If the pathogen is multidrug resistant
-
No safe and other effective alternative
-
Parenteral therapy is not feasible
-
No other effective alternative oral agents
Bacterial coverage
-
UTIs caused by multidrug resistant gram negatives rods
-
Resistant gram negative rods:
-
P. aeruginosa
-
Gastrointestinal and respiratory tract infection
-
Chronic or acute osteomyelitis
Adverse reaction
-
Fluoroquinolones has no documented evidence of increased incidence of arthropathy in pediatric patient using fluoroquinolones
-
Tetracycline
Bacterial coverage
-
Tetracycline provides coverage against tick borne organisms, e.g., (Lyme disease, Rocky Mountain spotted fever)
-
Doxycycline and minocycline are used for acne ( Propionibacterium acnes)
-
Doxycycline may have MRSA coverage as well
Adverse reaction
-
Tetracyclines causes staining of dental enamels.
-
Tetracycline is not recommended in children less than 8 years old.
-
Tetracyclines can be used in children younger than 8 years in life threatening situations, e.g., rocky mountain spotted fever (doxycyclines is the drug of choice).
-
Doxycycline does not cause staining of permanent teeth comparing to tetracyclines.
Trimethoprim/sulfamethoxazole
Bacterial coverage
-
Pneumocystis jiroveci which is common in immunocompromised patient, e.g., HIV
-
Urinary tract infection , treatment, and prophylaxis (drug of choice in susceptible patients)
-
Methicillin-resistant staphylococcal infection
-
Gastroenteritis due to salmonella, shigella, and isospora belli
-
Burkholderia cepacia
-
Brucella
Adverse reaction
-
Rash
-
Neutropenia
-
Stevens–Johnson syndrome
Vancomycin
Mechanism of action
-
Inhibits bacterial cell wall synthesis by binding tightly to peptidoglycan precursors and blocking polymerization
Bacterial coverage
-
Confirmed gram positive infection in patient seriously ill or allergic to beta-lactam antibiotics
-
Initial empiric treatment in a child (> 2 months) with meningitis in combination with third generation cephalosporin
-
Methicillin-resistant staphylococcal infection
-
Prophylaxis before prosthetic device implantation requiring major surgery
-
Enterally for C. difficile
-
Acute infectious endocarditis if S. aureus is the likely cause
Adverse reaction
-
Red man syndrome, or red neck syndrome
-
Vancomycin releases histamine that can cause pruritus, erythema of the head and neck
-
This is a related drug infusion problem just slow down the infusion rate and premedicate the patient with diphenhydramine
-
-
Ototoxicity and nephrotoxicity (follow the trough level and adjust the dose accordingly)
-
Misuse of vancomycin cause development of resistance
Indications
-
C. difficile diarrhea (It is not systemically absorbed)
-
S. aureus infections
Antivirals
Acyclovir
Mechanism of action
-
Terminates the viral deoxyribonucleic acid (DNA) synthesis when incorporated into the viral DNA chain .
Appropriate use of acyclovir
-
Herpes simplex virus (HSV) type 1 and HSV type 2
-
Varicella
-
Treatment of recurrent primary genital HSV2 or primary HSV1 mucocutaneous infections
-
IV acyclovir is the drug of choice for treatment of HSV encephalitis
Major side effect of acyclovir
-
Acute renal failure due to precipitation in the renal tubules (proper hydration and slower infusion can minimize this problem)
-
Nausea, vomiting, and diarrhea
Valacyclovir
Background
-
Newer potent oral antiviral (Inhibits DNA polymerase; incorporates into viral DNA)
Indications
-
HSV1
-
HSV2
-
Varicella-Zoster virus (VZV)
Ganciclovir
Indications
-
CMV infection
Foscarnet
-
CMV infection
Other Antiviral Agents, Against DNA Viruses
-
Famciclovir, valganciclovir, penciclovir, and cidofovir
Nucleoside Reverse Transcriptase Inhibitors
Mechanism of action
-
These drugs inhibit replication of HIV by interfering with the reverse transcriptase enzyme
Indication
-
HIV infection
Example of nucleoside reverse transcriptase inhibitors and their side effects
-
Zidovudine (ZDV)
-
Significant side effect; bone marrow suppression
-
-
Didanosine (ddI)
-
Significant side effects; pancreatitis and peripheral neuropathy
-
-
Zalcitabine (ddC)
-
Significant side effects; stomatitis and neuropathy
-
-
Stavudine (d4T)
-
Contraindication:
-
◦ Cannot be combined with ddI in pregnant women can cause fatal lactic acidosis
-
-
Side effects; pancreatitis and peripheral neuropathy
-
Abacavir
-
Most serious side effect is FATAL hypersensitivity
-
Nonnucleoside Reverse Transcriptase Inhibitors (NNRTI)
Indication
-
HIV infection
Example of NNRTI and common side effects
-
Efavirenz
-
Teratogenic
-
-
Nevirapine
-
Rash
-
Protease Inhibitors
Mechanism of action
-
Inhibit the HIV protease enzyme that involved with processing the completed virus
Indication
-
HIV infection
Examples of protease inhibitors medications and the common side effects
-
Indinavir
-
Asymptomatic hyperlipidemia
-
Nephrolithiasis
-
-
Nelfinavir
-
Diarrhea
-
-
Saquinavir
Antiparasites
Permethrin
-
Excellent safety profile
-
Five percent permethrin is the drug of choice for treatment of scabies
-
It paralyze the parasite and cause death
-
One percent permethrin solution is effective for head lice
-
It is not recommended in infants younger than 2 months and during pregnancy
Metronidazole
Mechanism of action
-
Metronidazole is nitroimidazole bactericidal drug
Indications
-
Anaerobic bacteria
-
Clostridium
-
Trichomonas vaginalis
-
Gardnerella vaginalis
-
Treponema pallidum
-
Oral spirochetes
-
Helicobacter pylori
Malathion
-
It is the most effective drug in the treatment of pediculosis or head lice
-
It has ovicidal activity
-
Single topical application is effective in resistant cases
Chloroquine
Indication
-
It is the drug of choice for malaria prophylaxis in the sensitive chloroquine regions, e.g., Central and South America
-
Drug should be administered 1–2 weeks before travelling
-
Adverse effect
-
Gastrointestinal (GI) upset, headache, dizziness, blurred vision, insomnia, and pruritus
-
Mefloquine and atovaquone/proguanil
-
Commonly used for prophylaxis for malaria in chloroquine resistant regions, e.g., Africa and Middle east
Antifungals
Amphotericin B
Indication
-
Active against broad array of fungi, e.g., Candida, Aspergillus, Zygomycetes, Histoplasma, Coccidioides immitis
Toxicity
-
Febrile drug reaction
-
Hypokalemia
-
Hypomagnesemia
-
Nephrotoxicity (liposomal preparation is equally effective and less nephrotoxic)
Fluconazole
Indications
-
It is equally effective for treatment of invasive Candida albicans in neonates as amphotericin B
-
Treatment of oropharyngeal or esophageal candidiasis in immunocompromised patients
-
Treatment of vulvovaginal Candida
-
Treatment of cryptococcal meningitis
Griseofulvin
-
It is the standard first-line therapy for tinea capitis
-
No laboratory assessment of hepatic enzyme if used < 8 weeks
-
Serum liver enzyme monitoring every 8 weeks; prolonged therapy is a risk of hepatotoxicity
-
Consume with fatty meals for maximum absorption, e.g., peanut butter
Herpes Family Viruses (DNA Viruses)
-
HSV-1, HSV-2
-
Epstein–Barr virus (EBV)
-
CMV
-
VZV
-
Human Herpesvirus type 6 (HHV-6)
-
Human Herpesvirus Type 7 (HHV-7)
-
Human Herpesvirus Type 8 (HHV-8)
Herpes Simplex Virus HSV-1 and HSV-2
Background
-
HSV (both types 1 and 2) belongs to the family Herpesviridae
-
It is a double-stranded DNA virus
-
Characterized by neurovirulence, latency, and reactivation
-
The reactivation and replication of latent HSV always in the area supplied by the ganglia in which latency was established
-
Reactivation can be induced by various stimuli (e.g., fever, trauma, emotional stress, sunlight, and menstruation)
Mode of transmission
-
HSV-1; direct contact with infected secretions or lesion
-
HSV-2; direct contact with infected genital lesions or secretions (sexual transmission or during birth in neonates)
-
Risk of infection with HSV-1 increases with age
-
Incubation period of approximately 4 days, but can range from 2 to 12 days.
-
Period of communicability; viral shedding period that lasts at least 1 week and up to several weeks.
-
Newborn to mothers with primary herpes infection are more likely to be infected than infants born to mother with recurrent genital herpes simplex infection
-
Herpes simplex virus can be transmitted from a person with a primary recurrent infection regardless whether any symptoms are present
Diagnosis
-
The gold standard for laboratory diagnosis is the viral culture
-
HSV polymerase chain reaction (PCR; useful for CSF testing)
-
HSV IgG and IgM antibodies
-
Herpetic gingivostomatitis (HSV-1 common in infant and young children)
-
Fever
-
Multiple round ulcers or superficial erosions commonly affecting the palate, tongue, and gingiva
-
Diffuse erythema and swelling of the gingiva
-
Drooling, foul-smelling breath, and anorexia
-
Dehydration in children whose painful lesions result in poor fluid intake
-
Pain control and sufficient rehydration is the mainstay of management
Herpes labialis
-
The most common manifestation of HSV-1 infection
-
Recurrent orofacial herpes (commonly called fever blisters or cold sores)
-
The outer vermilion border is a common location
-
The crusted lesions often are confused with staphylococcal or streptococcal impetigo (secondary bacterial infection may occur)
-
Oral acyclovir or valacyclovir can be effective if started within 1–2 days of prodromal symptoms
Genital herpes
-
Most commonly caused by HSV-2 which is a sexually transmitted infection (STI)
-
Possible routes are:
-
Hematogenous route
-
Direct spread from mucocutaneous sites through the peripheral nerves
Complications
-
Urinary retention
-
Psychological morbidity
-
Aseptic meningitis
Treatment
-
Oral antiviral medication can be effective if started early
-
Chronic suppressive therapy with an oral antiviral is recommended for patients experiencing frequent recurrences (at least six episodes per year)
-
Herpetic keratoconjunctivitis
-
Ocular HSV infection is the second most common infectious cause of blindness worldwide
-
HSV-1 is the predominant cause
-
Neonates afflicted with ocular HSV may have associated systemic or CNS disease
-
Management
-
Prompt referral to ophthalmology is recommended to prevent complications such as permanent scarring, secondary bacterial infection, meningoencephalitis, and vision loss
-
Treatment consists of both topical ophthalmic antiviral (trifluridine, vidarabine, idoxuridine) and oral antiviral medications
-
Herpetic Whitlow (Fig. 1)
Fig. 1 
Herpetic Whitlow: 8 years old boy with painful blisters, grouped vesicular lesions with surrounding erythema on the index finger
-
Due to autoinoculation of HSV-1 (more in children) or HSV-2 (more in adolescents)
-
Vesiculoulcerative lesions affect the pulp of the distal phalanx of the hand associated with deep-seated swelling, and erythema
-
Oral antiviral medications are optional and are used in extensive disease
-

Herpes gladiatorum (Fig. 2)

Herpes gladiatorum: 16 years old boy wrestling player presents with painful blisters in the left ear
-
HSV-1 is more likely to be the agent than HSV-2
-
Herpes gladiatorum occurs in contact sports, e.g., wrestling and boxing
-
Most commonly affects exposed areas, e.g., face and upper extremities
-
Patients should avoid contact sports during outbreaks until the culture results are negative
-
Suppressive therapy is likely to be effective, but data about such therapy are insufficient
-
Herpes encephalitis and meningitis
-
Herpes encephalitis
-
Altered mental status
-
Personality changes
-
Seizures
-
Focal neurologic findings
-
-
HSV meningitis
-
CSF pleocytosis, with lymphocyte predominance and red blood cells
-
High protein in the CSF
-
-
Mollaret meningitis
-
Recurrent aseptic meningitis (mostly herpetic)
-
Episodes of severe headache, meningismus
-
Fever that resolve spontaneously
-
-
Complications
-
Bell palsy, atypical pain syndromes, trigeminal neuralgia, ascending myelitis, and postinfectious encephalomyelitis.
-
-
Recommended therapy: Parenteral acyclovir for 21 days.
Neonatal herpes
-
Neonatal herpes usually manifests in the first 4 weeks after birth
-
Clinical presentation
-
Lesion; skin, eye, and mouth (SEM)
-
CNS (often presenting with seizures, lethargy, and hypotonia)
-
Disseminated (including liver, adrenal glands, lungs)
-
-
Disseminated neonatal HSV
-
Shock
-
Elevated liver enzymes
-
Disseminated intravascular coagulation
-
Multiple organ system failure
-
-
Management
-
Institute therapy pending culture results if significant suspicion exists, e.g.,
-
Sepsis syndrome with negative bacteriologic culture results
-
Severe liver dysfunction
-
Fever and irritability
-
Abnormal CSF findings, particularly if seizures are present
-
-
-
Timely diagnosis and prompt initiation of treatment are crucial
Eczema herpeticum
-
Eczema herpeticum also is known as Kaposi varicelliform eruption
-
HSV infections of skin with underlying barrier defect, e.g., atopic dermatitis
-
Vesicles and crusts coalescing into plaques on underlying eczematous skin
Management
-
Intravenous (IV) antiviral therapy
-
Antibiotic therapy for secondary bacterial infection
-
Topical emollients
-
Topical corticosteroids in areas of atopic dermatitis once systemic antiviral therapy has been initiated
-
The use of calcineurin inhibitors is contraindicated in eczema herpeticum
-
-
Epstein–Barr Virus (EBV)
Background
-
EBV or human herpesvirus 4, is a gammaherpesvirus that infects more than 95 % of the worlds population with infection
-
Mode of transmission primarily by oral contact with saliva
-
EBV is shed in saliva at high concentrations for more than 6 months following acute infection and intermittently at lower concentrations for life
-
Young children directly or through the handling of toys
-
Adolescents; close contact such as kissing
-
Clinical presentation
-
EBV infection in healthy person; Infectious mononucleosis (EBV is the most common cause)
-
Fever
-
Sore throat (similar to streptococcal pharyngitis but more painful)
-
Cervical lymphadenopathy commonly anterior and posterior cervical lymph node (may compromise the airway)
-
Splenomegaly (90 %); 2–3 cm below the left costal margin is typical
-
Hepatomegaly (10 %)
-
Fatigue and malaise (might take from 6 months to few years to improve)
-
Rash
-
This condition generally is a benign, self-limited illness in healthy persons
EBV infection in immunocompromised persons
-
Nonmalignant EBV-associated proliferations, e.g., virus-associated hemophagocytic syndrome
-
Nasopharyngeal carcinoma, Burkitt's lymphoma, and Hodgkin disease
-
Diagnosis
-
Heterophile antibodies test is Not recommended for children younger than 4 years of age
-
The IgM-VCA (most valuable and specific serologic test)
-
EBV serology (Table 1)
Table 1 Serum Epstein-Barr virus (EBV) antibodies in EBV infection (Adapted from the Red Book Epstein-Barr Virus infections., 27th ed. AAP; 2006)
Management
-
Short courses of corticosteroids for fewer than 2 weeks can be given in the following cases:
-
Upper airway obstruction
-
Thrombocytopenia complicated by bleeding
-
Autoimmune hemolytic anemia
-
Seizures
-
Meningitis
-
Cytomegalovirus (CMV)
Background
-
CMV is a double-stranded DNA virus and is a member of the Herpesviridae family. At least 60 % of the US population has been exposed to CMV.
-
CMV usually causes an asymptomatic infection; afterward, it remains latent throughout life and may reactivate.
Mode of transmission and period of communicability
-
Vertical transmission
-
CMV can be maternally transmitted during pregnancy, perinatally, or after postnatal exposure
-
Postnatally can be transmitted via human milk
-
Risk decreased by the use of pasteurized human milk
-
Horizontal transmission
-
Exposure to CMV can occur from almost all body fluids, including:
-
◦ Urine, saliva, and tears
-
◦ Genital secretions and transplanted organs
-
-
Toddlers infected postnatally with CMV shed the virus in their urine for a mean of 18 months (range 6–40 months)
-
Healthy adults infected with CMV will shed the virus for only up to several weeks
-
Shedding of CMV in toddlers in child care centers can be as high as 70 %
-
-
Transfusion and transplantation
-
Can be eliminated by CMV-negative donors
-
Filtration to remove white blood cells (WBCs)
-
Latent form in tissue and WBCs can be reactivated many years later
Congenital CMV infection
-
Microcephaly
-
Periventricular calcifications
-
Chorioretinitis, strabismus, microphthalmia, and optic nerve atrophy
-
Hypotonia, poor feeding, ventriculomegaly, cerebellar hypoplasia
-
Intrauterine growth restriction
-
Prematurity
-
Jaundice
-
Hepatosplenomegaly
-
Thrombocytopenia; petechiae and purpura
-
Sensorineural hearing loss (SNHL); 7–15 % will develop progressive SNHL later in childhood
Diagnosis
-
Perinatally:
-
CMV immunoglobulin M in fetal blood or by isolating the virus from amniotic fluid
-
-
Postnatally:
-
Congenital CMV is confirmed by detection of the virus in urine, blood, and saliva within the first 3 weeks of life by culture or PCR
-
Treatment
-
Congenital CMV
-
Treatment of unclear benefit
-
CNS disease is sometime treated with ganciclovir for 6 weeks
-
Pneumonitis, hepatitis, and thrombocytopenia is sometimes treated with ganciclovir for 2 weeks
-
-
CMV retinitis in HIV
-
Ganciclovir and valganciclovir are indicated for induction and maintenance therapy
-
-
CMV pneumonitis in BM or stem cell transplant patients
-
Ganciclovir plus CMV immune globulin are used together
-
-
Varicella-Zoster Virus (VZV); Chickenpox
Background
-
VZV is herpesvirus family member, and is highly contagious
-
Spreading via direct contact, airborne droplets, and transplacental passage
-
VZV is the cause of chickenpox and herpes zoster
Clinical presentation
-
The prodrome: is low-grade fevers, headaches, and malaise developing after the incubation period
-
Skin lesions initially appear on the face and trunk
-
Each lesion starts as a red macule and passes through stages of papule, vesicle, pustule, and crust
-
The vesicle on a lesion’s erythematous base leads to its description as a pearl or dewdrop on a rose petal
-
The lesions predominate in central skin areas and proximal upper extremities with relative sparing of distal and lower extremities
-
Subsequent central umbilication and crust formation
-
Patients are considered contagious until all lesions crust over
-
Chickenpox generally is a benign self-limited illness, especially in healthy children under age 12 years
Complication
-
Acute complications
-
Bacterial superinfection of cutaneous lesions, specially Streptococcus pyogenes which can progress to cellulitis and myositis
-
Pneumonia (major cause of morbidity and mortality), hepatitis, and thrombocytopenia
-
-
Post-infectious complications
-
Cerebellar ataxia
-
Encephalitis
-
Shingles (Herpes Zoster)
Background
-
VZV is the cause of chickenpox and herpes zoster
-
Herpes zoster reactivation of the dormant virus residing in cells of the dorsal root ganglia
-
Shingles classically is a unilateral rash consisting of grouped vesicles on an erythematous base, covering one to three adjacent dermatomes, often accompanied by pain and pruritus
-
The diagnosis can be rapidly confirmed by vesicular fluid testing by using either VZV PCR or direct fluorescent antibody (DFA) assay
Congenital varicella syndrome:
-
low-birth weight
-
Intracranial calcifications and cortical atrophy
-
MR and seizures
-
Chorioretinitis and cataract
-
Cicatricial scarring of body or extremities is diagnostic especially if infection at 8–20 weeks gestation
Prevention
-
Children can go back to school if all lesions are crusted
-
VZIG given to the baby born to infected mother if < 5 days before birth or 2 days or less after birth
-
Intravenous acyclovir is indicated for varicella infection in infants born to mothers who experience chickenpox from 5 days before until 2 days after delivery
Human Herpesvirus Type (HHV)-6 or Roseola Infantum (Exanthem Subitum)
Background
-
Caused by HHV-6 or -7
-
Commonly affect age between 6 and 18 months
Clinical presentation (Fig. 3)

Roseola infantum: 9 months old boy afebrile presents with small, pale pink papules and blanchable, maculopapular exanthem, had high fever for 3 days before the rash
-
Very high fever for several days, followed by maculopapular rash after the resolution of fever
-
Maculopapular rash appears on the trunk and extremities hours to days after fever
-
They may have lymphadenopathy, vomiting, diarrhea, febrile seizure, or respiratory symptoms
-
HHV-6 is a common cause of febrile seizure
Management
-
Mainly supportive
Human Herpesvirus-7 (HHV-7)
-
Childhood febrile illness, somewhat unclear
Human Herpesvirus-8 (HHV-8)
-
Kaposi sarcoma
-
Hemophagocytic lymphohistiocytosis
Other DNA Viruses
-
Parvovirus B19
-
Adenovirus
Parvovirus B19 (Erythema Infectiosum/Fifth Disease)
Background
-
Incubation period 4–14 days
-
Mode of transmission: by respiratory secretions
Clinical presentation
-
Erythema infectiosum
-
Mild constitutional symptoms, e.g., Fever, malaise, myalgia, and headache
-
Bright red facial rash (slapped cheek appearance)
-
Circumoral pallor
-
Lacy maculopapular rash begin on the trunk and move to extremities (Fig. 4)
Fig. 4 
Erythema infectiosum: erythematous maculopapular rash on the arm, which fades into a classic lacelike reticular pattern as confluent areas clear
-
. The rash last for 2–4 days.
-
Rash may be pruritic, does not desquamate, may recur with bathing or exercise
-
Arthritis or arthralgia may occur
-
-
Aplastic anemia
-
Hemolytic disease such as sickle cell anemia, spherocytosis, thalassemia transient low to zero reticulocyte leukopenia
Transient low to zero reticulocyte, and leukopenia
-
Chronic anemia in HIV disease
-
Adult acute arthritis
-
Hydrops fetalis
-
-
Remember
-
Rash is not infectious and children can go to school without restrictions
-

Adenovirus
-
Background
-
Mode of transmission:
-
Person to person through contact with respiratory secretions
-
Fecal-oral transmission, and via fomites
-
-
Outbreaks usually are concentrated in winter, spring, and early summer otherwise all year round
-
Incubation period:
-
Respiratory infections from 2 to 14 days
-
Gastrointestinal disease from 3 to 10 days
-
Clinical presentation
-
Respiratory tract infection:
-
Nonspecific febrile illness
-
Upper respiratory tract infection
-
Otitis media
-
Pharyngitis
-
Exudative tonsillitis
-
Pneumonia
-
-
Pharyngoconjunctival fever:
-
Fever, tonsillitis (sometimes suppurative)
-
Follicular conjunctivitis, coryza, and diarrhea
-
Cervical and preauricular lymphadenopathy is common
-
Generalized rash in association with fever, conjunctivitis , and pharyngitis can be mistaken for Kawasaki disease
-
Laboratory
-
Antigen detection and viral culture and serology
Management
-
Adenoviral infections generally are self-limited and require no more than supportive treatment.
-
Respiratory Viruses
-
Influenza
-
Parainfluenza
-
Respiratory syncytial virus
-
Human metapneumovirus
-
Rhinovirus
-
Coronavirus
Influenza Virus
Background
-
Influenza is an orthomyxovirus
-
Types: A, B, and C. Types A and B are responsible for epidemic disease in humans
-
Influenza A viruses found in humans are H1N1 and H3N2
-
Frequent antigenic change, or antigenic drift:
-
◦ Point mutations during viral replication, results in new influenza virus variants
-
◦ Point mutations causing seasonal epidemics that generally occur in winter months in temperate zones
-
-
Occasionally, influenza A viruses form a new subtype through antigenic shift, creates the possibility of a pandemic
-
-
Mode of transmission:
-
Large-particle respiratory droplet between individuals
-
Contact with contaminated surfaces
-
Incubation period is 1–4 days
Clinical presentation
-
Fever, malaise, myalgia, headache , nonproductive cough, sore throat, and rhinitis.
-
Children also may develop croup or bronchiolitis .
-
Younger children may have febrile seizures or sepsis like symptoms.
-
Uncomplicated influenza disease typically resolves within 3–7 days.
Complications
-
Primary viral pneumonia
-
Secondary bacterial infections such as pneumonia ( S. aureus and S. pneumoniae)
-
Sinusitis and otitis media
-
Encephalitis
-
Underlying medical conditions such as asthma or congenital heart disease increases morbidity
Diagnosis
-
Rapid antigen-detection tests, immunofluorescence
-
Viral culture, and reverse transcriptase-polymerase chain reaction (RT-PCR)
-
In general, testing should be performed when the results are expected to affect patient care
-
AAP immunization guidelines
-
AAP recommend annual vaccination of all children ages 6 months through 18 years before the start of influenza season.
-
Regardless of seasonal epidemiology, children 6 months through 8 years of age who previously have not been immunized against influenza require two doses of trivalent inactivated influenza vaccine (TIV) or live-attenuated influenza vaccine (LAIV) administered at least 1 month apart to produce a satisfactory antibody response.
Three types of influenza vaccine
-
TIV.
-
Quadrivalent influenza vaccine now available.
-
LAIV.
-
Egg allergy is not a contraindication to influenza vaccine anymore, except severe allergic reaction (e.g., anaphylaxis)
Indication of antiviral medications
-
Children who have influenza and are at high risk for complications, regardless of the severity of their illness.
-
Healthy children who have moderate-to-severe illness.
-
Oseltamivir is a neuraminidase inhibitors approved for treatment and prophylaxis of both influenza A and B.
-
Oseltamivir is administered orally.
-
The most common adverse effects are nausea and vomiting, although neuropsychiatric events have been reported.
Avian Influenza H5N1
Background
-
Reported cases were in south Asia, Iraq, Turkey, and Egypt
-
Highly pathogenic strain in birds and poultry
-
It is not a human strain
Mode of transmission
-
Human who have close contact to infected birds or poultry
-
Visiting market selling live infected birds
Clinical presentation
-
Severe lower respiratory disease in infected persons
Prevention
-
H5N1 specific vaccine (developed and approved)
-
Avoid visiting markets where live birds are sold
-
Thorough cooking inactivates the virus but avoidance poultry if there a concern is more appropriate
Parainfluenza Virus
Background
-
Parainfluenza viruses are paramyxoviruses distinct from the influenza family
Clinical manifestation
-
May cause a clinical syndrome similar to that of influenza
-
It is major cause of laryngotracheobronchitis (croup) in children (see respiratory section)
-
They also can cause pneumonia and bronchiolitis
-
Most parainfluenza infections are self-limited
Respiratory Syncytial Virus
Background
-
Infection with RSV, the most common cause of bronchiolitis
-
More than 90,000 hospitalizations of RSV infections
-
High risk infants of severe bronchiolitis:
-
Infants younger than 3 months of age are at increased risk for apnea
-
Prematurity
-
Neonatal respiratory distress syndrome
-
Unrepaired congenital heart disease
Clinical presentation
-
Upper respiratory prodrome is very common
-
Cough, nasal congestion, and rhinorrhea
-
Tachypnea
-
Increased work of breathing
-
Nasal flaring and grunting
-
Inter-costal, supracostal, and subcostal retractions
Suprasternal, Intercostal,and subcostal retractions
-
Crackles, wheezes, and referred upper airway noise
-
Upper airway obstruction can contribute significantly to increased work of breathing
-
Variable hypoxemia
Diagnosis
-
Based on history and physical examination
-
Routine laboratory or radiologic studies are not recommended to support the diagnosis
-
Common radiologic findings include hyperinflation, areas of atelectasis, and infiltrate
Management
-
Suctioning may increase comfort and improve feeding.
-
Excessive suction can be associated with nasal edema and lead to additional obstructions.
-
-
Know the “Day of illness” the worsening clinical symptoms, with peak symptomatology around day 3–4 of illness.
-
Intravenous fluid hydration and oxygen administration may be required.
-
Bronchodilators use is not recommended by AAP for routine use.
-
If an improvement in clinical status is documented, continued treatment with bronchodilator therapy might be considered.
-
-
Corticosteroid medications, inhaled or administered systemically, should not be used in the treatment of bronchiolitis .
-
Initiation of antibiotic therapy for suspected acute otitis media (AOM) should be based on patient age, severity of illness, and diagnostic certainty.
-
Chest physiotherapy should not be used to treat bronchiolitis.
-
Human Metapneumovirus
Background
-
Humans are the only source
-
Overlap with RSV season
Clinical presentation
-
Bronchiolitis indistinguishable from RSV bronchiolitis
-
Most children have one human metapneumovirus infection before 5 years of age
Treatment
-
Supportive
Rhinoviruses (RVs)
-
The most common cause of common cold (25–80 % of cases).
-
The common cold is an acute respiratory tract infection (ARTI) characterized by mild coryzal symptoms, rhinorrhea, nasal obstruction, and sneezing.
-
The most common virus triggers asthma.
-
About 200 antigenically distinct viruses from eight different genera can cause common cold as well (66–75 %).
Severe Acute Respiratory Syndrome (SARS) Associated Coronavirus Infection
Background
-
Outbreak occurred with hundreds of reported death cases in China, Hong Kong, Taiwan, and Singapore.
-
Can cause SARS.
-
SARS-associated coronavirus (SARS-CoV).
-
Through air travel can spread to many areas of the world, e.g., Canada.
-
It is a serious potentially life-threatening viral infection.
Mode of transmission
-
Airborne is the primary route
Clinical presentation
-
Most cases affect adults
-
Young children usually develop milder symptoms if infected
-
Fever, cough, difficulty breathing
Treatment
-
Mainly prevention
-
No specific treatment showed benefits
Gastrointestinal Viral Infection
-
Norovirus (Norwalk virus)
-
Rotavirus
Norwalk Virus
Background
-
Norovirus, formerly referred to as Norwalk virus, is the most common cause of epidemic nonbacterial gastroenteritis in the world.
-
CDC report that noroviruses account for more than 96 % of all viral gastroenteritis cases in the USA.
Clinical presentation
-
Nausea and vomiting (profuse, nonbloody, nonbilious)
-
Watery diarrhea (nonbloody)
-
Abdominal cramps
-
Headaches
-
Low-grade fever is common: but temperatures may reach 38.9 °C
-
Myalgias and malaise
Rotavirus
Background
-
It is a cause of severe acute gastroenteritis
-
The disease is significant in infants who are not immunized with rotavirus vaccine
Clinical presentation
-
Severe watery diarrhea, electrolyte imbalance, and metabolic acidosis
-
Severe dehydration can occur
Immunization
-
Oral human attenuated monovalent rotavirus (RV1) or Rotarix for 2 and 4 months of age by mouth
RNA Viruses
-
Enterovirus
-
HIV
-
Measles
-
Mumps
-
Rubella
-
Rabies
-
Arboviruses
Enteroviruses
-
Non-polio viruses (coxsachievirus A and B, echoviruses and enterovirus)
-
Background
-
More common in the summer
-
Enteroviruses transmitted by the feco-oral route and person to person
-
-
Meningitis/Encephalitis
-
Meningitis commonly caused by echovirus
-
Common in older children
-
Fever, headache, photophobia, and nuchal rigidity, CSF pleocytosis
-
Severe complications: seizure, hemiparesis, hearing loss, and mental deterioration
-
No signs toxicity as in bacterial meningitis
-
Best diagnostic test: CSF enterovirus PCR
-
-
Herpangina
-
Caused by Coxsackievirus type A is a subgroup of enterovirus which is a subgroup of picornavirus
-
Sudden onset of high fever in 3–10 years of age, and can be associated with vomiting, malaise, myalgia, and backache
-
Poor intake, drooling, sore throat, dysphagia, and dehydration may occur
-
Oral lesions:
-
◦ One or more small tender papular pinpoint vescular lesions, on erythematous base on anterior pillars of the faucets, soft palate, uvula, tonsils, and tongue, then ulcerate in 3–4 days.
-
-
-
Hand-foot-mouth disease (Fig. 5)
Fig. 5 
Hand-foot-mouth disease: a. Tender vesicles and macules on an erythematous base, and crusted vesicles on the foot and the leg. b. Multiple vesicles that erode and become surrounded by an erythematous halo in the mouth. c. Erythematous macules and vesicles on the palm
-
Coxsackie A16 and enterovirus 71
-
Fever (may be present)
-
Oral vesicles and ulcers on buccal mucosa and tongue
-
Painful vesicles on hands and feet, it may affect the groin, and buttocks
-
Usually last for 7–10 days
-
Most common complication is dehydration due to odynophagia
-
-
Acute hemorrhagic conjunctivitis
-
Subconjunctival hemorrhage
-
Swelling, redness, and tearing of the eye
-
Resolve spontaneously within 7 days
-
-
Myocarditis/pericarditis
-
Commonly caused by Coxsackievirus B or echovirus
-
Common symptoms; shortness of breath, chest pain, fever, and weakness
-
-
Congenital and neonatal infection
-
Can range from mild febrile infection to encephalitis and negative bacterial culture
-
Can cause hepatic necrosis
-
Poliovirus infection
Background
-
Polioviruses are enterovirus belong to family of Picornaviridae
Clinical presentation
-
Fever common in less than 6 years of age
-
Aseptic meningitis
-
Flaccid paralysis in a descending manner without reflexes
-
The poliovirus destroys the anterior horn cells in the spinal cord
-
-
Diagnosis
-
Viral stool culture
-
Throat swab
-
-
Treatment
-
No curative treatment
-
-
Prevention
-
Polio vaccine (IPV/OPV)
-

Human Immunodeficiency Virus (HIV)
Background
-
HIV is RNA virus
-
Highest infectivity due to the very high (3–4 weeks) initial viremia
-
Nearly all patients seroconvert within 6 months of acquiring the infection
Mode of transmission
-
HIV infection is transmitted by two principal modes in the pediatric age group:
-
Mother-to-child
-
Transplacental transfer
-
Exposure to maternal blood, amniotic fluid, and cervicovaginal secretions during delivery
-
Postpartum through breastfeeding
-
-
Behavioral (risk behavior in adolescent either unprotected sex or injection drugs)
Clinical presentation
-
During the “window period:
-
Infected person has a negative HIV antibody test result, but HIV RNA testing results are usually positive
-
-
Acute retroviral syndrome, characterized by:
-
Fever, lymphadenopathy, rash, myalgia, arthralgia, headache, diarrhea, oral ulcers, leukopenia, thrombocytopenia, and transaminitis
-
-
Red flags of HIV infection
-
Thrush in apparently healthy child or adolescent
-
Invasive candidal infections
-
Recurrent severe infections
-
Lymphadenopathy and/or hepatosplenomegaly
-
Failure to thrive
-
Parotid enlargement
-
Diagnosis
-
Infants born to HIV-positive mothers
-
Most infants are normal at birth and then may develop lymphadenopathy, HSM, chronic diarrhea, failure to thrive , and oral candidiasis.
-
Within the first 48 h, 14 days, and 4 weeks of life, 38, 93, and 96 % of infected children, respectively, have positive HIV DNA PCR results.
-
Any positive HIV DNA PCR finding should be confirmed with follow-up HIV DNA PCR before infection is diagnosed.
-
HIV DNA PCR testing: HIV infection can be ruled out if one of the following is true:
-
DNA HIV PCR results are consistently negative in an infant older than 4 months in the absence of breastfeeding.
-
Two DNA HIV PCR results obtained at least one month apart are negative in an infant older than 6 months.
-
-
HIV antibody testing between 12 and 18 months of age to confirm the loss of maternal antibody is optional.
-
-
Screening and diagnosis of children older than age 18 months
-
Screening enzyme-linked immunoassay (EIA)
-
Confirmatory test such as western blot is performed if EIA is positive
-
Evaluation of HIV positive children
-
CD4 percentage and absolute cell counts
-
Plasma HIV RNA concentration (viral load)
-
HIV genotype to assess for baseline resistance, and mutations
-
Complete blood count with differential count
-
Serum chemistries with liver and renal function tests
-
Lipid profile and urinalysis
-
For children younger than 5 years of age, CD4 percentage is the preferred test for monitoring immune status
-
Screening for hepatitis B and C infection as well as for tuberculosis is recommended for all HIV-infected patients
Treatment of HIV
-
Triple-drug combination antiretroviral therapy effectively controls HIV infection
Prevention
-
Breastfeeding is contraindicated in HIV positive mothers
-
All exposed infants should receive 6 weeks of ZDV
-
Condoms and abstinence are the best forms of preventing sexual transmission of AIDS
-
Cesarean delivery and treatment of HIV-positive mothers (specially with high viral load) decreases the risk of transmission of HIV to their infants
Immunization of infants and children
-
Immunization schedule for HIV-exposed children is the same as for their healthy peers, with only a few exceptions:
-
◦ Patients who have severely symptomatic illness.
-
◦ Patient with CD4 percentage of less than 15 % or CD4 counts of less than 200 cells/mm3 should not receive measles-mumps-rubella (MMR), varicella vaccines or live vaccines.
-
-
Annual influenza immunization is recommended for all children older than age 6 months, but only the killed vaccine.
Measles
Background
-
Mode of transmission: respiratory droplets (airborne).
-
The virus is infectious for 3–4 days before the onset of morbilliform rash and 4 days after the exanthem.
Diagnosis
-
IgM level serology (most reliable test)
-
Antigen detection in respiratory epithelial cells
-
Tissue by immunofluorescent method or PCR
Clinical presentation
-
Coryza
-
Cough
-
Conjunctivitis
-
High fever
-
Koplik spots
-
Rash is erythematous maculopapular rash spread from up–down and disappear the same way
Prevention
-
Intramuscular (IM) immunoglobulin prophylaxis should be given to unimmunized child if exposed to measles infection
-
Infants (6–12 months) should be pre-vaccinated before travelling to high risk areas, e.g., India.
-
Children received measles vaccine before 1 year do not count and need to receive two doses of MMR after 12 months for full immunization.
-
Infected child with measles should be placed under airborne precaution transmission and isolated for 4 days after the rash and for all duration of illness if immunocompromised.
Complications
-
Otitis media is the most common
-
Pneumonia (common cause of death)
-
Encephalitis
-
Subacute sclerosing panencephalitis (SSPE) is rare and it may occur after 6–15 years
Mumps
Background
-
Mumps is an acute, self-limited, systemic viral illness characterized by the swelling of one or more of the salivary glands, typically the parotid glands.
-
The illness is caused by a specific RNA virus, known as Rubulavirus.
Mode of transmission
-
Airborne and contact to respiratory secretions
-
Incubation period is 12–25 days
Clinical presentation
-
Symptoms in the patient’s history consist mostly of fever, headache, and malaise.
-
Within 24 h, patients may report ear pain localized near the lobe of the ear and aggravated by a chewing movement of the jaw.
-
Unilateral or bilateral parotid swelling at least for 2 days.
Complications
-
Encephalitis and orchitis
-
Arthritis, thyroiditis, pancreatitis, myocarditis, oophoritis (rare)
Diagnosis
-
Serology and virus isolation
Prevention
-
MMR vaccine at 1 and 4 years of age
-
Isolation of infected individual is 9 days from the onset of parotid swelling
-
Unimmunized children should stay at home for 26 days from the last case in school
Rubella
Background
-
The name rubella is derived from a Latin term meaning “little red”.
-
Rubella is generally a benign communicable exanthematous disease.
-
It is caused by rubella virus, which is a member of the Rubivirus genus of the family Togaviridae.
-
Disease transmission: by droplet inhalation from the respiratory tract of an infected host.
-
Incubation period: 14–21 days.
-
Communicability: Patients are infectious 2 days before and 5–7 days after the rash.
Clinical presentation
-
Lymphadenopathy:
-
Retroauricular
-
Postauricular
-
Posterior occipital
-
-
Rash:
-
Maculopapular erythematous rash last for 3 days
-
Forschheimer spots; rose colored spot on soft palate
-
-
Other manifestation:
-
Pharyngitis and conjunctivitis
-
Anorexia, headache, and malaise
-
Low-grade fever and polyarthritis
-
Complications
-
Congenital rubella syndrome
-
Cataract, salt and pepper chorioretinitis, and deafness
-
PDA
-
IUGR and microcephaly
-
-
HSM and jaundice
-
Blueberry muffin rash
-
Anemia , thrombocytopenia, and leukopenia
B-cell, and T-cell deficiency
-
Metaphyseal lucencies
-
-
Infant with congenital rubella may shed the virus from the nasal mucosa > 1 year to susceptible contact
Rabies Virus
Background
-
Rabies virus is a RNA virus classified in the Rhabdoviridae family
-
Usually is transmitted by bats and carnivores, e.g., raccoon, foxes, and coyotes
Clinical presentation
-
Anxiety
-
Dysphagia
-
Seizures
-
Encephalitis
-
In most cases progress to death
Prophylaxis recommendation
-
All person bitten by, bats, carnivores, e.g., raccoon, foxes, and coyotes
-
Domestic animals that may be infected
-
Open wound or scratch contaminated with saliva of infected animals or human
-
Prompt local flushing and cleaning the wound with soap and water
-
The need for tetanus and antibiotic should be considered
Passive and active immunization should be started as soon as possible
-
Human rabies immunoglobulin (passive).
-
Rabies vaccine (active).
-
Both should be given together.
-
Human rabies immunoglobulin as much as possible of the dose should be infiltrated directly to wound, the remainder of the dose should be given intramuscularly.
-
Rabies vaccine should be given IM, the first dose immediately after exposure then repeated at days 3, 7, and 14.
Arboviruses
-
West Nile virus
-
Dengue fever
West Nile Virus
Background
-
It is the most common arbovirus identified in the USA
-
West Nile virus is transmitted by mosquitoes
-
Typically the spring and summer
-
California, Colorado, and Idaho are the most common location
Clinical presentation
-
Most cases are asymptomatic
-
May present with fever and flu-like symptoms
-
Fever, headache, altered mental status, paresis, nerve palsies, or coma in more severe cases
Diagnosis
-
Fourfold rise in virus-specific serum antibodies, or positive IgM-CSF antibody titer is helpful in the diagnosis
Treatment
-
Supportive
Dengue Fever
Background
-
Dengue fever is an arbovirus transmitted by mosquitoes
-
Typically the spring and summer
-
History of travel to endemic area is the most important part to assist in the diagnosis of Dengue fever
-
Endemic in Latin America and Puerto Rico
-
Key West, Miami, Florida are endemic areas in the USA
Clinical presentation
-
Severe muscle, and joint pain
-
Headache, and retro-orbital pain
-
Nonspecific rash, nausea, vomiting, diarrhea, and respiratory symptoms
-
It can lead to dengue shock syndrome and death
Laboratory
-
It may show leukopenia, thrombocytopenia, and modest elevation of liver enzyme
-
Fourfold rise in virus-specific serum antibodies, or positive IgM-CSF antibody titer is helpful in the diagnosis
-
Treatment is supportive
Hepatitis A Virus (HAV)
Background
-
HAV is the most common cause of viral hepatitis worldwide
-
No known animal reservoir
-
Mode of transmission is fecal-oral route
-
Incubation period is 15–50 days
-
Highest period of communicability is 1 week before and after the onset of symptoms
-
CD8 + T cells are responsible for the destruction of infected liver cells
Clinical presentation
-
In children younger than 5 years may be asymptomatic or with just few symptoms
-
Older children and adult may develop symptoms of acute infection which may last 2 weeks to several months
-
Malaise, anorexia, fever, nausea, vomiting, and eventually jaundice
-
Most of the cases generally resolve without sequelae within a few weeks
Diagnosis
-
Anti-HAV immune globulin M (IgM) in a single serum sample is a good test for current or recent infection.
Prevention
-
HAV vaccine at 12 months and booster dose at least 6 months after the initial dose.
-
Prevention of HAV infection can be promoted by enforcing good hygiene in child care centers, with conscientious hand washing after changing diapers and before handling food.
-
If travelling is imminent to endemic areas or the patient is immunocompromised, immunoglobulin (IG) can be administered simultaneously with vaccine.
Treatment
-
Mainly supportive
-
Avoid acetaminophen, it can exacerbate damage to liver cells
Prognosis
-
HAV does not carry the risk of chronic infection
-
Immunity after infection is life-long
Hepatitis B Virus (HBV)
-
Background
-
The infection has an incubation period of 2–6 months
-
HBV is commonly transmitted via body fluids such as blood, semen, and vaginal secretions
-
HBV does not spread by breast feeding, kissing, hugging, sharing utensils
Clinical presentation
-
Acute self-limited hepatitis:
-
Increase in serum transaminases and resolution of the infection within 6 months
-
Nausea
-
Fever
-
Abdominal pain
-
Jaundice, fatigue
-
General malaise
-
-
Fulminant hepatitis:
-
Acute hepatitis associated with a change in mental status due hepatic encephalopathy
-
-
Chronic hepatitis:
-
Generally is asymptomatic in childhood, having minimal or no effect on growth and development
-
Serum transaminase values usually are normal
-
They can flare at any time
-
Hepatitis B viral serology and liver functions tests
-
HBsAg is the first serologic marker to appear and found in infected persons, its rise correlates with the acute symptoms.
-
Anti-HBc is the single most valuable serologic marker of acute HBV infection, because it appears as early as HBsAg, and continue later in the course of the disease when HBsAg disappeared.
-
Anti-HBs marks serologic recovery and protection; marks vaccine immunity.
-
Both Anti HBs and Anti HBc are detected in person with resolved infection.
-
HBeAg is present in person with active acute or chronic infection and marks infectivity.
-
Anti-HBe marks improvement and is the goal of therapy in chronically infected patients.
-
Remember: Alanine transaminase (AST) and aspartate aminotransferase (ALT) can be derived from muscle, you should verify that serum creatine kinase and aldolase values are within the normal range before assuming that the elevated serum AST and ALT values are hepatic in origin.
-
Test reflecting cholestasis
-
High-serum concentrations of gamma-glutamyl transferase
-
High-serum alkaline phosphatase
-
High-conjugated bilirubin
-
-
Test reflecting liver failure
-
High-prothrombin time, despite administration of vitamin K
-
Low-serum albumin concentrations are the most useful indicators of impaired synthetic liver function
-
-
HBV perinatal infection
-
Nearly all perinatally acquired HBV infection are asymptomatic
-
Maternal screening of all pregnant women for HBV is now standard
-
Prophylaxis for all newborns of HBV-positive women in the first 12 h after birth:
-
◦ Combination of passive (IgG) and active immunization (first dose of the vaccine) followed by the complete HBV vaccine schedule
-
Breastfeeding does not increase the risk of transmission
-
Treatment is mainly supportive
-
Interferon-Alpha2b and lamivudine are the current approved therapy
-
Hepatitis C Viral Infection (HCV)
Background
-
HCV is a spherical, enveloped, single-stranded RNA virus belonging to the Flaviviridae family and Flavivirus genus
-
Egypt had the highest number of reported infections with 22 % prevalence of HCV antibodies in persons in Egypt.
Mode of transmission
-
Infants and children
-
The maternal-fetal route is the principal route of transmission
-
-
Adults
-
Injection during drug abuse is the most common mode of transmission
Long term complication of HCV infection
-
Chronic carrier
-
Chronic hepatitis
-
Hepatocellular carcinoma
-
Testing for HCV
-
HCV infection is investigated by measuring anti-HCV antibody and is confirmed by the detection of serum HCV RNA by PCR.
-
Screening of infants born to HCV-infected mothers is recommended by measuring serum anti-HCV antibody at 18 months of age.
-
Know that children with chronic hepatitis C infection should undergo periodic screening tests for hepatic complications and the treatment regimens are available.
Treatment (see GI chapter for more details)
-
Genotype 1 is the most aggressive and most resistant to antiviral therapy
-
Genome 2 and 3 has a better response
-
Remember: A high rate of spontaneous mutations in the viral genome is the reason for the lack of an effective vaccine .
Human Papillomavirus (HPV)
Background
-
Oncogenic strain 16 and 18 are responsible for two thirds of all cervical cancers
-
Nononcogenic HPV type 6 and 11 are responsible for > 90 % of anogenital wart
Immunization
-
Quadrivalent vaccine contains types 6, 11, 16, and 18
-
Bivalent vaccine contains 16 and 18
Bacterial Pathogens
Gram Positive Bacteria
S. aureus
Background
-
S. aureus is a well-known cause of both local and invasive infection
-
Coagulase positive
-
Grapelike clusters (Fig. 6)
Fig. 6 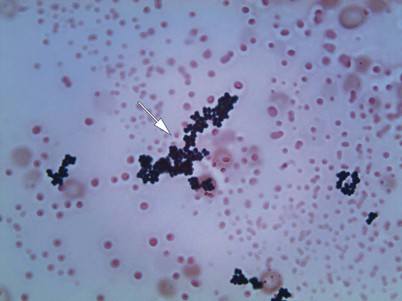
Staphylococci in blood culture (gram stain, original magnification × 1000). The bacteria are gram-positive cocci and grow inpairs, tetrads, and clusters ( arrow)
-
S. aureus colonizes the nares and skin in 30–50 % of children

Common staphylococcal infections:
-
Bullous and crusted impetigo.
-
Soft tissue or lymph node infection.
-
If the organism seeds the bloodstream, dissemination to joints, bones, kidney, liver, muscles, lung, and heart valves may occur, causing substantial morbidity and potential mortality.
-
S. aureus is the most common cause of osteomyelitis, except sickle cell anemia patients is usually caused by salmonella.
-
Children with cyanotic congenital heart disease are at high risk of staphylococcal brain abscess .
-
Children who undergo neurosurgical procedures, specially shunt revisions at high risk for staphylococcal infection.
-
Catheters are usually associated with staphylococcal infection and must be removed if the patient develops symptoms or positive culture, and antibiotic must be started.
Folliculitis/Furunculosis/Carbunculosis (Fig. 7a and b)

a Furuncle: erythematous tender papulonodule with central punctum with point of fluctuant. b Folliculitis: Superficial inflammation centered around a follicle, tender to touch
Background
-
Folliculitis: superficial inflammation centered around a follicle.
-
Furuncles: bacterial folliculitis of a single follicle that involves a deeper portion of the follicle.
-
Carbuncle: bacterial folliculitis that involves the deeper portion of several contiguous follicles.
-
Bacterial folliculitis most often caused by S. aureus.
-
Hot tub folliculitis is usually caused by gram-negative bacteria (most often P. aeruginosa. It is self limited).
-
Usually the child looks healthy and does not appear ill.
-
Abscess ( < 5 cm) drainage alone is curative and should be performed along with a request for culture.
Management
-
Indication of antibiotics
-
The child has high fever or other systemic symptoms .
-
The abscess is larger than 5 cm.
-
Located in a critical location or in a difficult to drain area.
-
Signs and symptoms persist following incision and drainage.
-
-
Common anti-staphylococcal antibiotics:
-
TMP-SMX effective against MRSA
-
Cephalexin remains a good empiric choice for MSSA and GAS infections
-
Clindamycin
-
Doxycycline (in children older than 8 years of age)
-
-
Recurrent staphylococcal skin infections recommendations:
-
Enhanced hygiene and environmental cleaning
-
Treatment for anyone in the family who has active disease
-
Nasal mupirocin
-
Skin decolonization (chlorhexidine or bleach baths)
-
Treatment with antibiotic-based decolonization regimens (usually rifampin plus an additional agent) in selected cases
-
Toxic Shock Syndrome (TSS)
Background
-
Production of toxic shock syndrome toxin-1 (TSST-1).
-
Can be caused by S. aureus or S. pyogenes.
Risk factors
-
Tampon
-
Surgical implants
-
Invasive staphylococcal disease, including pneumonia and skeletal infection
-
Nasal packing
-
Progressive skin infection in cases caused by S. pyogenes
Clinical presentation
-
Fever
-
Vomiting
-
Hypotension (abrupt onset)
-
Hypocalcemia
-
Watery diarrhea
-
Myalgia
-
Strawberry tongue
-
Conjunctival hyperemia
-
Rash with hand and foot desquamation
-
Blood culture is usually negative if the cause is S. aureus
-
Blood culture is usually positive if the cause is S. pyogenes
Treatment
-
Vancomycin or clindamycin
-
In cases of tampon-associated TSS, must be removed immediately and the recommended length of therapy is 10–14 days
-
IV fluid and routine management of shock.
-
Do not treat hypocalcemia unless is symptomatic or electrocardiogram (EKG) changes.
-
Anytime there is a postsurgical toxic shock, any device implanted during surgery must be removed immediately.
Staphylococcal Scalded Skin Syndrome (SSSS)
Background
-
SSSS also known as Ritter's Disease of the Newborn
-
Ritter disease and staphylococcal epidermal necrolysis, encompasses a spectrum of superficial blistering skin disorders caused by the exfoliative toxins of some strains of S. aureus.
-
SSSS differs from bullous impetigo , the exfoliative toxins are restricted to the area of infection in bullous impetigo, and bacteria can be cultured from the blister contents.
-
Exfoliative toxins cause separation of the epidermis beneath the granular cell layer. Bullae and diffuse sheet -like desquamation occurs.
-
Exotoxin is a protein and is classified as either type A or B. Most are type A.
Clinical presentation
-
Fever, malaise, and irritability.
-
Most of the patients do not appear severely ill.
-
Tenderness to palpation.
-
Dehydration may be present and can be significant.
-
Nikolsky sign (gentle stroking of the skin causes the skin to separate at the epidermis.
-
Bacteremia may or may not present.
Diagnosis
-
Blood culture is usually negative in children (but positive in bullous impetigo) and is usually positive in adults.
-
A chest radiograph should be considered to rule out pneumonia as the original focus of infection.
-
A biopsy of the affected area will demonstrate separation of the epidermis at the granular layer.
Management
-
Fluid rehydration is initiated with Lactated Ringer solution at 20 mL/kg initial bolus.
-
Repeat the initial bolus, as clinically indicated, and followed by maintenance therapy with consideration for fluid losses from exfoliation of skin being similar to a burn patient.
-
Prompt treatment with parenteral anti-staphylococcal antibiotics is essential.
S. aureus Food Poisoning
Background
-
S. aureus is the most common cause of food poisoning in the USA
-
Eating from contaminated food containing preformed enterotoxin
-
Usually associated with meat, baked food filled with cream, and mayonnaise
-
Incubation period < 4–6 h
Clinical presentation
-
Nausea, vomiting, and abdominal cramps in few hours after exposure to contaminated food
-
Fever may be present
-
Some children can have severe dehydration
Management
-
Hydration
-
No antibiotic is required
Staphylococcal, Coagulase-Negative
Background
-
Staphylococcus epidermidis and Staphylococcus saprophyticus are example of coagulase-negative staphylococci
-
S. epidermidis is methicillin-resistant in most cases
-
S. epidermidis is the most common cause of catheter-related bacteremia
-
Catheter become contaminated when passing through the skin
-
S. epidermidis is a common contaminant in the blood cultures
Common source of infection
-
Skin, mucus membrane
-
Nosocomial infection
-
Intravenous catheter
-
Ventriculoperitoneal shunts
-
Prosthetic devices, e.g., heart valves, joints, and pacemakers
-
Bone marrow transplant
-
Premature infants (intravascular catheter)
Management
-
Removal of the foreign body may be necessary to clear the infection.
-
In neonatal intensive care unit (NICU), positive culture must be initially treated if a suspicious of infection.
-
Draw two cultures from two different sites to be considered positive, both culture should be positive within 24 h.
-
Vancomycin is the drug of choice.
Methicillin-Sensitive S. aureus (MSSA)
Background
-
Most of S. aureus strains produce beta-lactamase enzyme and are resistant to penicillin and ampicillin
Drug of choice
-
Nafcillin or oxacillin
Alternative drugs
-
Cefazolin
-
Clindamycin
-
Vancomycin
-
Ampicillin + sulbactam
Methicillin-Resistant Staphylococcus aureus (MRSA)
-
Background
-
MRSA strains are resistant to all beta-lactamase resistant (BLR) beta-lactam and cephalosporin antimicrobial agents as well as other antimicrobial agents.
-
-
Drug of choice in MRSA cases (oxacillin MIC, 4 ≥ µg/mL)
-
Vancomycin ± gentamicin or ± rifampin (multidrug resistance)
-
e.g., endocarditis, septicemia, and CNS infection (combination therapy is recommended)
-
-
Alternative drugs in MRSA cases (multidrug resistance)
-
Trimethoprim-sulfamethoxazole
-
Linezolid
-
Quinupristin/dalfopristin
-
Fluoroquinolones
Community (not multidrug resistance)
-
Vancomycin ± gentamicin (or ± rifampin) for life threatening infections, e.g., endocarditis.
-
Clindamycin (if strain susceptible) for pneumonia , septic arthritis, osteomyelitis, skin, or soft tissue infection.
-
Trimethoprim-sulfamethoxazole for skin or soft tissue infections.
-
Vancomycin.
-
Vancomycin-intermediately susceptible S. aureus.
Eradication of nasal carriage of S. aureus
-
Use mupirocin twice a day for 1–7 days.
-
Group B Streptococcus (GBS) or Streptococcus agalactiae
Background
-
Gram-positive diplococcus
-
Transmission
-
The primary reservoir in adults is the lower gastrointestinal tract, followed by the genitourinary tract.
-
The presence of GBS in the maternal genital tract at birth is the significant determinant of colonization and infection in the infant.
-
-
The most common maternal manifestations are asymptomatic bacteriuria, urinary tract infection (UTI) , bacteremia, chorioamnionitis, and endometritis.
Early onset disease (EOD)
-
Typically occurs within the first 24 h after birth but can occur up to 1 week of age.
-
Infants can present with a range of illness, from asymptomatic bacteremia to septic shock.
-
Respiratory symptoms, such as tachypnea, grunting, flaring, apnea, and cyanosis, are the initial clinical findings in more than 80 % of neonates.
-
Hypotension is present in 25 %.
-
Lethargy, poor feeding, temperature instability, abdom- inal distention, pallor, tachycardia, and jaundice .
Late onset disease (LOD)
-
Presents most commonly within the first 4–6 weeks after birth
-
Bacteremia without a defined focus remains the most common manifestation
-
Meningitis is more common in LOD than EOD
-
Pneumonia, cellulitis, and osteoarticular infections
Diagnosis of invasive GBS infection
-
Isolation of the organism from a normally sterile body site, such as blood or CSF
-
C-reactive protein level and white blood cell count, may be helpful
Management
-
Initial treatment for EOD usually is ampicillin plus gentamicin, until the identity of the pathogen is determined.
-
If meningitis is suspected, the ampicillin dose should increase 150–200 mg/kg/day and the gentamicin dose is 7.5 mg/kg/day.
-
The drug of choice for treatment of proven GBS infections is penicillin.
-
The recommended dosage for treatment of bacteremia without meningitis is 200,000 units/kg/day and increases to 300,000–500,000 units/kg/day for meningitis.
-
Length of treatment depends on the site of infection.
-
Bacteremia without a focus requires 10 days of therapy.
-
Meningitis requires a minimum of 14 days.
Prevention Guidelines
-
The drug of choice for intrapartum prophylaxis remains intravenous penicillin, with ampicillin as an acceptable alternative.
-
Both agents are given every 4 h until delivery, with at least one dose administered 4 h before birth.
S. pneumonia (Pneumococcal Infection)
Background
-
S. pneumoniae is a gram-positive, catalase-negative, alpha-hemolytic bacterium.
-
The bacteria are gram-positive diplococci (Fig. 8).
Fig. 8 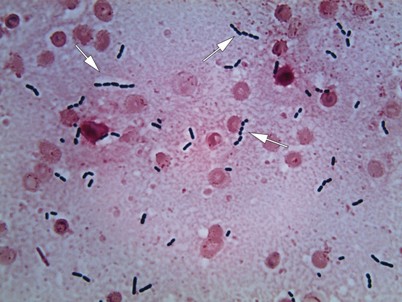
Streptococcus pneumoniae (pneumococci) in blood culture (gram stain, original magnification × 1000). The bacteria are gram-positive diplococci ( arrows). They are often lancet-shaped
-
Introduction of PCV7 and PCV13 significantly reduced invasive pneumococcal disease in children.

Risks of invasive pneumococcal disease (IPD)
-
The highest age-specific attack rates of IPD occur during the first 2 years after birth
-
Children who have sickle cell disease
-
Children who have asplenia
-
Congenital immune deficiencies
-
Immunosuppressive medications or bone marrow transplants also are at increased risk
-
CSF leaks, e.g., neurosurgical procedures or skull fractures
-
Cochlear implants
Clinical Manifestations
-
Common pneumococcal infections include:
-
AOM
-
Sinusitis
-
Pneumonia
-
Bacteremia (most common manifestation of invasive pneumococcal disease)
-
Meningitis (leading cause of meningitis)
-
-
Pneumonia
-
S. pneumoniae is the most common bacterial cause of community-acquired pneumonia in both children and adults
-
High fever and ill appearing
-
Cough and tachypnea
-
Respiratory distress
-
Crackles
-
Diminished breath sounds
-
Lobar consolidation may be noted on chest radiography in older children
-
Know that Infants and young children may have bronchopneumonia with a scattered distribution of parenchymal consolidation
-
Pleural fluid may be evident in some patients
-
Diagnosis
-
Pneumococcal infection is diagnosed with certainty by isolation of the organism from blood or normally sterile body fluids such as CSF, pleural, synovial, or middle-ear fluid.
-
Antigen detection.
-
Susceptibility test.
Treatment
-
Outpatient Pneumonia: Amoxicillin or amoxicillin-clavulanate in dosages recommended for AOM should be administered to children whose pneumonia is managed as outpatients .
-
Cefuroxime axetil and cefdinir also are effective empiric agents
-
-
Inpatient pneumonia Parenteral penicillin, ampicillin, cefuroxime, cefotaxime, and ceftriaxone are acceptable treatments for hospitalized children who have pneumonia.
-
Pneumococcal meningitis due to concerns about antibiotic resistance, the treatment of proven or suspected cases mandates empiric therapy with cefotaxime or ceftriaxone plus vancomycin .
Streptococcus pyogenes
-
Group A Streptococcus (GAS) is a gram-positive bacterium that grows in chains (Fig. 9).
Fig. 9 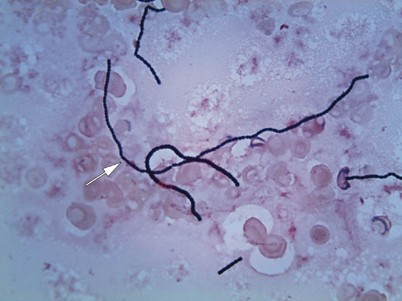
Streptococci in blood culture (gram stain, original magnification x1000). The bacteria are gram-positive cocci and grow in chains (arrow)

Group A Beta-Hemolytic Strepotococci (GABHS) Pharyngitis
Background
-
GAS is a gram-positive bacterium that grows in chains
-
The most common GAS infection
-
Most often in school-age children
-
Transmission results from contact with infected respiratory tract secretions
-
Close contact in schools and child care centers
-
The incubation period for GAS pharyngitis is 2–4 days
Clinical presentation
-
Sore throat, fever, headache , and abdominal pain is the most classic presentation
-
Nausea, vomiting may occur
-
Pharyngeal erythema and palatal petechiae (Fig. 10)
Fig. 10 
Streptococcal pharyngitis: palatal petechiae, rapid strep was positive in this patient
-
Inflammation of the uvula
-
Anterior cervical lymphadenopathy
-
Tonsillar exudates may or may not present

Diagnosis
-
Rapid antigen detection test is highly recommended to decrease overuse of antibiotics .
-
Testing of asymptomatic household contacts not recommended except when contacts are at increased risk of developing sequelae of GAS infection, e.g., rheumatic fever, poststreptococcal glomerulonephritis, or toxic shock syndrome.
-
If rapid antigen detection test (RADT) positive treat (specificity of 95 %).
-
If RADT is negative do throat culture (sensitivity of 65–90 %).
-
Treatment of GAS sore throat as long as 9 days after the onset of symptoms still effectively prevents rheumatic fever, initiation of antibiotics is seldom of urgent importance.
Treatment
-
Reduces complications.
-
Decrease the duration of infection.
-
Reduces transmission to others.
-
Oral penicillin V K (250–500 mg twice to three times a day for 10 days) is the antibiotic treatment of choice for GAS pharyngitis.
-
Amoxicillin (50 mg/kg, maximum 1 g, once daily for 10 days) often is used instead of oral penicillin because of its more palatable liquid formulation.
-
Cephalosporins or macrolides may be used as first-line therapy in patients allergic to beta-lactam antibiotics but otherwise are not recommended as first-line therapy.
Intramuscular penicillin G benzathine 600 000 U for children who weigh <27 kg and 1.2 million U for heavier children as single dose (if the adherence is a problem but is painful)
-
Know that treatment is indicated if a GAS carrier develops an acute illness consistent with GAS pharyngitis.
Treatment to eradicate GAS carriage indications
-
History of acute rheumatic fever
-
Close contact who has a history of rheumatic fever
-
Families experiencing repeated episodes of GAS pharyngitis
-
Eradication regimens include clindamycin, cephalosporins, amoxicillin-clavulanate
Indications for tonsillectomy include
-
More than seven documented GAS infections in 1 year or
-
More than five episodes in each of the preceding 2 consecutive years
-
Know that incidence of pharyngitis decreases with age
Scarlet Fever
Background
-
Scarlet fever (scarlatina) is a syndrome characterized by exudative pharyngitis, fever, and scarlatiniform rash.
-
It is caused by toxin-producing GABHS found in secretions and discharge from the nose, ears, throat, and skin.
Clinical presentation
-
Fever may be present.
-
Patient usually appears moderately ill.
-
On day 1 or 2, the tongue is heavily coated with a white membrane through which edematous red papillae protrude (classic appearance of white strawberry tongue).
-
By day 4 or 5, the white membrane sloughs off, revealing a shiny red tongue with prominent papillae (red strawberry tongue).
-
Red, edematous, exudative tonsillitis.
-
Diffuse, erythematous, blanching, fine papular rash that resembles sandpaper on palpation (Fig. 11)
Fig. 11 
Scarlet fever: fine erythematous punctate eruption with dry, rough texture to the skin that resembles the feel of coarse sandpaper and scarlet macules overlying the generalized erythema
-
The rash is prominent especially in the flexor skin creases of the antecubital fossa ( Pastia lines which pathognomonic for scarlet fever).
-
Circumoral pallor.
-
Desquamation after the rash starts to fade (usually the rash last about 1 week).

Diagnosis
-
Throat culture or rapid streptococcal test
-
Anti-deoxyribonuclease B and antistreptolysin-O titers (antibodies to streptococcal extracellular products)
Management
-
Penicillin remains the drug of choice (documented cases of penicillin-resistant group A streptococcal infections still do not exist).
-
First-generation cephalosporin may be an effective alternative.
Streptococcosis
-
Occur in children younger than 3 years
Young infants may not present with classic pharyngitis
-
Low-grade fever
-
Thick purulent nasal discharge
-
Poor feeding
-
Anterior cervical lymphadenopathy
-
Some patient may be toxic with high fever, malaise, headache, and severe pain upon swallowing
Impetigo
Background
-
GAS impetigo is a superficial bacterial skin infection (small percentage)
-
In North America the etiologic agent is primarily S. aureus
Clinical presentation: Fig. 12a and b

a Impetigo: honey crusted lesions under the nostril and on the cheek. b Impetigo: honey crusted lesions on the arm and trunk
-
Common (i.e., crusted or nonbullous) impetigo: Initial lesion is a superficial papulovesicular lesions that rupture easily.
-
The lesion becomes purulent and covered with an amber-colored crust.
-
Bullous impetigo: superficial fragile bullae containing serous fluid or pus forms and then ruptured to form a round, very erythematous erosions.
-
The lesions usually located in exposed area specially the face and extremities.
-
Lesions usually often spread due to autoinoculation.
Treatment
-
Topical mupirocin or retapamulin for localized lesions.
-
Multiple localized lesions may require systemic treatment that covers both GAS and staphylococcal infections, such as cephalexin or clindamycin.
-
Should not go back to school until at least 24 h after beginning appropriate antimicrobial.
-
Avoid close contact with other children if possible .
Perianal Streptococcal Dermatitis
Background
-
GABHS
-
It primarily occurs in children between 6 months and 10 years of age
-
It is often misdiagnosed and treated inappropriately
-
Early antibiotic treatment results in dramatic and rapid improvement in symptoms
Clinical presentation
-
Perianal rash, itching, and rectal pain; blood-streaked stools may also be seen in one third of patients.
-
Bright red, sharply demarcated rash around the anal area (Fig. 13).
Fig. 13 
Perianal Streptococcal Dermatitis: 4 years old present with rectal pain, itchiness, and discomfort when sitting, the PE shows, bright red, sharply demarcated rash around the anal area. Strep test was positive

Diagnosis
-
A rapid streptococcal test of suspicious areas can confirm the diagnosis.
-
Routine skin culture is an alternative diagnostic aid.
Management
-
Treatment with oral amoxicillin or penicillin is effective.
-
Topical mupirocin three times per day for 10 days.
-
Follow-up is necessary, because recurrences are common.
Erysipelas GAS
Clinical presentation
-
Erythema and edema
-
Sharply defined and elevated border tender to palpation
-
Systemic signs such as fever often are present
-
Lymphangitis may occur
Management
-
Systemic antibiotic therapy is required
-
Parenteral antibiotics may be needed, especially in immunocompromised patients
Acute Rheumatic Fever (ARF)
Background
-
ARF is caused by previous GAS pharyngeal infection
-
It is most common among children ages 5–15 years
Classified according to Jones criteria
-
Evidence of recent GAS infection
-
Positive throat culture or rapid strep test
-
Elevated or rising antistreptococcal antibody titer
-
-
Minor criteria
-
Fever
-
Arthralgia
-
Elevated acute phase-reactant
-
Prolonged PR interval
-
-
Major criteria
-
Arthritis (migratory polyarthritis in 75 % of cases)
-
Carditis or valvulitis
-
Erythema marginatum
-
Subcutaneous nodules
-
Sydenham chorea
-
Diagnosis
-
Evidence of a preceding GAS infection along with the presence of two major manifestations or one major and two minor manifestations
-
Streptococcal antibodies: antistreptolysin O (ASO), antihyaluronidase (AHase), and antideoxyribonuclease B (anti-DNase B) antibodies
Treatment of ARF
-
Eradication of GAS requires the same antibiotic regimens that are used to treat GAS pharyngitis
-
Household contacts should be treated if the cultures are positive for GAS
-
Aspirin 80–100 mg/kg/day and continued until all symptoms have resolved
-
Carditis is managed with therapies used for heart failure
-
Prophylactic antibiotics should be started immediately after the therapeutic antibiotic course is complete :
-
Penicillin V, sulfadiazine, or macrolides for patients at lower risk of ARF recurrence
-
Benzathine penicillin G IM every 4 weeks for patients at higher risk of ARF recurrence
-
Prophylaxis should continue for several years, typically until a patient is an adult and recurrence-free for 10 years
-
Longer prophylaxis is indicated if the patient has residual heart disease
-
Poststreptococcal Glomerulonephritis
Background
-
It is the most common cause of acute nephritis worldwide
Clinical presentation
-
Asymptomatic microscopic hematuria or
-
Nephritic syndrome
-
Hematuria
-
Proteinuria
-
Edema
-
Hypertension
-
Elevated serum creatinine values
-
Diagnosis
-
Urinalysis shows hematuria with or without red blood cell casts, proteinuria, and often pyuria
-
Serum C3 complement values are low
-
Negative throat or skin cultures at the time of diagnosis
-
Latent period from onset of infection to onset of nephritis
-
Treatment
-
Supportive management of the clinical manifestations.
-
Hypertension and edema:
-
Loop diuretics such as furosemide
-
Sodium and water restriction
-
-
Know that clinical manifestations of PSGN typically resolve quickly.
-
Serum creatinine return to baseline by 3–4 weeks.
-
Hematuria resolve within 3–6 months.
-
Proteinuria may persist for up to 3 years.
Prognosis
-
Excellent in most children
Streptococcal Toxic Shock Syndrome
Background
-
GAS TSS is a form of invasive GAS disease associated with the acute onset of shock and organ failure.
Risk factors
-
Injuries resulting in bruising or muscle strain.
-
Surgical procedures.
-
Varicella infection.
-
NSAIDs use.
-
Streptococcal exotoxins that act as superantigens, causes release of cytokines leading to capillary leak, leading to hypotension and organ damage.
Clinical presentation
-
Fever.
-
Abrupt onset of severe pain, often associated with a preceding soft-tissue infection, e.g., cellulitis or osteomyelitis
-
Know that patient may be normotensive initially, but hypotension develops quickly.
-
Erythroderma, a generalized erythematous macular rash may develop.
Diagnosis
-
Leukocytosis with immature neutrophils
-
Elevated serum creatinine values
-
Hypoalbuminemia
-
Hypocalcemia
-
Elevated creatine kinase concentration
-
Myoglobinuria, hemoglobinuria
-
Positive blood cultures
-
Diagnosis of GAS TSS requires isolation of GAS e.g., blood or CSF
Treatment for GAS TSS
-
Aggressive fluid replacement is essential to maintain adequate perfusion to prevent end-organ damage.
-
Vasopressors also may be required.
-
Immediate surgical exploration and debridement is necessary, and repeated resections may be required.
-
Empiric therapy with broad-spectrum IV antibiotics to cover both streptococcal and staphylococcal infections e.g.,:
-
Clindamycin IV plus penicillin G IV
-
-
Immune globulin intravenous (IGIV) also may be used as adjunctive therapy.
Pediatric Autoimmune Neuropsychiatric Disorder Associated with Group A Streptococci (PANDAS)
Background
-
PANDAS describes a group of neuropsychiatric disorders, in particular obsessive compulsive disorder (OCD), tic disorders, and Tourette syndrome, that are exacerbated by GAS infection.
Diagnostic criteria for PANDAS include:
-
Tourette syndrome; abrupt onset in childhood
-
Relationship between GAS infection and episodic symptoms confirmed by RADT, throat culture, or skin culture or serologic testing
-
Evaluation for GAS infection should be considered in children who present with the abrupt onset of OCD or tic disorder
Management
-
Treatment of the GAS infection and neuropsychiatric therapy
-
Behavioral therapy and pharmacological therapies, including:
-
Selective serotonin reuptake inhibitors (SSRIs) for OCD
-
Clonidine for tics
Necrotizing Fasciitis
Background
-
GAS necrotizing fasciitis is a form of invasive GAS disease. This infection is characterized by extensive local necrosis of subcutaneous soft tissues
-
GAS pyrogenic exotoxins that act as superantigens, which activate the immune system
Clinical presentation
-
Fever, hypotension, malaise, and myalgias
-
Rapidly increasing pain; and erythematous skin that progresses to blisters, bullae, and crepitus with subcutaneous gas.
Laboratory findings
-
Leukocytosis with a predominance of neutrophils
-
Elevated creatine kinase, lactate, and creatinine values
-
Positive blood cultures
Diagnosis
-
Diagnosis is clinical and requires a high degree of suspicion because of the rapid progression of infection.
Treatment
-
Early and aggressive surgical exploration and debridement
-
Antibiotic therapy with penicillin G IV plus clindamycin IV, and aminoglycoside as well is recommended
-
Hemodynamic support if GAS TSS is present as well
-
Repeat surgery is necessary until all necrotic tissue has been removed
-
Antibiotic therapy should continue for several days after completion of surgical debridement
Listeria monocytogenes
Background
-
Aerobic gram-positive bacillus
-
Mood of transmission
-
Unpasteurized milk
-
Soft cheese
-
Undercooked poultry
-
Prepared meat
-
Asymptomatic vagina carrier in pregnant women
-
Clinical presentation
-
Neonatal sepsis early onset < 7 days causes bacteremia or pneumonia
-
Neonatal sepsis late onset > 7 days causes meningitis
Treatment
-
Ampicillin and aminoglycoside
Corynebacterium diphtheriae
Background
-
Gram-positive pleomorphic bacillus
-
It is rare due to immunization against diphtheria
Clinical presentation
-
Low-grade fever
-
Sore throat
-
Malaise
-
Difficulty swallowing
-
Bilateral cervical lymphadenopathy
-
Grayish exudates over mucous membrane
-
Bleeding after attempting to remove the membrane
Treatment
-
Antitoxin should be started immediately if diphtheria is suspected called equine hyperimmune antiserum IV to neutralize the toxins.
-
Diphtheria toxins can cause myocarditis, necrosis, peripheral neuritis.
-
Airway obstruction and neck swelling (bull neck) can occur.
Know that close contact should receive single IM dose of penicillin G benzathine or oral erythromycin regardless their immunization status.
Enterococcus
Background
-
Gram-positive cocci.
-
Normal inhabitant of the gastrointestinal tract.
-
E. faecalis and E. faecium.
-
Most neonatal enterococcal infections are nosocomial and occur after second week of life, usually with bacteremia due to line infection or necrotizing enterocolitis (common symptoms in neonates include, fever, bradycardia, apnea, and abdominal distention).
Associated infections
-
Bacteremia in neonates
-
Catheter associated bacteremia
-
Endocarditis
-
Intra-abdominal abscess
-
UTI
Antibiotics
-
It is resistant to all cephalosporins and vancomycin as well
-
It is susceptible to aminoglycoside and linezolid
-
It is imperative to do sensitivity test because of increasing resistance
-
Sensitive enterococcal sepsis or endocarditis must be treated with vancomycin, PCN, ampicillin, in addition to gentamicin
Bacillus anthracis
Background
-
Large positive rods (bacilli) that cause anthrax
-
Types of anthrax: cutaneous anthrax, pulmonic and gastrointestinal
-
Inoculation occurs from handling contaminated substance, e.g., wool, and in the mail in cases of bioterrorism
Clinical presentation
-
Painless papules and ulcers
-
Painless black eschar with painless swelling and induration
Treatment
-
Penicillin G or quinolones, e.g., ciprofloxacin
Bacillus cereus
Background
-
It is a soil dwelling gram-positive rods, beta hemolytic bacterium.
-
Produces gastrointestinal symptoms due enterotoxin production in vivo in the GI tract.
Clinical presentation
-
Vomiting with incubation period 1–6 h (the emetic form is commonly associated with fried rice left at room temperature)
-
Diarrhea with incubation period 8–16 h
-
Eye infection after traumatic eye injuries in contact lens wearers
Diagnosis
-
It is usually clinical
-
B. cereus spores in stool
-
Isolated toxins from suspected food items
Treatment
-
Self limited and require no antibiotics
Arcanobacterium haemolyticum
Background
-
A. haemolyticum (can be mistaken with strep pharyngitis or scarlet fever)
-
Gram positive bacillus
-
Grows slowly as small colonies with narrow bands of hemolysis on blood-enriched agar
-
Growth enhanced by culture on rabbit or human blood with incubation in 5 % CO2
Clinical presentation
-
Common in teenagers and young adults
-
0.5–3 % of acute pharyngitis
-
Except for absence of palatal petechiae and strawberry tongue, the disease indistinguishable from that caused by group A Streptococcus
-
Fever
-
Pharyngeal exudates
-
Cervical lymphadenopathy
-
Scarlatiniform or maculopapular pruritic rash in 50 % of cases usually spares the palm and soles
Treatment
-
Macrolides: erythromycin or azithromycin
Anaerobes
Clostridium botulinum
Background
-
C. botulinum is an anaerobic gram-positive rod that survives in soil and marine sediment by forming spores.
-
Human botulism is caused by neurotoxins A, B, E, and occasionally F.
Infant botulism
-
Ingestion of honey or exposure to soils increases the risk
-
Age between 3 weeks and 6 months
-
Symptoms develop 3–30 days from the time of exposure
-
Clinical presentation
-
Constipation usually is the initial finding
-
Feeding difficulty is a common presenting symptoms
-
Hypotonia
-
Increased drooling
-
Weak cry
-
Truncal weakness
-
Cranial nerve palsies
-
Generalized weakness with ventilatory failure
-
-
Treatment of infant botulism
-
Botulism immune globulin (BIG) IV should be started as early as possible if clinically suspected.
-
No antibiotics.
-
Foodborne botulism
-
Background
-
Most common source is home canned food.
-
Symptoms develop 12–36 h after toxin ingestion.
-
Wound botulism is similar except the incubation period between 4 and 14 days.
-
-
Clinical presentation
-
Initial symptoms: dry mouth, nausea, and diarrhea
-
Bilateral cranial nerve palsies
-
Eye diplopia and blurring vision
-
Dysphagia
-
Upper extremity weakness
-
Respiratory dysfunction
-
Lower extremity dysfunction
-
-
Diagnosis
-
Stool toxins detection
-
-
Treatment of botulism in older patients
-
Equine trivalent antitoxin (Type A, B, and E)
-
Wound debridement for wound botulism is recommended
-
Clostridium perfringens
Background
-
Gram-positive, rod shaped, anaerobic, spore forming bacterium of the genus Clostridium
-
Spores found in raw meat and poultry
Clinical presentation
-
Sudden onset of diarrhea
-
Crampy abdominal pain
Management
-
Resolve with 24 h
-
No treatment is necessary
Clostridium tetani
Background
-
C. tetani, an obligate anaerobic gram-positive bacillus, is the pathogen responsible for tetanus.
-
It is nonencapsulated and form spores that are resistant to heat, desiccation, and disinfectants.
-
Contaminated deep puncture wounds , open wounds, soil, and animals (wool) containing spores are the most common sources of this bacteria.
Neonatal tetanus
-
Contaminated umbilical cord is a common source of infection.
-
Poor feeding (poor suck and swallowing due to muscle spasm).
-
Constant crying
-
Decreased movement
-
Spasm and rigidity
Generalized tetanus
-
Trismus (lockjaw)
-
Sardonic smile (risus sardonicus)
-
Severe muscle spasm
-
Opisthotonos (severe hyperextension)
-
Laryngeal spasm can lead airway obstruction and death
-
Tetanic seizure is severe tonic contractions with high fever
-
Diagnosis is always clinical
Treatment
-
Human tetanus immune globulin immediately
-
Penicillin G or metronidazole
-
Muscle relaxants
Prevention of tetanus
-
Routine immunization with Dtap and Tdap
Prevention in wound injuries guideline
-
Tetanus vaccine + /−Tetanus immunoglobulin (TIG)
-
Dirty wound, immunization is unknown or less than three tetanus shots: Give TIG + tetanus vaccine
-
Dirty wound, immunized > 5 years and < 10 years: Immunize, no TIG
-
Dirty wound, immunized < 5 years: No treatment
-
Clean wound, immunized < 10 years: No treatment
-
Clean wound, immunized > 10 years: Immunize, no TIG
-
Clostridium difficile
Background
-
Gram-positive anaerobes
-
Colonization
-
Around 50 % of infants younger than 1 year are colonized
-
Carriage decrease by 1–5 % by 2 years of age
-
-
Risk factor:
-
Having infected roommate or having symptomatic patient in the same ward
-
Antibiotics, e.g., beta-lactams drugs, clindamycin, and macrolides
-
Underlying bowel disease or surgeries
-
-
Symptomatic disease is due to toxins A and B produced by the organism
Clinical presentation
-
Asymptomatic colonization is common in infants and young children
-
Watery diarrhea
-
Abdominal cramps
-
Abdominal tenderness
-
In severe cases:
-
Systemic toxicity
-
Bloody diarrhea
-
Toxic megacolon, perforation or even death are complications of pseudomembranous colitis
-
-
Diagnosis
-
Documenting toxin A and B in stool (should be tested promptly or stored at 4 °C)
-
Endoscopic finding of pseudomembranous enterocolitis
-
Examination for occult blood is not diagnostic
-
In young infants you must consider other causes because they are colonized
Treatment
-
Oral or IV metronidazole
-
Oral vancomycin with or without metronidazole can be used in severe cases
-
Oral vancomycin can be used alone in those who do not respond to metronidazole
Prevention
-
Hand washing with water and soap
-
Know that alcohol based product are not effective in eradications of the organisms
-
Diluted bleach solution is the best for decontamination of surfaces
-
Limit antibiotic use
-
Infected child should be excluded from child care facility for the duration of diarrhea
-
Actinomycosis
Background
-
Actinomycosis is a subacute-to-chronic bacterial infection caused by filamentous, gram-positive, non acid-fast, anaerobic-to-microaerophilic bacteria.
-
It is characterized by contagious spread, suppurative and granulomatous inflammation, and formation of multiple abscesses and sinus tracts that may discharge sulfur granules.
Clinical presentation
-
The most common clinical forms of actinomycosis are cervicofacial (i.e., lumpy jaw) usually caused by dental infection.
-
In women, pelvic actinomycosis is possible when IUD in place.
Treatment
-
Initial therapy should include IV penicillin or ampicillin for 4–6 weeks followed by high dose of oral penicillin, clindamycin or doxycycline.
Gram Negative Bacteria
Gram Negative Anaerobes
Bacteroides and Fusobacterium anaerobes
Causes Variety of Clinical Manifestations Depending on the Location
-
Head and neck
-
Retropharyngeal abscess
-
Peritonsillar abscess
-
Dental abscess
-
Ludwig angina
-
-
CNS
-
Brain abscess
-
Subdural and epidural empyema
-
-
Lung
-
Aspiration pneumonia
-
Lung abscess
-
Pleural empyema
-
-
Abdomen
-
Peritonitis
-
Appendicitis
-
Intra-abdominal abscess
-
-
Skin and soft tissue
-
Infected bite wound
-
Necrotizing fasciitis
-
Cellulitis
-
-
Antibiotics with anaerobic activity
-
Clindamycin
-
Penicillin
-
Ampicillin-sulbactam
-
Amoxicillin-clavulanic acid
-
Metronidazole
-
Campylobacter species
Background
-
Campylobacter jejuni (gram-negative motile bacilli)
-
It is one of the most common agent associated with bacterial gastroenteritis
Common sources
-
Uncooked poultry (chicken and turkey)
-
Unpasteurized milk
-
Dogs and cats
Clinical presentation
-
Bloody diarrhea
-
Abdominal pain (may mimic inflammatory bowel disease in severe cases)
-
Tenesmus
-
Fever
Diagnosis
-
Stool culture in a selective media at temperature 42 °C incubated in gas mixture O2 and CO2
Azithromycin is the drug of choice
-
Antibiotic is recommended to shorten the duration of illness and prevent relapse
-
Chlamydophila pneumoniae
Background
-
C. pneumoniae is distinct antigenically, genetically, and morphologically from Chlamydia species
-
Transmitted from person to another via respiratory secretion
Clinical presentation
-
Patient may be asymptomatic or mildly to moderately ill
-
Illness is usually prolonged with cough persist for 2–6 weeks
-
Pneumonia and pulmonary rales
-
Acute bronchitis and bronchospasm
-
Less commonly nonexudative pharyngitis, laryngitis, otitis media, and sinusitis
Diagnosis
-
Chest radiography; may reveal an infiltrate
-
No reliable test to identify the organism is available
-
Fourfold increase in immunoglobulin (Ig) G titer or IgM titer of ≥ 16 is evidence of acute infection
Treatment
-
Macrolides or tetracycline
Chlamydophila psittaci
Background
-
C. psittaci is obligate intracellular bacterial pathogen.
-
Birds are major reservoir of C. psittaci, e.g., parakeets, and parrots, also animal such as goats and cows may become infected.
Clinical presentation (Psittacosis)
-
Fever
-
Nonproductive cough
-
Headache
-
Malaise
-
Extensive interstitial pneumonia can occur
-
Pericarditis, hepatitis, and encephalitis can occur (rare)
Diagnosis
-
Same as C. pneumonia
Treatment
-
Tetracyclines are preferred therapy except children less than 8 years of age
-
Macrolides, e.g., azithromycin
-
Chlamydia trachomatis
Background
-
It is the most frequently identified infectious cause of neonatal conjunctivitis; it is transmitted perinatally from infected mothers.
Clinical presentation
-
The symptoms typically develop 5–14 days after birth
-
Conjunctival edema
-
Hyperemia
-
Watery-to-mucopurulent discharge
-
A pseudomembrane may form and bloody discharge may be present if infection is prolonged
Management
-
Know that topical prophylaxis with erythromycin or silver nitrate given to all infants to prevent neonatal gonococcal conjunctivitis is ineffective against chlamydial conjunctivitis.
-
Important: when chlamydial conjunctivitis is diagnosed in an infant, the infant’s mother and her sexual partner(s) must be tested.
-
Treatment is erythromycin PO 50 mg/kg/day in four divided doses × 14 days.
Topical treatment alone is ineffective
-
Remember: untreated infections may result in corneal and conjunctival scarring.
Pneumonia due to C. trachomatis
Background
-
Small, gram-negative, obligate intracellular organisms .
-
Transmitted to the infant from the birth canal.
-
Generally presents as a subacute infection 2–19 weeks after birth.
-
C. trachomatis infection may cause neonatal conjunctivitis, nasopharyngitis, otitis media, and pneumonitis.
Clinical presentation
-
Rhinorrhea, congestion, or conjunctivitis
-
Tachypnea
-
Staccato cough
-
Crackles (rales)
-
Wheezing (rare)
-
Preterm infants may have episodes of apnea
Diagnosis
-
Chest radiography reveals infiltrates and hyperinflation
-
Laboratory testing may reveal:
-
Peripheral eosinophilia
-
Elevated serum immunoglobulins
-
-
A positive nasopharyngeal culture is considered diagnostic of infection
Treatment
-
Antibiotic treatment should be started presumptively on clinical grounds.
-
Oral erythromycin for 14 days or azithromycin, 20 mg/kg/day, once daily × 3 days.
-
If untreated, symptoms can last for months and include persistent hypoxemia.
-
Remember: Diagnosis of chlamydial pneumonia in an infant necessitates treatment of the infant’s mother and her sexual partner .
Trachoma
Background
-
This disease is a chronic keratoconjunctivitis caused by the obligate intracellular bacterium C. trachomatis.
-
Disease transmission occurs primarily between children and the women who care for them.
-
Trachoma is the most common infectious cause of blindness worldwide.
Clinical presentation
-
Chronic follicular keratoconjunctivitis with corneal neovascularization resulting from untreated or chronic infection.
-
Blindness occurs in up to 15 % of those infected.
-
Trachoma rarely occurs in the USA.
Diagnosis
-
It is a clinical diagnosis and nucleic acid amplification tests (NAATs) can confirm the causative agent.
-
The cicatricial phase has unique clinical features, which lead to definitive diagnosis in most cases.
Treatment
-
Azithromycin
Neisseria gonorrhoeae (Gonococcal Infections)
Background
-
N. gonorrhoeae is a gram-negative diplococcus.
-
Gonococcal infection is the second most common bacterial disease in the USA that is classified as a reportable and notifiable infection.
-
It is the highest in youth, especially females between 15 and 19 years of age.
-
The incubation period is 2–7 days.
-
A child abuse evaluation must be performed in any prepubertal case of gonococcal infection.
Neonatal conjunctivitis
-
Conjunctivitis due to mucosal transmission during vaginal delivery.
-
Topical antibiotics (erythromycin, silver nitrate, or tetracycline) to the eyes of a newborn within 1 h of birth can prevent the infection.
-
Treatment is ceftriaxone 125 mg IM × 1.
Gonococcal pharyngitis
-
Genital-oral activity is the major risk
-
Infection is asymptomatic in most cases
-
Patients who have gonococcal pharyngitis have a significant public health impact
-
Gonococcal pharyngitis are at risk for developing disseminated gonococcal infection (DGI)
-
Pharyngeal infection clears spontaneously within 12 weeks
-
Treatment is ceftriaxone 250 mg IM × 1
Gonococcal urethritis
-
Dysuria and a mucopurulent penile discharge
-
They may be coinfected with other sexually transmitted organisms, most commonly, C. trachomatis
-
Positive leukocyte esterase usually seen in urine specimen
-
Diagnosis of gonococcal urethritis
-
Presence of intracellular diplococci in urethral discharge
-
Treatment is ceftriaxone 250 mg IM × 1 plus azithromycin 1 g × 1
Epididymitis (gonococcus)
-
Dysuria and a mucopurulent discharge
-
Scrotal edema as well as scrotal, inguinal, or flank pain
-
Urinalysis may demonstrate WBCs
-
In most cases, this infection is transmitted sexually and may be an extension of urethritis
Gonococcal proctitis
-
Most cases of proctitis due to N. gonorrhoeae occur in homosexual males
-
Clinical presentation
-
Anal discharge
-
Rectal bleeding
-
Anorectal pain
-
Tenesmus
-
Constipation
Disseminated gonococcal infection (DGI)
-
DGI infection occurs in 0.5–3 % of people infected with N. gonorrhoeae
-
DGI usually cause an asymptomatic genital infection
-
Migratory arthritis (wrist, ankle, and knee) are the most common locations
-
Dermatitis
-
Tenosynovitis
-
Fever and chills may occur
-
Elevated white blood cell count
-
DGI occurs more commonly in females
Screening methods for infection N. gonorrhoeae and Chlamydia
-
Culture is the gold standard for diagnosing C. trachomatis.
-
Standard collection sites include the endocervix, male and female urethra, nasopharynx, conjunctiva, vagina, and rectum.
-
Nucleic acid amplification tests (NAATs) amplify nucleic acid sequences specific for the organism of interest.
-
The ease of using urine specimens, together with the high sensitivity of NAATs, has made these tests the preferred method for screening.
-
The presence of gram-negative intracellular diplococci on microscopy suggests the diagnosis of a gonococcal infection.
-
N. meningitidis (Meningococcal Infections)
Background
-
Aerobic gram-negative diplococcus N. meningitidis.
-
Natural commensal organism living in the nasopharynx of humans.
-
Children younger than 2 years of age have a nearly fivefold greater risk of contracting meningococcal disease than the general adult population.
-
Risk of transmission; crowded living conditions, e.g., college dormitories, military barracks.
Clue to clinician of invasive meningococcal infection
-
Rash
-
Any rash appearing in the context of a sudden febrile illness should raise concern
-
Meningococcal rash is typically present within 24 h of any symptomatology
-
Petechiae may be intraoral or conjunctival or be hidden in skinfolds
-
Early rash may not be petechial
-
-
True rigors
-
Shaking chill that cannot be stopped voluntarily
-
Prolonged (10–20 min)
-
-
Neck pain
-
Severe pain in the neck, back, or extremities
-
May manifest in younger children as refusal to walk
-
Meningismus: In patients older than 3 years, the classic signs of Kernig and Brudzinski may be elicited
-
-
Vomiting
-
May be associated with headache or abdominal pain without diarrhea
-
-
Cushing triads:
-
Bradycardia
-
Hypertension
-
Respiratory depression
-
-
Purpura fulminans (meningococcemia)
-
Aggressive spread of purpura to large areas with ischemic necrosis
-
Sudden drops in blood pressure
-
Acute adrenal hemorrhage (Waterhouse–Friderichsen syndrome)
-
Diagnosis
-
Culture of the organism from a normally sterile site is the gold standard for bacteriologic diagnosis.
-
Cerebrospinal fluid study:
-
CSF WBC counts are elevated in most patients who have meningitis.
-
CSF WBC counts are low or even normal if the disease is severe and rapidly progressive.
-
Markedly low glucose and elevated protein values are associated with the diagnosis of meningitis.
-
-
All patients with meningococcal disease or meningitis must be tested for CH50 or CH100 assay (20 % of children with meningococcal disease will end having a complement deficiency).
Management
-
Know that antibiotics or fluids should not be delayed for the sake of cultures or other testing.
-
Penicillin is effective treatment for both severe meningococcal septicemia (SMS) and meningococcal meningitis if the diagnosis is certain.
-
Broad-spectrum antibiotics effective against N. meningitidis and other potential pathogens are indicated (e.g., ceftriaxone, cefotaxime, vancomycin).
-
Emergency care evaluation and preferably transported via emergency medical services to allow for prompt delivery of intravenous fluids and airway management if the condition is suspected.
-
Large isotonic fluid boluses (20 mL/kg) over the first 5 min.
-
Inotropic/vasoactive agent such as dopamine or dobutamine.
-
Hydrocortisone may be beneficial in children who have SMS and respond poorly to vasopressors.
Prevention and indication of MCV4 (A, C,Y, and W-135)
-
MCV4 is routinely recommended at 11–12 years of age.
-
Unvaccinated adolescents through 18 years of age should receive a dose at the earliest opportunity.
-
Military recruits and all college freshmen who will be living in campus dormitories.
-
Persons who have terminal complement component deficiencies.
-
Anatomic or functional asplenia.
-
Note: 30 % of infections are due to serogroup B which is not covered by the vaccine.
-
Antibiotic prophylaxis, e.g., Rifampin, ciprofloxacin, azithromycin, or ceftriaxone should be used for contacts:
-
Child care contact
-
Direct exposure to oral secretions of individual with meningococcal disease (such as personnel providing mouth-to-mouth resuscitation)
-
Haemophilus influenzae
Background
-
Pleomorphic gram-negative coccobacillus.
-
Used to be the most common cause of meningitis and serious bacteremia in children.
-
Introduction of the H. influenzae vaccine quickly reduced the incidence of encapsulated H. influenza type b.
-
Nontypeable strains are still responsible for a large number of mucosal infections, including conjunctivitis , otitis media, sinusitis, and bronchitis.
Bacterial meningitis
-
Peak age is less than 1 year .
-
Mortality rate around 5 %.
-
Common complications include: subdural empyema, brain infarct, cerebritis, ventriculitis, brain abscess , and hydrocephalus.
-
Long-term sequelae occur in 15–30 % of survivors with sensorineural hearing loss, others include language disorders, intellectual disability (ID), and developmental delay.
-
Dexamethasone before or with antibiotics such as ceftriaxone or cefotaxime to prevent hearing loss and neurologic sequelae.
Epiglottitis
-
H. influenzae type b (Hib) was the predominant organism (> 90 %) in pediatric epiglottitis cases (other bacteria can cause epiglottitis as well, e.g., S. pneumoniae, group A beta-hemolytic streptococci, S. aureus, and Moraxella catarrhalis.
-
Occurs primarily in children (ages 2–7 years).
-
The clinical triad of drooling, dysphagia, and distress is the classic presentation.
-
Fever with associated respiratory distress or air hunger occurs in most patients.
-
Treatment in patients with epiglottitis is directed toward relieving the airway obstruction and eradicating the infectious agent.
-
Optimally, initial treatment is provided by a pediatric anesthesiologist and either a pediatric surgeon or a pediatric otolaryngologist.
-
Once the airway is controlled, a pediatric intensivist is required for inpatient management.
Buccal infections
-
Buccal cellulitis previously was always caused by H. influenzae infection before the vaccine.
-
Always associated with bacteremia if present.
-
Present with palpable cellulitis on both checks, purplish in color and child looks very toxic.
Periorbital cellulitis
-
Previously H. influenzae was the a common cause, now pneumococcus bacteria is the most common etiology
-
Minor trauma or insect bite of the eye lid usually associated with preseptal cellulitis due to S. aureus or a Group A Streptococcus
Pyogenic arthritis
-
H. influenzae was the most common cause of septic arthritis before Hib vaccine in children less than 2 years of age
Occult bacteremia
-
Occult bacteremia with H. influenzae will result in in 30–50 % developing meningitis or other deep, or focal infection from occult bacteremia.
-
All occult bacteremia from H. influenzae has to be treated immediately.
Pneumonia
-
Pneumonia from H. influenzae used to cause about one third of bacterial pneumonia before Hib vaccine and usually associated with pleural effusion, positive blood culture in most of the cases .
Treatment (Patient with life threatening illness)
-
Remember: the organism produces beta lactamase which makes amoxicillin is ineffective.
-
Cefotaxime or ceftriaxone is the antimicrobial of choice.
-
Meropenem or chloramphenicol is another option.
-
Amoxicillin is the drug of choice for noninvasive diseases such as otitis media or sinusitis, if amoxicillin fails, uses antibiotics against beta-lactamase-producing strains, e.g.,nontypeable H. influenzae including amoxicillin/clavulanic, TMP-SMX, azithromycin, cefuroxime axetil, cefixime, and cefpodoxime.
Rifampin antibiotic prophylaxis for contact with invasive H. influenzae type b infection
-
All household who did not receive immunization
-
Less than 4 years with incomplete immunization
-
Younger than 12 months who did not complete primary HIB immunization
-
Immunocompromised child
-
Nursery school and child care center if two or more cases within 60 days
Helicobacter pylori
Background
-
H. pylori is a gram-negative microaerophilic bacillus
-
It is spiral, curved, or U-shaped and has two to six flagella at one end under microscope
-
Transmission is fecal-oral, oral-oral from human-to human contact
Diagnosis
-
Know that AAP recommends testing only when treatment for H. pylori infection would be warranted.
-
Endoscopy remains the gold standard for evaluating H. pylori.
-
H. pylori stool antigen and urea breath test is a promising diagnostic tools.
-
Serologic tests for H. pylori are unreliable marker of disease.
Treatment indications
-
Endoscopically confirmed gastric or duodenal ulcer
-
Histologically proven gastric metaplasia
-
Gastric mucosa-associated lymphoid lymphoma (MALT)
-
Prior ulcer disease and current active infection
First-line: 14 days treatment regimens for children generally include
-
Clarithromycin (15 mg/kg/day divided twice a day, up to 500 mg per dose) with:
-
Either amoxicillin (50 mg/kg/day divided BID, up to 1 g per dose) or metronidazole (20 mg/kg/day divided BID, up to 500 mg per dose) and
-
Proton-pump inhibitor (PPI)
Mycoplasma pneumonia
Background
-
M. pneumonia is the leading cause of pneumonia in school age children and young adults
-
Infection is prevalent in person living in group setting
Clinical presentation
-
Pulmonary manifestations
-
Nonproductive cough
-
Chills
-
Scattered rales
-
Skin rash
-
Bilateral infiltrate on chest radiograph
-
-
Extrapulmonary manifestation
-
Pharyngitis
-
Rash
-
Stevens–Johnson syndrome
-
Hemolytic anemia
-
Arthritis
-
CNS disease (encephalitis, cranial nerve palsy (specially CNIII))
-
Testing for mycoplasma
-
IgG and IgM serology or cold agglutinin
-
Mycoplasma DNA PCR
Treatment
-
Mycoplasma lacks the cell wall and beta lactams are not effective
-
Azithromycin is the drug of choice
Pasteurella multocida
Background
-
Small gram-negative coccobacilli, it is a normal flora in number of animals, e.g., dog and cats.
-
Dog or cat bite is a common risk.
Clinical presentation
-
Erythema, tenderness, and edema usually develop rapidly within 24 h.
-
Infection occurs few days after the bite is usually caused by S. aureus.
Treatment
-
Clean the wound with soap and water.
-
Treatment should cover potential pathogens, e.g., P. multocida, S. aureus, and anaerobes.
-
Administration of antibiotic within 8–12 h of injury may decrease the risk of infection.
-
Amoxicillin-Clavulanate is the drug of choice
Ampicillin-sulbactam IV in severe cases
-
Clindamycin and TMP-SMX is appropriate for children allergic to penicillin.
Bordetella pertussis
Background
-
Pertussis is a small gram-negative coccobacillus that infects only humans.
-
Pertussis is spread by aerosol droplets expelled while coughing or sneezing in proximity to others.
-
Incubation period of 7–14 days.
Clinical presentation
-
Catarrhal phase
-
Lasts from 1 to 2 weeks
-
Mild fever
-
Cough
-
The cough worsens as the patient progresses to the paroxysmal phase
-
-
Paroxysmal phase
-
Lasts from 2 to 6 weeks
-
Rapid fire or staccato cough
-
Five to ten uninterrupted coughs occur in succession, followed by a “whoop” as the patient rapidly draws in a breath
-
May occur several times per hour
-
Can be associated with cyanosis, salivation, lacrimation, and posttussive emesis
-
Despite the severe spells, patients often appear relatively well between episodes
-
Whoop is usually absent in infants less than 6 months of age
-
Gasping, gagging, and apnea can occur
-
-
Convalescent phase
-
Decreasing frequency and severity of the coughing episodes
-
Lasts from weeks to months
-
Complications of pertussis
-
Pertussis is most severe in infants < age 6 months
-
Apnea
-
Pneumonia
-
Seizures
-
Encephalopathy
-
Death
Thoracic pressure related complications
-
Pneumothorax or pneumomediastinum
-
Subcutaneous emphysema
-
Superficial petechial hemorrhage
-
Rib fracture
-
Rectal prolapse
-
Intracranial hemorrhage
Diagnosis
-
PCR is beginning to replace culture as the diagnostic test of choice for B. pertussis in many clinical settings.
-
PCR for B. pertussis is a rapid, specific, and sensitive diagnostic test that will remain positive late in the course of the illness.
-
Leukocytosis as high as 60,000 can be seen.
-
Absolute lymphocytosis.
Management
-
Infants afflicted with pertussis often require hospitalization for fluid, nutritional, and respiratory support.
-
If left untreated, most individuals will clear B. pertussis spontaneously from the nasopharynx within 2–4 weeks of infection.
-
Antibiotics can shorten the course and attenuate the severity of pertussis if started early, and shorten the period of contagiousness as well.
-
Once the paroxysmal phase antibiotics are not effective in altering the course of the disease.
-
Azithromycin is the drug of choice:
-
Infant less than 6 months 10 mg/kg per day as single dose for 5 days
-
Older infants and children 10 mg/kg as a single dose on day 1 then 5 mg/kg per day as a single dose on days 2-5
Prophylaxis to close contacts is the same as the treatment
-
Infants less than 1 year
-
Pregnant women
-
Immunocompromised
-
Underlying lung disease
Immunization
-
Because immunity to pertussis from the DTaP series wanes over time, a booster dose is recommended at age 11–18 years.
Legionella pneumophila
Background
-
Gram-negative bacilli that requires a particular media to grow (enriched, buffered, charcoal yeast extract)
-
Legionella infection is rare in children
-
Legionella is an aerobic bacteria
-
Legionella is present in water
-
It is a multisystem disease
Clinical presentation
-
Fever
-
CNS symptoms; delirium and confusion
-
Pneumonia similar to mycoplasma; the CXR looks much worse than the exam
-
Treatment
Azithromycin
-
Quinolones and rifampin to severely ill patients
Brucellosis
Background
-
Brucellosis is a zoonotic infection caused by the bacterial genus Brucella.
-
Brucellosis caused by gram-negative bacillus.
-
The bacteria are transmitted from animals to humans by ingestion through infected food products, e.g., unpasteurized milk or cheese, direct contact with an infected animal, or inhalation of aerosols.
-
Brucella melitensis (from sheep; highest pathogenicity).
-
Brucella suis (from pigs; high pathogenicity).
-
Brucella abortus (from cattle; moderate pathogenicity).
-
Brucella canis (from dogs; moderate pathogenicity.
Clues to Brucella infection
-
Fever of unknown origin.
-
Culture negative endocarditis.
-
Individuals at greatest risk for brucellosis are those exposed to goats, sheep, cows, camels, pigs, reindeer, rabbits, or hares, both in areas of endemic disease and in areas where the disease is not endemic.
-
Bone/joint inflammation.
-
Orchitis.
-
Hepatic abscess.
-
CNS symptoms.
Diagnosis
-
Elevated liver enzymes is a common finding
-
Culture can take 4–6 weeks (alert laboratory if suspecting Brucella)
-
Serology is the most commonly used method for diagnosis
-
Point-of-care assays are available that offer fast and accessible diagnostic capabilities
-
PCR
Treatment
-
Doxycycline, gentamicin, streptomycin, rifampin, or trimethoprim-sulfamethoxazole (TMP-SMZ).
Bartonella henselae (Cat-scratch disease)
Background
-
B. henselae is gram negative rod or bacilli with a polar flagellum.
-
Kittens or cats less than 1 year old are most common source (no human to human).
-
Transmission can occur by petting alone with subsequent self-inoculation via a mucous membrane, skin break, or conjunctiva.
-
Clue for the diagnosis; contact with cats and lymphadenopathy.
Clinical presentation
-
Regional lymphadenopathy (cervical and axillary are common locations; Fig. 14)
Fig. 14 
Fourteen years old female with large tender axillary lymphadenopathy, she has kittens at home
-
Usually large and may be tender, warm and erythematous
-
Suppuration can occur in 30 % of cases
-
Node may remain enlarged for several months
-
Papule at the site of scratch may precedes the development of lymphadenopathy
-
-
Parinaud oculoglandular syndrome:
-
Painless nonpurulent conjunctivitis
-
Ipsilateral preauricular lymphadenopathy
-
-
Other clinical presentations
-
Fever of unknown origin (FUO)
-
Hepatic splenic microabscesses
-
Painful osteolytic lesions
-
-
Patients may recall being scratched, licked, or bitten by a cat in the previous 2–8 weeks
-
Fever, anorexia, headache, sore throat, or arthralgia may occur
-
Lymphadenopathy remains regional and typically resolves within 2–4 months but may last up to 6–12 months

Diagnosis
-
Indirect fluorescence assay (IFA) testing and Enzyme-linked immunoassay (ELISA) are used to detect serum antibody to B. henselae.
-
An antibody titer that exceeds 1:64 suggests recent Bartonella infection.
-
Lymph node biopsy generally is not indicated in typical cases of CSD.
Treatment
-
Cat-scratch disease is self limited.
-
Use of antibiotics is controversial and not indicated for typical CSD in immunocompetent patients.
-
Azithromycin, doxycycline, or rifampin may reduce the time for lymph node swelling to resolve.
-
Antipyretics and analgesics.
Surgical Treatment
-
Remember: Incision and drainage is not recommended (risk of sinus tract and persistent drainage).
-
Aspiration will be diagnostic and therapeutic; repeated aspirations may be performed if pus re-accumulates and pain recurs.
Citrobacter
-
Cause brain abscess in neonates
-
Order CT or MRI if CSF grow citrobacter otherwise is very rare disease
Klebsiella
-
It is a rare cause of pneumonia and meningitis.
-
It also can cause UTIs but is less common than E. Coli.
-
Most klebsiella are resistant to ampicillin.
Pseudomonas species
Background
-
Gram-negative organism
-
Found in the soil and freshwater
-
Gains entry through hair follicles or via skin breaks
Risk factors
-
Cystic fibrosis (see pulmonary chapter)
-
Associated with progressive deterioration of pulmonary function
-
-
Associated with hot tub folliculitis
-
Ocular infection from contaminated lenses
-
Puncture wound osteomyelitis
-
In immunocompromised patients, e.g., ecthyma gangrenosum
-
Hospitalized and debilitated patients
-
Burn
-
Ventilator associated pneumonia
Clinical presentation according to the site of infection
-
Pseudomonas key words
-
Nail-puncture wound through tennis shoes
-
IV drug abuse, with endocarditis, or osteomyelitis
-
Diabetes with otitis media
-
Leukemia with ecthyma gangrenosum
-
-
Hot tub folliculitis
-
Clinical presentation:
-
◦ The rash onset is usually 8 h to 5 days after exposure to contaminated water
-
◦ Erythematous pruritic macules that progress to papules and pustules
-
◦ Rash usually spares, face, neck, soles, and palms
-
◦ Usually confused with insect bites (history is important)
-
◦ Rash clears spontaneously within 2–10 days
-
-
Self limited require no antibiotics
-
Acetic acid 5 % compresses for 20 min twice a day for 4 days for symptomatic relief
-
Antimicrobial therapy
-
Piperacillin, ticarcillin
-
Ceftazidime (third generation)
-
Cefepime (fourth generation)
-
Carbapenems (e.g., meropenem, imipenem)
-
Aminoglycoside (gentamicin)
-
Aztreonam
-
Certain fluoroquinolones (ciprofloxacin, levofloxacin)
Nontyphoidal Salmonella
Background
-
Gram-negative bacilli that are usually motile bacteria
-
It is a common cause of diarrhea
-
Incubation period 6–72 h
Mode of transmission
-
Contaminated poultry, beef, eggs, fruits, vegetables, bakery and dairy products
-
Turtles, iguana and exotic reptiles
Clinical presentation
-
Can be asymptomatic
-
Most common presentation is gastroenteritis
-
Abrupt onset of fever, nausea, and vomiting
-
Abdominal cramps
-
Moderate to severe watery diarrhea are to most common manifestation
Diagnosis
-
Stool may show leukocytes, mucus, and blood.
-
CBC; leukocytosis and shift to the left.
-
The Patient can be a carrier after symptoms for 4–5 weeks.
Indication of antibiotic therapy
-
In infants less than 3 months
-
Infant < 12 months with temperature > 39 °C
-
Hemoglobinopathies, e.g., sickle cell anemia, HIV, and neoplastic diseases
-
Immunocompromised patients at any age
Typhoid fever
Background
-
Salmonella enterica, Serovar typhi ( S. typhi)
-
Mode of transmission
-
Poor sanitation and overcrowding
-
Spread by fecal-oral contamination of food or water by individuals who are carriers for S. typhi in either stool or urine
-
Typhoid is endemic in many developing areas
-
Clinical presentation
-
Fever “can exceed 104 °F (40 °C)”
-
Malaise
-
Chills
-
Headache, anorexia, myalgias, and dry cough may be seen
-
Abdominal pain is common
-
Diarrhea is more likely in children
-
Abdominal tenderness, hepatosplenomegaly, and a coated tongue
-
Rose spots (pink, blanchable maculopapular lesions that are 2–4 mm in diameter) are seen on the torso and abdomen
-
Know that neonatal typhoid generally presents within 3 days of birth with fever, emesis, diarrhea, abdominal distention, pronounced hepatomegaly, jaundice , and sometimes, seizures
-
Know that absence of abdominal or intestinal changes is not typical of typhoid
Diagnosis
-
Blood cultures are the mainstay of diagnosis
-
Stool culture
Treatment and Prognosis
-
Treatment includes:
-
Hydration and correction of fluid-electrolyte imbalance
-
Antipyretics and antibiotics
-
-
The choice of antibiotic as well as the route and duration depends on the host, site of infection, and sensitivities of the organism.
-
Multidrug resistant (MDR) strains, including resistance to ampicillin and TMP-SM have emerged.
-
IV cefotaxime or ceftriaxone for 14 days is appropriate.
-
For severe typhoid with obtundation, stupor, coma, or shock:
-
Two-day course of IV dexamethasone may be life-saving.
-
Shigella
Background
-
Shigella is a gram-negative bacilli
-
Shigella dysenteriae and Shigella flexneri usually cause bloody diarrhea
-
Shigella sonnei and Shigella boydii usually cause watery diarrhea
-
Ingestion of as few as 10 organism can cause diarrhea
-
Incubation period is 2–4 days
-
Outbreak can occur in child care centers
Mode of transmission
-
Person to person
-
Feco-oral
-
Ano-oral
-
House flies
-
Contaminated fomites
Clinical presentation
-
Range from mild diarrhea to life-threatening dysentery
-
Fever
-
Abdominal camps
-
High-volume watery stools
-
Small-volume bloody stool may follow 24–48 h later
-
Blood-mucoid stool is a common presentation
-
Rectal prolapse occurs in 5–8 %
Complications
-
Hemolytic-uremic syndrome
-
Seizures
-
Colonic perforation
-
Toxic encephalopathy
Diagnosis
-
Stool culture is diagnostic
-
Stool study with large number of neutrophil is suggestive but not specific
-
Peripheral WBCs are usually elevated; bandemia is very common
Treatment
-
Antimicrobial therapy is recommended for all patient with shigellosis.
-
Antimicrobial therapy for 5 days will shorten the duration and eradicate the organism from stool.
-
Oral ampicillin or TMP-SMX but the resistance makes them useless of Shigella infection.
-
Ceftriaxone, ciprofloxacin or azithromycin are usually effective.
-
Ciprofloxacin is not recommended if less than 18 years, if there is an alternative.
Daycare center
-
Once Shigella is identified in a daycare or household, all other symptomatic individuals in these environments should be cultured for Shigella as well.
-
Anyone found to have Shigella cannot return to daycare until the diarrhea has stopped and stool culture test is negative.
Escherichia coli
Background
-
E. coli is a gram-negative, lactose fermenting, motile rod, belonging to the Enterobacteriaceae.
-
E. coli is one of the most frequent causes of many common bacterial infections , including cholecystitis, bacteremia, cholangitis, urinary tract infection (UTI) , and traveler’s diarrhea, and other clinical infections such as neonatal meningitis and pneumonia .
Acute bacterial meningitis
-
The vast majority of neonatal meningitis cases are caused by E. coli and group B streptococcal infections .
-
Pregnant women are at a higher risk of colonization with the K1 capsular antigen strain of E. coli, which commonly observed in neonatal sepsis.
-
Low-birth weight and a positive CSF culture result portend a poor outcome.
-
Most survivors have subsequent neurologic or developmental abnormalities.
Pneumonia
-
E. coli respiratory tract infections are uncommon and are almost always associated with E. coli UTI .
Intra-abdominal infections
-
E. coli intra-abdominal infections often result from a perforated viscus (e.g., appendix, diverticulum) or may be associated with intra-abdominal abscess, cholecystitis, and ascending cholangitis.
-
They can be observed in the postoperative period after anastomotic disruption. Abscesses are often polymicrobial.
-
E. coli is one of the more common gram-negative bacilli observed together with anaerobes.
Enteric infections
-
Enterotoxigenic E. coli (ETEC) is a cause of traveler’s diarrhea; TMP-SMX is the drug of choice.
-
Enteropathogenic E. coli (EPEC) is a cause of childhood diarrhea; can be treated with TMP-SMX
-
Enteroinvasive E. coli (EIEC) causes a Shigella -like dysentery.
-
Enteroaggregative E. coli (EAEC) is primarily associated with persistent diarrhea in children in developing countries, and enteroadherent E. coli (EAEC) is a cause of childhood diarrhea and traveler’s diarrhea in Mexico and North Africa.
-
Enterohemorrhagic E. coli (EHEC) causes hemorrhagic colitis or hemolytic-uremic syndrome (HUS).
-
Strains of STEC serotype O157:H7 have caused numerous outbreaks and sporadic cases of bloody diarrhea and HUS.
E. coli (O157:H7)
Background
-
Gram-negative rods.
-
It occurs in all ages.
-
Transmitted via ingestion of contaminated food, e.g., (ground beef) or infected feces.
-
The disease linked to eating undercooked beef, and unpasteurized milk or apple juice.
-
Produces shiga toxins; the most virulent strain.
-
The incidence of E. coli O157:H7 > Shigella.
Clinical presentation
-
Usually begin as nonbloody diarrhea then become bloody
-
Severe abdominal pain is common
-
Fever in one third of the cases
-
May progress to hemorrhagic colitis in severe cases
-
Hemolytic uremic syndrome (HUS) may occur
Management
-
No antibiotic is proven to be effective and no prove that antibiotic increase the risk HUS.
-
No antibiotics are indicated.
-
Do not use antimotility agents.
UTIs
-
The urinary tract is the most common site of E. coli infection, and more than 90 % of all uncomplicated UTIs are caused by E. coli infection .
-
The recurrence rate after a first E. coli infection is 44 % over 12 months.
-
E. coli UTIs are caused by uropathogenic strains of E. coli. E. coli causes a wide range of UTIs, including uncomplicated urethritis, cystitis, pyelonephritis, and urosepsis.
Other miscellaneous E. coli infections:
-
Septic arthritis.
-
Endocarditis.
-
Soft tissue infections especially in patients with diabetes.
Yersinia enterocolitica
Background
-
Small-gram-negative coccobacillus
-
It produces entero and endotoxins
-
Pigs are commonly infected
-
Ingestion of raw or improperly prepared food, such as pork (pork intestine or chitterlings), contaminated unpasteurized milk, and water
Clinical presentation
-
Blood and mucus in stool
-
Fever
-
Right lower quadrant pain
-
Leukocytosis
-
Usually confused with appendicitis
Treatment
-
No treatment for isolated intestinal infection
-
If extraintestinal manifestation or immune compromised antibiotic is indicated
-
Cefotaxime, TMP-SMX (if older than 2 months), or aminoglycosides
Yersinia pestis
Background
-
Gram-negative coccobacillus that causes plague
-
Wild rodents are the reservoir
-
It is transmitted by flea or direct contact such as skinning the animals
-
Has a high mortality rate
-
Keyword (adenopathy and hunting) like tularemia
Clinical presentation
-
Localized lymphadenopathy “buboes” that suppurate
-
Bubonic type can lead to pneumonic form that rapidly transmitted by coughing to others
-
If not treated, it can lead to sepsis and death
-
Diagnosis
-
Lymph node aspiration or serology
Treatment
-
Gentamicin has been used successfully in the treatment of human plague
-
Doxycycline (as dosed for anthrax) is a recommended alternative in patients who cannot take aminoglycosides or in the event of a mass casualty scenario, making parenteral therapy unachievable.
Francisella tularensis
Background
-
Gram-negative pleomorphic bacillus that causes tularemia or “rabbit fever”
-
It is found in many animals specially the rabbits
-
Its transmitted by ticks and blood sucking flies
-
Organism can be ingested or inhaled
-
It is prevalent in Desert SW; Arkansas, Missouri, and Oklahoma
Clinical presentation
-
Fever, chills, myalgias, and arthralgias
-
Irregular ulcers at the site of inoculation
-
Lymphadenopathy that suppurate and form an ulcer
-
Oculoglandular tularemia (Unilateral conjunctivitis, corneal ulceration)
-
Pneumonic tularemia (Dry cough, dyspnea, and pleuritic-type chest pain)
-
Typhoidal tularemia—Fever, chills, myalgias, malaise, and weight loss
Diagnosis
-
Serology, e.g., ELISA or PCR
Treatment
-
Gentamicin or tetracycline
Prevention
-
Avoid tick-infested areas, check cloth for ticks and use tick repellents.
-
Avoid exposure to dead or wild mammals and wear gloves if such exposure is necessary; hands should be thoroughly washed afterwards.
Rocky Mountain Spotted Fever (RMSF)
Background
-
It is a tickborne rickettsial disease
-
Common in the Southeastern USA
-
Caused by Rickettsia rickettsii
Clinical presentation
-
Fever
-
Malaise
-
Headache
-
Abdominal pain
-
Myalgias
-
3–4 days later the rash will appear
-
Maculopapular rash start in the wrist and ankle spread centrally as well as palm and sole
-
Rash become petechial and purpuric
Laboratory
-
ELISA or indirect fluorescent antibody detecting immunoglobulin IgM and IgG to the organism
-
PCR is also available through CDC and prevention
Treatment
-
No need to wait to confirm the diagnosis to start treatment
-
Tetracycline particularly doxycycline is the treatment of choice even in children less than 8 years
-
Antibiotic is given for 5–7 days or at least 3 days after fever resolve
-
Best outcome if the treatment started within 5 days of illness
Complication
-
Vasculitis
-
DIC
-
Death
Ehrlichiosis
Background
-
Gram-negative cocci
-
Transmitted by tick bite
-
Monocytic ehrlichiosis (HME)
-
Granulocytic ehrlichiosis (HGE)
-
Common location
-
Southeastern and Southcentral USA
-
Clinical presentation
-
Similar to RMSF but usually without rash
-
Leukopenia
-
Neutropenia
-
Thrombocytopenia
-
Hyponatremia in most of the cases
-
Elevated liver enzymes
Treatment
-
Drug of choice is doxycycline (Table 2)
Borrelia burgdorferi (Lyme Disease)
Background
-
Tick-borne infection caused by spirochete B. burgdorferi
-
Transmitted by Ixodes species ticks in the nymphal stage
-
Commonly seen in the summer.
-
Common areas in the USA are Northeast to mid-Atlantic, e.g., Connecticut, New York, and New Jersey
Early localized disease stage I
-
Erythema migrans (pathognomonic skin lesion) either bullseye or clear center
-
Myalgia
-
Arthralgia
-
Fever
Early disseminated disease stage II (weeks-months later)
-
Recurrent erythema migrans (rare)
-
Meningitis (lymphocytic)
-
Cranial nerve palsies, e.g., Bell palsy
-
Peripheral neuropathy, e.g., foot drop
-
Heart block; first, second, or third degree heart block
Late disseminated disease stage III
-
Arthritis
-
Oligo-migratory arthritis
-
Remember: Lyme disease can be confused with Juvenile rheumatoid arthritis
Diagnosis
-
Erythema migrans is pathognomonic and is an early lesion and antibodies not developed yet.
-
No need to test the patient in order to treat in the first few weeks.
-
-
Serologic testing is to confirm the diagnosis in stage two or three or in atypical cases.
-
Initial test is sensitive enzyme immunoassay assay (EIA); high false positive rate.
-
Confirm with western blot test.
Treatments
-
Isolated Bell palsy or erythema migrans
-
Amoxicillin if < 8 years old
-
Doxycycline 100 mg bid if > 8 years old
-
-
Cardiac and neurologic complications:
-
Ceftriaxone 75-100 mg/kg/day
-
Treponema pallidum
Background
-
TP is spirochete mobile bacteria
-
Mode of transmission:
-
Sexual contact
-
Perinatal
-
Exposure to infected blood or tissue
Clinical presentation
-
Primary syphilis
-
Genital chancre
-
It is a painless papule, and then become painless ulcer, which is very contagious
-
-
Secondary syphilis 2–10 weeks after the chancre heals
-
Maculopapular rash involve the palm and sole
-
Condyloma lata (wart like plaques around the anus or the vagina)
-
Generalized lymphadenopathy
-
-
Tertiary syphilis (symptomatic late syphilis)
-
Cardiovascular, CNS, gummatous lesions
-
Diagnosis
-
Screening methods:
-
RPR (rapid plasma reagin) and VDRL correlates with disease activity
-
EBV infection can cause false positive results
-
-
FTA-ABS confirm the diagnosis and this test remain positive for life
Treatment
-
Penicillin
-
Doxycycline or tetracycline if allergic to penicillin
-
Congenital syphilis (see chapter The Fetus and Newborn Infants)
Leptospirosis
Mode of transmission
-
Swimming with dog or contact with fresh water contaminated with the urine of an animal that is a chronic carrier, e.g., rats.
Clinical presentation
-
Fever
-
Headache
-
Elevated liver enzyme
Diagnosis
-
Early blood culture, later in the disease urine culture may show the organism
Treatment
-
Penicillin or doxycycline
Mycobacterium tuberculosis
Background
-
M. tuberculosis, a tubercle bacillus, is the causative agent of TB.
-
Mycobacteria, such as M. tuberculosis, are aerobic, non spore-forming, non motile, facultative, curved intracellular rods measuring 0.2–0.5 μm by 2–4 μm.
-
It retains many stains after decolorization with acid-alcohol, which is the basis of the acid-fast stains used for pathologic identification.
-
TB is transmitted most commonly via airborne spread.
-
Kissing, shaking hand, and sharing food do not spread the infection.
-
-
TB is unlikely to spread from child to another child < 4 years of age.
-
TB is likely to spread from infected adult to children (usually household or daycare).
Risk factors
-
Foreign-born individuals in the USA have TB rates 9.5 times higher than those in the US-born persons
-
Immigrants from Mexico, Philippines, Vietnam, China, and India
-
Untreated HIV infection
-
Immunocompromising conditions
-
Recent latent tuberculosis infection (LTBI)
-
Intravenous drug use
-
Certain medical conditions such as diabetes and renal failure
Clinical presentation
-
Only 5–10 % of children older than 3 years of age who have untreated LTBI progress to disease.
-
Most LTBI progress to disease within 1–2 years of initial infection.
-
The most common site of infection is the lung, which accounts for up to 80 % of all cases of disease.
-
Pulmonary Disease
-
Infants and adolescents are more likely to be symptomatic than 5–10-year-old children
-
Cough (usually last 3 weeks or longer)
-
Hemoptysis
-
Low-grade fever
-
Weight loss (rare)
-
Night sweat
-
Loss of appetite
-
Hilar or mediastinal adenopathy may be seen
-
Cavity lesions
-
-
Superficial lymphadenopathy:
-
The most common extrapulmonary form of TB.
-
Children who have TB lymphadenopathy tend to be older than those who have nontuberculous mycobacterial lymphadenopathy.
-
Common locations: anterior cervical, followed by posterior triangle, submandibular, and supraclavicular.
-
LNs usually measure 2–4 cm and lack the classic inflammatory findings of pyogenic nodes.
-
There may be overlying violaceous skin discoloration.
-
Surgical node excision is not curative but may be necessary to establish the diagnosis.
-
Most children respond well to a 6-month course of multidrug therapy, but occasionally therapy must be extended to 9 months, based on clinical response.
-
-
CNS disease
-
Tuberculomas, occurring in 5 % of children who have CNS TB, appear as a single rim-enhancing lesions ranging from 1 to 5 cm.
-
In TB meningitis, CSF analysis typically demonstrates lymphocytes, a low-glucose concentration, and a high-protein value.
-
The most common findings on CNS imaging:
-
◦ Hydrocephalus and Basilar enhancement.
-
◦ Vascular lesions involving the basal ganglia and midbrain also are common.
-
-
TB should be considered in cases of childhood stroke.
-
-
Pleural TB
-
More seen in older child and adolescent.
-
Can occur in isolation or concomitantly with pulmonary parenchymal disease.
-
Symptoms include chest pain, fever, cough, dyspnea, and anorexia.
-
Auscultatory findings mimic those of bacterial pneumonia.
-
Most children have positive TST results.
-
Effusions are more common on the right and rarely bilateral.
-
The pleural fluid is exudative and lymphocytic.
-
A 6-month course of therapy is recommended.
-
-
Miliary tuberculosis
-
Due to lymphohematogenous spread, it is a disease of the young or immunocompromised children.
-
Miliary disease can present shortly after primary infection.
-
Multiorgan involvement is common.
-
Clinical presentation:
-
◦ Pyrexia.
-
◦ Hepatomegaly and splenomegaly.
-
-
The TST is insensitive in these patients because disseminated disease can produce TST anergy.
-
AFB culture from gastric aspirates can have a yield as high as 50 %.
-
A prolonged course of therapy (9–12 months) should be administered to patients who have disseminated disease.
-
-
Skeletal TB
-
The most common manifestations of skeletal disease are:
-
◦ Spondylitis.
-
◦ Arthritis.
-
◦ Osteomyelitis.
-
-
Most patients are in the second decade of life.
-
Spinal involvement (Pott disease), which can affect even young children.
-
Skeletal lesions can develop more than 10 years after initial infection.
-
Magnetic resonance imaging is the preferred imaging choice because it can demonstrate lesions months before plain radiographs.
-
Chest radiographs are positive in 50 % of children who have skeletal TB.
-
TST results are usually positive.
-
-
Other Forms TB include
-
Abdominal
-
Renal
-
Cutaneous disease
-
TB testing
-
Cultures can be obtained by sequential sputum sampling or by gastric aspiration of early morning secretions in the younger child
-
The bacillus grows slowly
-
6–8 weeks to grow on Lowenstein-Jensen media
-
2–3 weeks to grow in liquid media
-
-
AFB stains include Kinyoun, auramine-rhodamine (Truant), and Ziehl-Neelsen
-
Truant stains are the most sensitive
-
-
Tuberculin skin test (TST) (Table 3)
-
It is measured in millimeters of induration (not erythema).
-
Reading is 48–72 h after placement.
-
Know If a child returns for TST interpretation after 72 h and has induration meeting the criteria for positivity.
-
A negative result never eliminates the possibility of TB disease because many disseminated forms of TB, including TB meningitis can induce anergy to the skin test
Table 3 Positive tuberculin test reaction results in infants, children, and adolescents -
-
False-negative TST results:
-
Recent measles infection
-
High-dose corticosteroid treatment, irradiation
-
Immunosuppressive therapy
-
Immunocompromising medical conditions
-
-
A false-positive TST result:
-
Primarily in children exposed to nontuberculous (environmental) mycobacteria
-
Children recently received a bacillus Calmette-Guérin (BCG) vaccine
-
A boosting phenomenon: children received multiple sequential TSTs
-
It is recommended that children be screened for risks of exposure to TB by history initially
-
-
-
BCG vaccine
-
TST can be interpreted normally in a child who received a single dose of the BCG vaccine as a young child
-
Having received a BCG as an infant may not explain a positive skin test result later in life
-
The assumption that BCG receipt is the cause of a positive TST could lead to a lack of treatment for high-risk children who potentially could benefit from LTBI therapy
-
-
Whole blood interferon-gamma release assays (IGRAs)
-
These assays have several potential advantages:
-
Only one office visit is required.
-
There is no risk of the boosting phenomenon.
-
More specificity for LTBI because the antigens in the IGRAs are shared less commonly with nontuberculous mycobacteria and are not found on BCG.
-
-
This test cannot distinguish LTBI from TB disease.
-
-
Chest radiographs
-
Children who have LTBI usually have normal-appearing chest radiographs.
-
An isolated calcified lesion in a child who has a positive TST result can be treated as LTBI.
-
The most common abnormal radiographic finding is hilar or mediastinal adenopathy.
-
Other findings can include infiltrates, atelectasis, pleural effusions, cavities, or miliary disease.
-
TB exposure
-
Children younger than 4 years of age and immunocompromised children
-
Should be started on medication, usually isoniazid (INH), pending results of repeated skin testing.
-
If the second skin test result is negative, medication can be discontinued.
-
-
Children experiencing TB exposure who are older than age 4 years and immunocompetent can be observed off medications pending the second skin test result in 2-3 months
TB infection (LTBI)
-
The child demonstrating a positive skin test result should be treated for LTBI to decrease the risk of disease progression later in life.
-
The mainstay of therapy for LTBI is INH administered for a 9-month course.
-
An alternative for patients intolerant of INH is rifampin, which is administered for 6 months.
Treatment of TB
-
The standard initial regimen:
-
INH, rifampin, pyrazinamide (PZA), and ethambutol.
-
INH, rifampin, and ethambutol are administered for 6 months and PZA is stopped after the first 2 months.
-
If the source case’s isolate is known to be susceptible to the other three drugs, ethambutol need not be given.
-
These medications are efficacious, available in oral formulation, and well-tolerated by children.
-
-
The usual treatment duration for pulmonary and most extrapulmonary forms of TB is 6 months for isolates that are susceptible to all first-line TB drugs.
-
Exceptions are treating children who have disseminated or CNS TB, where treatment courses of 9–12 months often are used; children infected with MDR-TB.
-
Give vitamin B6 (pyridoxine).
-
Children coinfected with TB and HIV.
-
Initial therapy should include four drugs, if possible.
-
Side effects of antituberculous medications
-
INH, rifampin, and PZA are all hepatotoxic
-
Ethambutol can cause decrease in visual activity (decrease color perception is the first sign of deterioration).
-
Streptomycin can cause oto-nephrotoxicity.
Challenging clinical scenarios
-
Adult in the household has infectious TB
-
All children in the household should have chest radiographs and TSTs performed.
-
Children younger than 4 years of age should be started empirically on INH until the TST is repeated in 2–3 months.
-
If the second TST result is negative and the child is immunocompetent, INH can be discontinued.
-
If the TST result is positive or the child is immunocompromised, INH should be continued for 9 months.
-
-
Infant whose mother has TB
-
The TST is helpful only if the result is positive, which is very rare.
-
If the mother has a positive TST result and negative chest radiograph (LTBI), the child needs no evaluation.
-
If the mother has radiographic features consistent with TB, the neonate requires evaluation for congenital TB.
-
If the infant does not have congenital TB, he or she should be separated from the mother until the infant is receiving INH and pyridoxine (if the mother is breastfeeding) and the mother is receiving appropriate multidrug therapy.
-
Once the infant is receiving INH, separation is unnecessary and breastfeeding should be encouraged unless INH resistance is suspected.
-
-
Health-care workers (HCWs)
-
If positive TST results they should receive chest radiographs.
-
If the chest radiograph is negative, the HCW may be offered therapy for LTBI after weighing the risks and benefits of INH in adults.
-
If the chest radiograph is positive, the HCW needs to be evaluated further.
-
Follow-up
-
Children who have TB disease should be seen monthly while receiving therapy to document medication tolerance and adherence, weight gain, and achievement of appropriate milestones.
Mycobacterium avium-intracellulare
Background
-
Mycobacterium avium-intracellulare complex is the most common cause of nontuberculous disease in children
-
Usually occur in children with impaired cell immunity
-
Exposure to ubiquitous soil
Clinical presentation
-
Cervical lymphadenitis
-
Overlying skin is usually pink to violaceous
-
Usually unilateral
-
Increase in size over several weeks
-
-
Cutaneous infections
-
Ear infections
-
Disseminated infections (high fever, night sweats, weight loss, lymphadenopathy, abdominal pain, diarrhea, and anemia)
-
Osteomyelitis
-
Pulmonary diseases
Management
-
Complete resection of infected lymph node is diagnostic and curative
-
Azithromycin in combination ethambutol or rifampin
Nocardia
Background
-
Nocardia are weakly gram-positive, beaded and filamentous bacteria found worldwide in soils
-
It is hard to isolate
Clinical presentation (it may present with any of the following)
-
Thin walled cavitary lung lesions
-
Focal brain abscess
-
Neutrophilic chronic meningitis
-
Nodular skin lesions
Treatment
-
High-dose sulfonamide or TMP-SMX
-
In severely ill patients combination of drugs can be used; amikacin plus imipenem
Fungal Infections
Candida Species
-
Candida albicans is the most commonly isolated species, and cause infections (Candidiasis or thrush).
-
Systemic infections of blood stream and major organs (invasive candidiasis or candidemia, particularly in immunocompromised patients.
-
Candida appears as budding yeast cells and pseudohyphae (Fig. 15).
Fig. 15 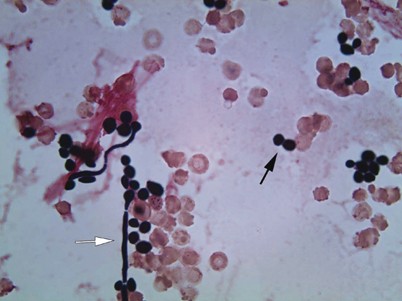
Candida albicans in blood culture (gram stain, original magnification × 1000). Budding yeast cells (blastoconidia, black arrow) and pseudohyphae ( white arrow)

Oral Thrush
Background
-
Common is the first 6 postnatal months
-
Possibly due to infants’ immunologic immaturity
Infection sources
-
Contaminated bottle nipples, pacifier, or dropper, e.g., vitamin dropper.
-
Infected mother’s nipples (although the incidence is high in formula fed infants).
-
Maternal vaginal colonization with Candida.
Recognize
-
Recurrent or persistent oral thrush beyond 6–12 months raises the concern of immunodeficiency, especially if associated with failure to thrive or hepatosplenomegaly.
Risk of infection
-
Use of inhaled steroid without adequate rinsing afterward or oral antibiotics can cause oral thrush.
-
Poorly controlled diabetes in adult can cause candida infection however is not associated with gestational diabetes.
Clinical presentation
-
Infant may have trouble feeding in severe cases.
-
Tiny focal white area that enlarge to white patches on oral mucosa (Fig. 16).
Fig. 16 
Thrush: Tiny focal white areas that enlarge to white patches on oral mucosa, it was difficult to remove the white spots with the tongue blade
-
If scraped with a tongue blade, lesions are difficult to remove and leave behind an inflamed base that may be painful and may bleed.
-
Examine the patient with diaper dermatitis for oral lesions.

Treatment
-
Oral nystatin.
-
Once-daily oral fluconazole is superior to oral nystatin for resistant thrush and effective candidal diaper dermatitis.
Candidal Diaper Dermatitis
Clinical presentation
-
Lesions consist of beefy-red plaques, often with scalloped borders.
-
Satellite papules and pustules may be observed surrounding the plaques (Fig. 17).
Fig. 17 
Candidal diaper rash: lesions consist of beefy-red plaques, with satellite papules
-
Maceration is often present, especially in intertriginous areas.

Treatment
-
Once-daily oral fluconazole is superior to oral nystatin for resistant thrush and effective candidal diaper dermatitis.
-
Topical clotrimazole if resistant to topical nystatin.
Vulvovaginitis
Background
-
Common in pubertal and adolescent girls
-
Risk factors
-
Oral antibiotics
-
Oral contraceptive
-
Pregnancy
-
Poor hygiene
-
Diabetes
-
Clinical presentation
-
Vulvar/vaginal erythema, and itching
-
White, cottage cheese like vaginal discharge
Treatment
-
Topical nystatin or clotrimazole
-
Single dose of oral fluconazole
Candidal Infections in Neonates
Background
-
Very low-birth weight
-
Prolonged venous catheter (obtain culture from the catheter)
Treatment
-
Remove the catheter
-
Parenteral amphotericin (lipid-complex formulation (less nephrotoxic))
-
Monitor for hypokalemia
-
Aspergillus
Background
-
Aspergillus species is ubiquitous molds found in organic matter.
-
Most common species affect the human is Aspergillus fumigatus and Aspergillus niger.
Mode of transmission
-
Inhalation of fungus spores
Clinical presentation
-
Underlying asthma or cystic fibrosis
-
May presents with fever and pulmonary infiltrates not responsive to antibiotics (allergic bronchopulmonary aspergillosis)
-
Patient may cough mucous plug
-
-
Underlying preexisting cavities, e.g., TB, sarcoidosis, or CF
-
Aspergilloma or fungal ball, it may cause hemoptysis
-
-
Allergic fungal sinusitis
-
Present with purulent discharge and unilateral opacity
-
-
Immunocompromised patient may present:
-
Fever, cough, dyspnea, pleuritic chest pain, and hemoptysis
-
Diagnosis
-
Elevated IgE level
-
Deterioration of lung function and increase in sputum production in chronically ill patients, e.g., CF or asthma
-
Peripheral eosinophilia
-
Sputum culture
-
Bronchoalveolar lavage (BAL)
-
CT scan
Treatment of allergic pulmonary aspergillosis
-
Oral steroids
Cryptococcosis
Background
-
Infection with the encapsulated yeast Cryptococcus neoformans can result in harmless colonization of the airways
-
It can also lead to meningitis or disseminated disease, especially in persons with defective cell-mediated immunity.
-
Cryptococcosis represents a major life-threatening fungal infection in patients with severe HIV infection and may also complicate organ transplantation, reticuloendothelial malignancy, corticosteroid treatment, or sarcoidosis.
Clinical presentation
-
Severity of symptoms and presentation depends on the immune status and the affected organs
-
Pulmonary; cough, pleuritic chest pain, fever, dyspnea, weight loss, and malaise
-
Meningitis; headache, lethargy, confusion, seizures, and coma
-
Skin; papules, pustules, nodules, ulcers, or draining sinuses
Diagnosis
-
Cutaneous lesions: Biopsy with fungal stains and cultures.
-
Blood: Fungal culture, cryptococcal serology, and cryptococcal antigen testing.
-
Cerebrospinal fluid: India ink smear, fungal culture, and cryptococcal antigen testing.
-
In AIDS patients with cryptococcal pneumonia , culture of bronchoalveolar lavage washings.
Treatment for cryptococcal meningitis
-
Amphotericin B, and flucytosine for 2 weeks
-
Flucytosine speeds clearance of viable yeast from CSF but is potentially toxic, especially in patients with renal dysfunction
-
Then fluconazole for 8-10 weeks
Malassezia furfur
Overview
-
Can cause tinea versicolor (see skin disorders)
-
Can cause neonatal infection in NICU babies receiving TPN with lipids
-
NICU babies with M. furfur may present with fever, bilateral interstitial infiltrates, and increased WBCs
-
M. furfur requires olive oil overlay to grow
Management of infection in Neonates
-
Removal of catheters
-
Stop lipid infusion
-
Start amphotericin B or fluconazole
Histoplasmosis
Background
-
Endemic areas: Ohio, Missouri, and Mississippi River valleys
-
Mode of transmission
-
Inhalation of spores from birds excreta or contaminated soil
-
No person to person transmission
-
Clinical presentation
-
Flu like symptoms
-
Pulmonary infiltrates
-
Hilar lymphadenopathy with or without calcifications
-
Erythema nodosum
-
In younger children may develop progressive disseminated histoplasmosis
Treatment
-
Amphotericin B
Coccidioides (Coccidioidomycosis)
Background
-
Endemic areas
-
California, Arizona, New Mexico, and Texas
-
-
Mode of transmission
-
Inhalation of airborne spores
-
Clinical presentation
-
Most cases are asymptomatic
-
-
Fever
-
Cough
-
Weight loss (common)
-
Fatigue
-
Shortness of breath
-
Chills
-
Erythema nodosum
-
Night sweat
-
-
Mild respiratory distress or respiratory failure in severe cases
Diagnosis
-
Culture and DNA probe is the most definitive method for the diagnosis
-
High index of suspicion is important in patient who travelled or underlying medical conditions
-
Elevated ESR
-
Lymphocytosis and monocytosis
-
Eosinophilia > 5 %
-
Chest radiography may show consolidations and hilar lymphadenopathy
Treatment
-
Amphotericin B in Severe disseminated disease
-
Fluconazole for CNS infections
Blastomyces
-
Blastomyces causes illness similar to Histoplasma and Coccidioides
-
It is seen in Arkansas and Wisconsin hunters and loggers
-
Outbreak occurred in kids visited Wisconsin lodge and beaver dam
-
Blastomyces may disseminate to the skin and cause crusted skin lesions
-
Bone lesion more common with blastomycosis
-
Itraconazole or amphotericin B is the treatment of choice depending on the severity
Sporotrichosis schenckii
-
Common in florists
-
Symptoms may take from 7 to 30 day after inoculation
-
Present with painless papule at the site of inoculation then ulcerates
-
Extracutaneous manifestation may occur
-
Itraconazole is the drug of choice
-
Saturated solution K iodide, is much less costly and still recommended as an alternative treatment
Protozoa
Giardia lamblia (Giardiasis)
Background
-
Giardiasis is an infection of the small intestine caused by the flagellated protozoan Giardia intestinalis .
-
Mode of transmission
-
Travelers and hikers who drink water contaminated with stool from infected animals such as beavers, muskrats, and sheep.
-
Outbreaks also may occur from sewage contamination of water supplies.
-
Unprotected anal sex also is a source of transmission.
-
Child care centers from fecal-oral transmission.
-
Food-associated outbreaks may occur.
-
Clinical presentation
-
Most infections remaining asymptomatic
-
Watery diarrhea with abdominal cramping
-
Nausea
-
Vomiting
-
Weight loss
-
Flatulence
Diagnosed
-
Microscopic examination of the stool for cysts or by antigen detection
Treatment
-
Indicated for all symptomatic patients.
-
Metronidazole, a single dose of tinidazole, or nitazoxanide for 3 days.
-
Immunocompromised patients, e.g., AIDS at increased risk for chronic giardiasis and treatment failure.
Entamoeba histolytica
Background
-
Amebiasis is caused by pathogenic species of Entamoeba
-
Mode of transmission
-
Fecal-oral route
-
Travel to high-risk area, e.g., Mexico
-
Clinical presentation
-
Can be asymptomatic
-
Amebic dysentery or colitis
-
Bloody diarrhea with mucus
-
Tenesmus
-
-
Hepatic abscess
-
Fever
-
Abdominal pain
-
Tender enlarged liver
-
Elevated liver enzymes
-
Elevated ESR
-
Diagnosis
-
Stool microscopic examination
-
Stool antigen
-
Serum antibody
-
Ultrasound if liver abscess is suspected
Treatment
-
Symptomatic cases.
-
Metronidazole followed by paromomycin or iodoquinol to eradicate colonization.
-
-
Asymptomatic amebiasis in non endemic areas should be treated with a luminal agent (iodoquinol, paromomycin, or diloxanide furoate) to eradicate infection.
-
Amebic liver abscess can be cured without drainage and even by 1 dose of metronidazole.
Cryptosporidiosis
Background
-
Cryptosporidiosis, caused by Cryptosporidium protozoa
-
Transmitted via feco-oral route; child care centers, and swimming pools
Clinical presentation
-
Diarrhea
-
Chronic diarrhea in immunodeficient patients
Treatment
-
Many immunocompetent patients who have cryptosporidiosis have self-limited disease and do not require therapy
-
A 3-day course of nitazoxanide:
-
To reduce the duration and transmission of diarrhea in children older than 1 year of age
-
No swimming pool for at least 2 weeks after the diarrhea stopped
Toxoplasma gondii (Toxoplasmosis)
Background
-
Obligate intracellular protozoa
-
Mode of transmission
-
Ingestion of contaminated raw or uncooked meat
-
Cats excreta
-
Organ transplants
-
Transplacental to fetus causes congenital toxoplasmosis (see chapter Fetus and Newborns)
-
Clinical presentation
-
Most cases are asymptomatic
-
Fever
-
Malaise
-
Rash
-
Myalgia
-
Cervical lymphadenopathy (most common sign)
-
Brain abscess (test for HIV)
-
Chorioretinitis usually present years later (mostly congenital)
Diagnosis
-
Head CT: ring-enhanced lesion
-
Toxoplasma IgM antibodies
-
PCR
Treatment
-
Pyrimethamine plus sulfadiazine and folic acid
-
Lifelong therapy in HIV patients
Pneumocystis jiroveci (Carinii)
Background
-
Unicellular fungi that do not respond to antifungal treatment
-
Mode of transmission is unknown
-
Commonly seen in immunocompromised patients, e.g., HIV patients
Clinical presentation
-
Subacute diffuse pneumonitis
-
Dyspnea
-
Tachycardia
-
Oxygen desaturation
-
Nonproductive cough
-
Fever
Diagnosis
-
Chest radiography
-
Bilateral diffuse interstitial disease
-
-
Low CD4
-
Bronchoalveolar lavage
-
Lung biopsy
Treatment
-
TMP-SMX
-
IV pentamidine in severe cases
-
Prophylaxis in immunocompromised patients
-
TMP-SMX
-
Plasmodium (Malaria)
Background
-
Intracellular protozoa
-
Transmitted by mosquito bites in endemic area, e.g., south Africa
Plasmodium falciparum
-
Most severe
-
Symptoms develop within a month from returning from endemic area
-
Most common cause of congenital malaria
-
Complications
-
Cerebral malaria
-
Pulmonary edema
-
Severe anemia
-
Renal failure
-
Shock
-
-
Treatment
-
Chloroquine sensitive
-
◦ Chloroquine
-
-
Chloroquine resistant:
-
◦ Quinine plus doxycycline or clindamycin
-
◦ Or atovaquone-proguanil
-
◦ Or mefloquine
-
-
Severe cases
-
◦ Quinidine gluconate IV plus doxycycline or clindamycin
-
-
-
Plasmodium malariae, P. vivax, and P. ovale
-
Periodicity of symptoms
-
Nephrotic syndrome-P. malariae (most benign form)
-
Hypersplenism and splenic rupture-P. vivax and P. ovale
-
Treatment
-
◦ Chloroquine plus primaquine for P. vivax, and P. ovale
-
◦ Chloroquine phosphate for P. malaria
-
-
Clinical presentation of malaria
-
History of travelling to endemic areas in the past years
-
Paroxysmal fever, sweat and rigors
-
Pallor and jaundice
-
Headache and myalgia
-
Abdominal pain
-
Vomiting and diarrhea
-
In severe cases
-
Change in mental status
-
Hepatosplenomegaly
-
Anemia
-
Thrombocytopenia
-
Hypotension
-
Hypoglycemia
-
Hyperkalemia
-
Respiratory distress
-
Diagnosis
-
RBCs smear
Prevention
-
Travelling to chloroquine resistant areas, e.g., South Africa
-
Atovaquone-proguanil 2 weeks before and 4 weeks after or
-
Doxycycline (> 8 years old)
-
Mefloquine (safe for pregnant)
-
-
Travelling to chloroquine sensitive areas, e.g., South America
-
Chloroquine 2 weeks before and 4 weeks after or
-
Atovaquone-proguanil or
-
Mefloquine
-
Helminthic Organisms
Enterobius vermicularis (Pinworm)
Mode of transmission
-
From one person to another via feco-oral route
-
Eggs survive up to 3 weeks and are ingested from finger nails, bedding, and toys
-
Autoinfection
Clinical presentation
-
Anal and vulvar itching (more at night)
-
Enuresis
Diagnosis
-
Visualizing the adult worm at night on the perineum
-
Transparent tape collected over three consecutive mornings under microscope low power
Treatment
-
Albendazole
Ascaris lumbricoides (Ascariasis)
Mode of transmission
-
Ingestion of eggs from contaminated soil (feco-oral)
Clinical presentation
-
Most patient are asymptomatic
-
Nonspecific abdominal pain or discomfort
-
Intestinal obstruction (large number of worms)
-
Due to larvae migration to the liver and lung:
-
Obstructive jaundice
-
Peritonitis
-
Cough (Loeffler’s syndrome)
-
Diagnosis
-
Seeing the ova on microscopic stool examination
-
Seeing the adult worm itself
Treatment
-
Albendazole or pyrantel pamoate
Necator americanus (Hookworm) or Ancylostoma duodenale
Background
-
Found in rural, tropical and subtropical locales
-
Mode of transmission
-
Skin penetration of larvae from soil contaminated by human feces
-
Can cause itchiness and burning sensation
-
-
May be ingested as well
-
Can cause pharyngitis and gastroenteritis
-
-
Clinical presentation (blood sucker worm from the intestine)
-
Failure to thrive
-
Short stature
-
Anemia due to chronic blood loss
Diagnosis
-
Finding the eggs stool (may take 5–10 weeks after infection)
Treatment
-
Albendazole
Trichuriasis (Whipworms)
-
It is due to infection of large intestine with Trichuris trichiura.
-
More common in the Southern USA.
-
Transmitted to human by ingesting eggs.
-
Usually asymptomatic if only few worms.
-
Can cause fever, abdominal pain, weight loss, blood in stool and rectal prolapse.
-
Presence of eggs in stool is diagnostic.
-
Treatment is mebendazole.
Trichinosis (Trichinella spiralis)
-
Trichinella spiralis is usually found in pork.
-
Symptoms depend on the worm location.
-
After ingestion the eggs hatch, larvae invade the duodenum, and causes abdominal symptoms.
-
Larvae penetrate, reach bloodstream, end in muscular tissue and causes muscle pain.
-
If the larvae reach the heart can cause myocarditis.
-
Ocular involvement; presence of chemosis, periorbital edema, and eosinophilia usually suggest the diagnosis.
-
Diagnosis is confirmed by rising titers.
Strongyloides stercoralis
-
S. stercoralis is common in certain areas of the USA.
-
In the USA this infection is common in Kentucky and Tennessee.
-
It is the only helminthic organism replicates in the body with autoinfection, and the infection may persist for decades.
-
Can cause pulmonary symptoms with eosinophilia and GI symptoms as well.
-
It is potentially fetal in immunosuppressed patients.
-
Diagnosis of serial stool studies for larvae not the eggs.
-
Treatment is ivermectin or thiabendazole.
Toxocariasis
-
Toxocara canis and Toxocara catis can cause visceral larva migrans.
-
It is transmitted to human by ingesting soil contaminated with dog or cat excreta.
-
In human larva do not develop into adult worms but rather migrate through the host tissue; causing eosinophilia.
-
Treatment is albendazole or mebendazole.
Cestodes (Platyhelminthes)
-
Platyhelminthes include cestodes (tapeworms) and trematodes (flukes).
-
Cestodes are flatworms (tapeworms).The pork tapeworm. Taenia solium, present in two different ways.
-
If the cysticerci are ingested, taeniasis develops and tape worm grows in the intestine.
-
If contaminated food with eggs is ingested, the patient will develop cysticercosis.
-
Cysticerci go in CNS and the eyes and do nothing until they die.
-
Diagnosis of neurocysticercosis must be considered in the patients with new onset seizures and history of travelling to or immigration from Mexico, Central or South America or who is a household from these areas.
Trematodes (Platyhelminthes)
-
Trematodes or flukes.
-
Clonorchis sinensis is the Chinese liver fluke.
-
Schistosoma haematobium infects the bladder and cause urinary symptoms.
-
Schistosoma mansoni is a fluke found in Africa, the Middle East, and South America.
-
Schistosoma japonicum is found in Asia.
-
Most serious complications of Schistosomiasis is cirrhosis with esophageal varices.
-
Treatment is praziquantel
Fever Without Focus
Febrile Neonate
Background
-
It is difficult to distinguish between a serious bacterial infection and self limited viral illness in this age group.
-
Neonates who have fever and do not appear ill have a 7 % risk of having a serious bacterial infection.
-
Serious bacterial infections include occult bacteremia, meningitis, pneumonia , osteomyelitis, septic arthritis, enteritis, and UTI .
-
Late onset neonatal bacterial diseases, e.g., group B Streptococci, E. coli, and Listeria monocytogenes and perinatal herpes (HSV) infection.
-
If the neonate has fever recorded at home by reliable parents, the patient should be treated as febrile neonate.
-
If excessive clothing and blanket falsely elevating the temperature, the excessive covering should be removed and retake the temperature in 15–30 min.
Management
-
All febrile neonates must be hospitalized.
-
Full sepsis evaluation including blood, urine, CSF should be cultured.
-
Child should receive empirical antibiotics such as cefotaxime and ampicillin.
-
Acyclovir should be included if HSV infection is suspected.
-
CSF studies should include cell count, glucose, and protein level, Gram stain, cultures; HSV, and enterovirus PCR should be considered.
-
Stool culture and CXR may be included.
Fever in 1–3 Months Infants
Background
-
Large majority of the children with fever without localizing signs in 1–3 months age group likely viral syndrome.
-
Most viral diseases has distinct seasonal pattern unlike bacteria, e.g., respiratory syncytial virus, and influenza more common during winter and enterovirus infection more common during summer and fall.
Management
-
Ill appearing (toxic) febrile infants ≤ 3 months:
-
Require prompt hospitalization, immediate parenteral antibiotics after blood and CSF cultures are obtained.
-
-
Well appearing infants 1–3 months who is previously healthy with no evidence of focus of infection:
-
WBCs count of 5000–15,000 cells/µL, an absolute band count of ≤ 1500 cells/µL, and normal urinalysis, and negative culture (blood and urine) results are unlikely to have a serious bacterial infection.
-
-
The decision to obtain CSF studies in the well appearing 1–3 months old infant depends on the decision to administer empirical antibiotics.
-
If close observation without antibiotics planned, a lumbar puncture may be deferred.
Fever in 3–36 Months of Age
Background
-
Approximately 30 % of febrile children in the 3–36 months age group have no localizing signs of infection.
-
Viral infections are the cause of the vast majority of fevers in this population.
-
Risk factors indicating probability of occult bacteremia
-
Temperature ≥ 39 °C, WBC count ≥ 15,000/µL, elevated absolute neutrophil count, bands, ESR and CRP.
-
The risk of bacteremia and/or pneumonia or pyelonephritis, among infants 3–36 months of age increases as temperature (specially > 40 °C) and WBCs count (specially > 25,000) increases.
Management
-
Toxic appearing febrile children 3–36 months of age who do not have focal infection should be hospitalized, and prompt institution of parenteral antibiotics after blood, urine and CSF cultures are obtained (full sepsis evaluation).
-
For nontoxic appearing infants who have temperature < 39 °C can be observed as outpatient with no diagnostic test or antibiotics.
-
For nontoxic infants who have rectal temperature ≥ 39 °C, options include obtaining obtaining a blood culture, and administering empirical antibiotic therapy (ceftriaxone, a single dose 50 mg/kg not to exceed 1 g) or blood culture with no antibiotic and observing the patient within 24 h as out-patient. (Careful observation without empirical antibiotics is generally prudent).
Fever of Unknown Origin (FUO)
Background
-
FUO was defined as:
-
More than 3 weeks’ duration of illness. Temperature greater than 38.3 °C (101 °F) on several occasions.
-
Failure to reach a diagnosis despite 1 week of inpatient investigation.
-
-
Patients with undiagnosed FUO (5–15 % of cases) generally have a benign long-term course, especially when the fever is not accompanied by substantial weight loss or other signs of a serious underlying disease.
-
FUO last more 6 months in uncommon in children and suggests granulomatous or autoimmune disease (Table 4).
Approach
-
Age of the patient is helpful:
-
Children > 6 years of age often have respiratory or genitourinary tract infection, localized infection (abscess, osteomyelitis), JIA, or rarely leukemia.
-
Adolescent patients more likely to have TB, inflammatory bowel disease , autoimmune process or lymphoma in addition to the causes of FUO in younger children.
-
-
Exposure to wild or domestic animals, and zoonotic infection.
-
History of pica should be elicited; ingestion of dirt is a particularly important due to infection with Toxocara canis or Toxoplasma gondii.
-
Physical examination is essential to find any physical clues to underlying diagnosis, e.g., lymphadenopathy, rash, joint swelling, etc.
-
Laboratory it is determined on case-by-case bases.
-
ESR > 30 mm/h indicates inflammation and need further evaluation.
-
ESR > 100 mm/h suggests tuberculosis, Kawasaki disease, malignancy or autoimmune disease.
-
Low ESR does not eliminate the possibility of infection.
-
CRP is another acute phase reactant that is elevated and returns to normal more rapidly than ESR.
-
Cultures, serologic studies, imaging studies and biopsies depending on each case.
Treatment
-
The ultimate treatment of FUO is tailored to the underlying diagnosis.
-
Empirical trials of antimicrobial agents may be dangerous and obscure the diagnosis of infective endocarditis, meningitis, parameningeal infection, and osteomyelitis.
-
Antipyretics for fever and relief of symptoms.
Central Nervous System (CNS) Infections
Encephalitis
Definition
-
Inflammation of the brain
Causes
-
Viral, e.g., West Nile virus and herpesvirus (most common)
-
Bacteria, e.g., Mycoplasma, tertiary syphilis
-
Noninfectious, e.g., autoimmune
-
Prion protein
-
Parasitic
-
Fungal
-
Acute cerebellar ataxia
-
Ataxia
-
Nystagmus
-
Cerebellar dysarthria
-
Epidemiology
-
WNV remains the most commonly encountered arboviral encephalitis agent.
-
California encephalitis viruses have the greatest proportion of pediatric symptomatic infections (88 % of cases).
-
Eastern equine encephalitis has the highest overall mortality rate of 42 %.
-
The importance of local epidemiological information and seasonality cannot be ignored.
-
Enteroviruses are most often seen in spring and summer.
-
Arthropod-borne illnesses, in the summer and fall.
Clinical presentation
-
Altered mental status
-
Seizures
-
Weakness
-
Sensory disturbances
-
Nonepileptic movement disorders
-
Young children in absence of identifiable cause may present with:
-
Somnolence
-
Disinterest in feeding
-
Weak suck and irritability
-
Loss of head control
-
Abnormal eye movements
Further clinical clues:
-
Fever (either acutely or in the 1–4 week interval before the onset of symptoms)
-
Meningeal irritation
-
Any child presenting with uncharacteristic behavior that is persistent and disproportionate to environmental and situational factors
-
Initial evaluation of the patient include:
-
Seasonal presentation.
-
History of immunosuppression.
-
Travel history.
-
Recent local epidemiological information.
-
Presence of focal neurologic symptoms or deficits.
Investigation
-
Complete blood count.
-
Complete metabolic panel.
-
Urinalysis.
-
MRI or CT scan for intracranial pressure.
-
EEG.
-
Enteroviral infections can produce a sepsis-like syndrome with more remarkable hematologic abnormalities.
-
Neonatal HSV infections sometimes produce hepatic function abnormalities and disseminated intravascular coagulation.
-
SIADH.
-
Lumbar puncture if normal pressure.
-
Cerebrospinal spinal fluid study:
-
The lumbar puncture is the single most utilized test for the diagnosis of encephalitis .
-
Increased opening pressure.
-
Normal or elevated protein concentration.
-
Normal glucose level.
-
Pleocytosis, polymorphonuclear leukocytes and then converts to lymphocytic in many viral cases.
-
Monocytic, predominance may show with progression of the disease.
-
Hemorrhagic pleocytosis with HSV.
-
Atypical lymphocytes with EBV.
-
Mononuclear leukocytes with echovirus or varicella-zoster infection.
-
PCR amplification of viral DNA.
-
Pleocytosis tends to be less dramatic in parainfectious encephalitis or acute cerebellar ataxia.
-
Fourfold rise in titer, especially immunoglobulin M, against a suspected agent is most often considered diagnostic.
-
-
Intravenous acyclovir while waiting for lumbar puncture, or while waiting for laboratory results, including HSV PCR.
-
Intracranial hypertension conservative measures
-
Head elevation
-
Hyperventilation
-
Fluid restriction
-
Mannitol is used on a limited basis
-
Treatment of seizure
-
Benzodiazepines (midazolam, lorazepam, diazepam) in the beginning followed by loading dose of fosphenytoin, or Phenobarbital.
Meningitis
Neonatal Streptococcal Meningitis
-
GBS remains the predominant neonatal meningitis pathogen .
-
Early-onset disease, infants typically manifest with signs suggestive of sepsis, often with pneumonia, but less commonly with meningitis.
-
Late-onset disease; the typical infant who has late-onset disease is 3–4 weeks of age and presents with meningitis or bacteremia.
Neonatal Gram-negative Meningitis
-
Gram-negative bacillary meningitis is rare and E. coli being the most commonly isolated pathogen.
-
Other gram-negative neonatal meningitis pathogens such as Citrobacter koseri, Enterobacter sakazakii, and Serratia marcescens.
Neonatal Herpes Simplex (HSV) Infection
-
HSV in the newborn can present as isolated skin or mucous membrane lesions, encephalitis, or a disseminated process.
-
HSV infection occurs most commonly in infants born to mothers who have active primary infection.
-
Frequently no maternal history or clinical evidence is available to alert the practitioner to this diagnosis.
-
The incubation period is 2 days to 2 weeks, and most infants who develop HSV CNS infection are 2–3 weeks of age .
Neonatal Listeria meningitis
-
Common sources:
-
Unpasteurized milk
-
Soft cheeses
-
Prepared ready-to-eat meats
-
Undercooked poultry
-
Unwashed raw vegetables
-
-
Can precipitate abortion and preterm delivery.
-
Septic appearance in the neonate is typical in cases of early onset.
-
Papular truncal rash has been identified.
S. pneumoniae
-
Pneumococcus is the leading pathogen causing bacterial meningitis in infants and young children in developed countries.
N. meningitidis
-
Meningococcal disease generally occurs in otherwise healthy individuals and often has a fulminant presentation with high fatality rates.
Aseptic meningitis
-
Enteroviruses virus infection is the most common .
-
B. burgdorferi in mid-Atlantic states.
-
Vasculitis in the setting of systemic lupus erythematosus or Kawasaki disease.
-
Drug-induced such as ibuprofen, and IV immunoglobulin
Other Causes of Meningitis
-
M. tuberculosis
-
B. burgdorferi
-
Rickettsia rickettsii
Clinical Manifestations of Meningitis
-
Infants younger than 1 month of age who have viral or bacterial meningitis
-
Fever
-
Hypothermia
-
Lethargy
-
Irritability
-
Poor feeding
-
-
Signs and symptoms of increased intracranial pressure and meningeal inflammation
-
Vomiting
-
Apnea
-
Seizures also can occur
-
-
Older children and adolescents often experience
-
Malaise
-
Myalgia
-
Headache
-
Photophobia
-
Neck stiffness
-
Anorexia
-
Nausea.
-
Physical Examination
-
Altered levels of consciousness can present as irritability, somnolence, lethargy, or coma
-
Intracranial pressure include:
-
Papilledema.
-
Diplopia.
-
Unilateral or bilateral dilated pupil.
-
Poorly reactive pupils.
-
Bulging fontanelle in infants.
-
Head circumference always should be obtained, especially in those who have an open fontanelle.
-
Meningismus is suggestive of meningeal irritation.
-
Kernig sign:
-
The patient lies supine and the thigh is flexed at a right angle to the trunk. If knee extension from this position elicits pain, the Kernig sign is positive.
-
-
Brudzinski sign:
-
The patient lies supine and flexes his or her neck.
-
A positive sign occurs if the patient also reflexively flexes the lower extremities, typically at the knees.
-
-
Absence of Kernig and Brudzinski signs does not exclude meningitis.
-
Exanthems typical for enterovirus, borreliosis (erythema migrans), and invasive meningococcal or pneumococcal disease (petechiae and purpura) may be present.
Diagnosis
-
All children who are suspected of having meningitis should have their CSF examined unless lumbar puncture is contraindicated.
-
Contraindications of lumbar puncture include:
-
Focal neurologic deficits.
-
Signs of increased intracranial pressure.
-
Uncorrected coagulopathy.
-
Cardiopulmonary compromise.
-
-
Computed tomography (CT) scan is performed before lumbar puncture if any signs of ICP.
-
CSF finding of Bacterial meningitis (Table 5).
-
Glucose concentration usually is less than one half of the measured serum value.
-
Protein value often is greater than 1.0 g/dL (10 g/L).
-
WBC often greater than 1.0 × 103/mcL (1.0 × 109/L), with a predominance of polymorphonuclear leukocytes.
-
Gram stain is extremely helpful if positive.
-
CSF culture remains the gold standard for diagnosing bacterial meningitis.
-
-
CSF finding viral meningitis
-
WBC count of 0.05–0.5 × 103/mcL (0.05–0.5 × 109/L).
-
Neutrophil predominance is common early in the course of infection, shifting to lymphocytic predominance quickly during the illness.
-
Glucose and protein concentrations frequently are normal, although the protein value can be slightly elevated. Gram stain is universally negative.
-
In cases of enteroviral meningitis, enteroviral PCR can confirm the diagnosis.
-
-
Tuberculous meningitis, epidemiologic clue, high protein and lymphocytosis.
-
SIADH and hyponatremia commonly occur in bacterial meningitis.
-
Leukopenia, thrombocytopenia, and coagulopathy may be present in meningococcal and rickettsial infection.
Management
-
Therapy should not be delayed if CNS infection is suspected.
-
Appropriate antimicrobials are required in bacterial meningitis, HSV encephalitis, Lyme meningitis, tuberculous meningitis, and rickettsial infection, and in all cases, timely diagnosis and correct antimicrobial choice are critical.
-
If the practitioner cannot perform a lumbar puncture or there are contraindications to CSF examination, a blood culture should be obtained and antibiotics administered promptly.
Drug choice and duration
-
For infants
-
Ampicillin (300 mg/kg/day divided every 6 h) and cefotaxime (200–300 mg/kg/day divided every 6 h) is appropriate.
-
Acyclovir (60 mg/kg/day divided every 8 h) should be added if HSV infection is a concern.
-
Vancomycin (60 mg/kg/day given every 6 h) should be added, if the Gram stain suggests pneumococcus.
-
-
Children older than 2 months of age
-
Vancomycin (60 mg/kg/day divided every 6 h) plus ceftriaxone (100 mg/kg/day given in one dose or divided into two doses) or cefotaxime (200–300 mg/kg/day divided every 6 h) should be used for empiric coverage.
-
Once culture and susceptibility data are available, definitive therapy can be selected.
-
-
HSV meningitis
-
Neonatal HSV CNS infection typically is treated with IV acyclovir (60 mg/kg/day divided every 8 h) for 21 days.
-
The dosing for non-neonates is 30 mg/kg/day divided every 8 h IV for 14–21 days.
-
Follow-up CSF HSV DNA PCR should be evaluated at day 21 and the course of therapy extended if the result still is positive.
-
Corticosteroids in bacterial meningitis
-
Adjunctive treatment has reduced rates of mortality, severe hearing loss, and neurologic sequelae significantly in adults who have community-acquired bacterial meningitis.
-
For children beyond the neonatal age groups, available data suggest that the use of adjunctive corticosteroids may be beneficial for Hib meningitis and could be considered in cases of pneumococcal meningitis.
-
The dose of dexamethasone for bacterial meningitis is 0.6 mg/kg/day divided into four doses and administered IV for 4 days. The first dose should be given before or concurrently with antibiotics.
Care of the child exposed to meningitis
-
Meningococcal and Hib disease create an increased risk for secondary infection in contacts.
-
Rifampin generally is the drug of choice for chemoprophylaxis in children.
Prognosis
-
Intellectual deficits (intelligence quotient < 70), hydrocephalus, spasticity, blindness, and severe hearing loss are the most common sequelae.
-
Hearing loss occurs in approximately 30 % of patients, can be unilateral or bilateral, and is more common in pneumococcal than meningococcal meningitis.
Brain Abscess
Causes of brain abscess
-
Chronic otitis media
-
Paranasal sinus infection
-
Mastoiditis
-
Head injury
-
S. aureus
-
Metastatic spread, e.g., endocarditis
-
Right-to-left cardiac or pulmonary shunts, especially in the presence of cyanotic congenital heart disease
Clinical presentation
-
Headache (most common)
-
May be throbbing
-
Worsen with changes in posture or Valsalva maneuver
-
-
Drowsiness
-
Confusion
-
Vomiting
-
Drowsiness, and coma
-
Hemiparesis
-
Papilledema
Frontal lobe abscesses
-
Apathy, memory deficits
-
Personality change
-
Mental slowing
Cerebellar abscesses
-
Nystagmus
-
Defective conjugate eye movements to that side
-
Ataxia
-
Hypotonia
Laboratory diagnosis
-
Little in the laboratory investigation of patients who have brain abscesses is specific to the diagnosis except for culture of the purulent material and antibiotic sensitivity of the responsible organism.
Neuroimaging
-
CT scan of the brain
-
Ill-defined
-
Low-density change within the parenchyma
-
Enhancement occurs following administration of contrast material
-
Classic ring-enhancing lesion with surrounding edema
-
Calcification is common in abscesses in neonates
-
-
Magnetic resonance imaging (MRI)
Antimicrobial therapy
-
For abscesses arising as a result of sinusitis in which streptococci are the most likely organisms, penicillin or cefotaxime and metronidazole.
-
Chronic otitis media or mastoiditis often is associated with P. aeruginosa and Enterobacteriaceae, antibiotics to treat abscesses secondary to these infections should include penicillin, metronidazole, and a third-generation cephalosporin.
-
Metastatic abscesses require a regimen based on the likely site of primary infection.
-
S. aureus commonly is isolated in abscess following trauma.
Surgical intervention
-
Provide a specimen of purulent material for bacteriologic analysis and antibiotic sensitivity testing.
-
Remove purulent material, thereby lowering intracranial pressure and decreasing the mass effect of the abscess.
-
Decompress and irrigate the ventricular system and debride the abscess in the event of its rupture into the ventricular system .
Suggested Readings
American Academy of Pediatrics, American Public Health Association, and National Resource Center for Health and Safety in Child Care and Early Education. Caring for our children: national health and safety performance standards: guidelines for out-of-home child care programs. 2nd ed. Elk Grove Village, Ill: American Academy of Pediatrics and Washington, DC: American Public Health Association; 2002.
Coats DK, Demmler GJ, Paysse EA, Du LT, Libby C. Ophthalmologic findings in children with congenital cytomegalovirus infection. J AAPOS. 2000;4:110–6.
Fatahzadeh M, Schwartz RA. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57:737–63.
American Academy of Pediatrics. Cytomegalovirus infection: Varicella-zoster infections. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2009 report of the committee on infectious diseases. 28th ed. Elk Grove Village: American Academy of Pediatrics; 2009. p. 714–27.
Committee on Pediatric AIDS. HIV testing and prophylaxis to prevent mother-to-child transmission in the United States. Pediatrics. 2008;122:1127–34.
American Academy of Pediatrics. HIV. In: Pickering LK, Baker CJ, Long SS, McMillan JA, editors. Red Book: 2006 Report of the Committee on Infectious Diseases. 27th ed. Elk Grove Village: American Academy of Pediatrics; 2006. p. 401–11.
Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118:1774–92.
American Academy of Pediatrics. Cat-scratch disease. In: Pickering LK, Baker CJ, Long SS, McMillan JA, editors. Red Book: 2006 report of the committee on infectious diseases. 27th ed. Elk Grove Village: AAP; 2006. p. 246–8.
American Academy of Pediatrics. Chlamydial infections. In: Pickering LK, Baker CJ, Long SS, editors. Red Book: 2006 report of the committee on infectious diseases. 27th ed. Elk Grove Village: American Academy of Pediatrics; 2006. p. 249–57.
American Academy of Pediatrics. Gonococcal infections. In: Pickering LK, Baker CJ, Long SS, McMillan JA, editors. Red Book: 2006 report of the committee on infectious diseases. 27th ed. Elk Grove Village: American Academy of Pediatrics; 2006. p. 301–9.
American Academy of Pediatrics. Tuberculosis. In: Pickering LJ, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2009 report of the committee on infectious diseases. 28th ed. Elk Grove Village: American Academy of Pediatrics; 2009. p. 680–701.
Duong M, Markwell S, Peter J, Barenkamp S. Randomized, controlled trial of antibiotics in the management of community-acquired skin abscesses in the pediatric patient. Ann Emerg Med. 2010;55:401–7.
American Academy of Pediatrics. Group A streptococcal infections. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2009 report of the committee on infectious diseases. 28th ed. Elk Grove Village: American Academy of Pediatrics; 2009. p. 616–28.
Amren DP, Anderson AS, Wannamaker LW. Perianal cellulitis associated with group A streptococci. Am J Dis Child. 1966;112:546–52.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Naga, O., Hakim, M. (2015). Infectious Diseases. In: Naga, O. (eds) Pediatric Board Study Guide. Springer, Cham. https://doi.org/10.1007/978-3-319-10115-6_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-10115-6_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-10114-9
Online ISBN: 978-3-319-10115-6
eBook Packages: MedicineMedicine (R0)