
Abstract
Leprosy, also known as Hansen’s disease, is an ancient chronic infectious disease that remains a major problem in the world today, infecting over 200,000 people each year, particularly affecting resource-limited and the most disadvantaged sections of society in under-developed countries of the world. Mycobacterium leprae, a slow-growing mycobacterium, causes leprosy in humans. Leprosy causes nerve damage and permanent disabilities including blindness and paralysis. People affected by leprosy face stigma and discrimination in society. Although multidrug therapy is available, millions of people are still affected by leprosy, so new vaccine, drug and disease management approaches are urgently needed for control, prevention and treatment of this disease. This chapter is a general review of leprosy, the current treatment and prevention measures and challenges that need to be addressed for complete eradication of this disease.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Leprosy, also known as Hansen’s disease, is an ancient chronic human infectious disease that remains a major public health problem in many developing countries. Leprosy is caused by the pathogen Mycobacterium leprae, first discovered over a century ago by the Norwegian scientist Gerhard-Henrik Armauer Hansen. M. leprae is a slow-growing mycobacterium and an obligate intracellular pathogen, which can survive out of the human host for up to 45 days [1,2,3]. The genome sequence analysis of M. leprae revealed massive gene decay and reductive evolution with functional genes accounting for less than half of the genome and pseudogenes accounting for the remaining more than half of the genome [3]. The genome size of M. leprae is 3.27 megabase which is extremely reduced in comparison to its related pathogen, M. tuberculosis (4.41 megabase) [3]. Gene deletions include those primarily involved in energy metabolism (a curtailed respiratory chain resulting in no ATP formation from NADH oxidation), microaerophilic and anaerobic respiratory chains, catabolism of carbon and nitrogen compounds and regulatory pathways [2,3,4]. The disease incubation period averages over 5 years, and the symptoms may take between 1 and 20 years to occur [5]. Leprosy affects the nerves, skin, respiratory tract, bones, testes and eyes, and can cause permanent deformity and disability if left untreated [6,7,8].
Historically, the first cases of leprosy were described in parts of China, India and Egypt: around third BC in China and around 600 BC in an Indian treaty Sushruta Samhita. There are hypotheses about the origin of this disease in Africa or in Asia and then its spread towards the European and American continents through human migrations [9, 10]. The global number of cases reported between 1960 and 1980 was 10–12 million. The number of cases declined drastically to 5.5 million in 1991 with the approval and use of multidrug therapy (MDT) since 1981. The number of cases further declined to 265,661 in 2006. Between 2006 and 2013, the number of cases was largely stable (215,656 in 2013) with a very slow reduction in case numbers [6]. Over the past 8 years, around 200,000 leprosy cases are being registered every year. According to the World Health Organisation (WHO) (https://www.who.int/news-room/fact-sheets/detail/leprosy), there were 202,256 new leprosy cases registered in 2019. The prevalence of leprosy differs from one region to another. For instance, the highest prevalence of this infection is in South-east Asia accounting for over 70% of the total cases globally as per records in 2013. India, Brazil and Indonesia are three countries with the highest number of new cases annually [11]. Bloke et al. [11] correctly predicted the unlikely elimination of future leprosy incidences in these high-endemic countries by 2020 (WHO’s previous target for global leprosy elimination by 2020) using the current methods for passive and active case detection and current MDT [11]. There are gender and age-related distributions; the proportion of women in the detected cases were lower than men (for instance, 0.5% in Pakistan, 56% in South Sudan); the proportion of children in detected cases were 0.6% in Argentina and Mexico and 39.5% in the Federated States of Micronesia [9]. Gender inequalities in physical appearance and social stigma are some of the reasons for gender-related leprosy distributions [12]. The sociocultural outcomes of the disease have been found to affect women more than men, such as more social and family rejections and restrictions.
2 Disease Transmission and Infection
M. leprae transmission occurs through air droplets and close contact with infected individuals. Lepromatous leprosy patients are usually most contagious due to the large number of bacilli (up to seven billion) in their infected tissues [9]. The main dissemination and entry route for the leprosy bacilli have been found to be the upper respiratory tract, as determined with experimental mouse models [3, 9, 13, 14]. A summary of leprosy transmission routes, infection and symptoms is shown in Fig. 3.1. Identification of leprosy transmission is hindered because clinical manifestations of the infection can usually take up to 10–15 years in the close contacts [15]. People living within leprosy-endemic communities are exposed to M. leprae, but few develop diseases, likely because most of the population develop protective immunity. Ramaprasad et al. [15] demonstrated the subclinical transmission of M. leprae involving transient infection of nose detected by PCR and a consequent mucosal immune response measured by salivary anti-M. leprae IgA (sMLIgA) tests.

Overview of leprosy transmission routes, infection and symptoms. Mycobacterium leprae is the causative agent of leprosy. The symptoms are nodules, lumps, bumps, lesions and patches on the skin, blindness, nerve damage, muscle weakness and paralysis to the hands, arms, legs and feet. The main route is transmission through air droplets from infected individuals and through contact with infected skin and tissues. Transmission can occur through close contact, such as living with a leprosy patient in the same household. The main factors are poverty, inadequate housing and unhygienic conditions, poor diet and contaminated water
The distinct phases in the immunology of leprosy are not completely understood. At the site of infection such as in the nasal mucosa, M. leprae encounters macrophages or dendritic cells as the first contacts in the absence of an adaptive immune response. The bacilli are taken up by these immune cells with concomitant production of cytokines and chemokines and stimulation of cell-mediated Th1 or Th2 immune responses [4]. M. leprae-infected dendritic cells present phenolic glycolipid-1 (PGL-1) antigen on their cell surface with subsequent antibody responses and T cell stimulations. Monocytes and dendritic cells in the tuberculoid lesions express Toll-like receptors (TLRs) that recognize M. leprae antigens and induce Th-1 type cell-mediated immune responses for proinflammatory cytokine production and granuloma formation [4, 16]. In macrophages, the bacilli are challenged with antimicrobial peptides and reactive oxygen and nitrogen species to eliminate the infection. Schwann cells (both myelinated and nonmyelinated) are one of the primary targets of M. leprae infection [4, 17, 18]. M. leprae adheres to the Schwann cell surface through binding of the PGL-1 to laminin-2 of the axon unit, followed by ingestion of the bacilli by the Schwann cells [19]. M. leprae can proliferate in the Schwann cells, and it uses host cell nutrients to synthesize its biomass [2, 18]. Schwann cells are also able to present M. leprae antigens to T cells, which may be responsible for the inflammatory responses and consequent nerve damage [4].
Several genetic factors have been identified to be involved in specific host immune responses to M. leprae and in heterogeneity of the clinical manifestations of the disease [20,21,22,23]. Mi et al. [21] provided a comprehensive review of the cell type-specific immunological and genetic factors associated with various clinical forms of the disease: genes VDR, OPA1, SLC7A2, RAB32, SLC29A3, LRRK2, IRGM, CTSB, DEFB1, PARK2, PACRG and TNF are associated with macrophage-specific immune responses; TLR1, TLR2, NOD2, HLA, MICA and MICB are associated with dendritic cell responses; FLG is associated with keratinocytes; IL23R, IL12B, TNFSF15, TYK2, SOCS1, IL18R1 and LTA are associated with T cells [21]. A genome-wide association analysis identified single nucleotide polymorphisms in C13orf31, LRRK2, NOD2 and RIPK2 genes strongly associated with multibacillary leprosy and that variants of genes in the NOD2-mediated signalling pathway are involved in susceptibility to M. leprae infection [24]. Distinct cytokine expression was found to be associated with the multibacillary and resistant form of the disease. Yamamura et al. [25] demonstrated a predominant expression of interleukin (IL)-4, IL-5 and IL-10 in multibacillary leprosy and the expression of IL-2 and interferon gamma (IFN)-γ in the lesions analysed from 16 patients with lepromatous and tuberculoid leprosy.
M. leprae infection induces host cell metabolic reprogramming. Formation of lipid droplets and accumulation of oxidised phospholipids, cholesterol and fatty acids that results in “foamy cells” is a characteristic of infected cells such as that observed in the infected skin lesions, macrophages and Schwann cells [26]. Foamy cell formation is also a characteristic of the related M. tuberculosis infection [27]. In addition to up-regulation of lipid metabolism genes in infected host cells, a decrease in mitochondrial ATP formation with a concomitant rise in glycolytic activity has been reported. Infected Schwann cells showed increased glucose uptake and pentose phosphate pathway activity during M. leprae infection [17]. These changes in host cell metabolism are linked to innate immune responses during infection. In infected Schwann cells and macrophages, lipid droplet formation regulates the production of Prostaglandin E2 (PGE2) immunomodulator that controls regulatory T cell (Treg) and macrophage bactericidal activity [26]. Inhibition of lipid droplet formation has been shown to down-regulate production of the anti-inflammatory cytokine IL-10 and cause a switch from an anti-inflammatory to a pro-inflammatory phenotype [28, 29]. M. leprae infection induces an elevated expression of indoleamine 2,3-dioxygenase (IDO-1) in macrophages and dendritic cells of lepromatous lesions that increases tryptophan degradation and suppression of innate and adaptive immunity, which in turn decelerates immune signalling to eradicate the infection and supports the survival of M. leprae in the host environment [26, 30]. Accumulation of iron in infected host macrophages has been hypothesised to benefit the survival of M. leprae. The increase in iron metabolism is linked to the non-responsiveness of macrophages to IFN-γ signalling and promotion to an anti-inflammatory M2-like phenotype [26].
3 Disease Classification and Pathophysiology
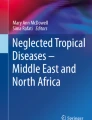
In infected individuals, the bacillus is generally found in the macrophages, keratinocytes and histiocytes of the skin causing dermatological conditions and in the Schwann cells of peripheral nerves causing axonal dysfunction and demyelination [3, 7]. Infection of Schwann cells leads to their de-differentiation and reprogramming, which consequently leads to degeneration and deformation of the peripheral nerves. White et al. [7] reviewed the various clinical manifestations of the disease and provided a summary of the various clinical forms of leprosy and their classifications. The different clinical forms of leprosy are likely due to the genetic and biological variability between infected individuals. According to the WHO, different forms of leprosy are classified based on the symptoms such as the presence of bacilli in the skin smears and visible lesions [7, 8]. Infection is classified as “paucibacillary” with 1–5 skin patches and no apparent bacteria in skin smears. Individuals with more than five skin patches and visible bacteria in the skin smears are classified as “multibacillary” [7]. A study by Pardillo et al. [31] compared the practice of counting lesions to assign treatment regimens in 264 untreated leprosy patients. This study found misclassification, where 38–51% of patients assigned as paucibacillary cases (according to the WHO classification) had multibacillary infection and were therefore at risk of under-treatment and developing drug resistance [31]. The classifications based on the immune responses to infection are tuberculoid (TT), borderline tuberculoid (BT), borderline borderline (BB), borderline lepromatous (BL) and lepromatous (LL), with the last one being the most severe form of the disease, causing extensive nerve damage and physical disability [7, 32, 33] (Fig. 3.2). An alternative WHO classification categorises TT and BT types as paucibacillary and BB, BL and LL as multibacillary [34].

Classification of different forms of leprosy. (a) Tuberculoid (TT) leprosy: this shows a leprosy lesion on the lower back that has healed spontaneously and remains only a thin scar with a complete loss of sensation. (b) Borderline tuberculoid (BT) leprosy: this shows an annular lesion on the cheek of a boy with BT. (c) Borderline borderline (BB): this shows a scarred lesion on the right cheek. (d) Borderline lepromatous (BL) leprosy: this shows a few raised and erythematous lesions on the arm of a patient. (e) Lepromatous leprosy: this leprosy patient has marked loss of the eyebrows and eyelashes and thickening of the facial skin. (The images are from the Wellcome Collection with 4.0 International (CC BY 4.0) licence)
The clinical manifestations of TT are skin lesions (large hypochromic macules, large thickened infiltrated plaques) and nerve damage (usually around skin lesions) and sensory impairment affecting mainly the hands and feet [9]. LL patients present with multiple lepromas on the skin, (most frequently on the face, earlobes, fingers and toes) and peripheral nerve damage with hypertrophy, sensory and motor impairment [9, 35]. BT patients present with several large asymmetrical and hypoaesthetic skin lesions; BB patients present with non-anaesthetic annular lesions, and BL patients present with more than ten bilateral and non-anaesthetic lepromas and annular lesions [9]. The clinical manifestations associated with various forms of leprosy are summarised in Table 3.1. The immunological responses correlated with tuberculoid TT and BT are Th1 cell-mediated responses involving IL-2 and IFN-γ signalling and formation of delineated granulomas to arrest bacterial growth [34]. A Th2 immune response with IL-10 and IL-4 signalling that impedes granuloma formation, allowing bacterial replication and causing infiltration of skin and nerves and severe clinical manifestations, is associated with BL and LL disease types [34, 36].
Reactions or inflammatory responses to M. leprae that occur during the disease or during treatments are the causes of nerve and skin damage. Reactions are categorised into type 1 reactions, type 2 reactions and diffuse lepromatous leprosy [8, 10, 16, 37, 38] (Table 3.2). Type 1 or reversal reactions are associated with BT, BB and BL forms of the disease driven by the cell-mediated immune response to M. leprae [8, 39]. Patients with type 1 reactions suffer pain in lesions, nerve damage such as lagophthalmos, the loss of ability to close the eyelids, inflammatory eye conditions leading to blindness and nerve injury in the feet leading to disability [4, 7, 8]. There is an increase in the levels of proinflammatory cytokines such as tumour necrosis factor (TNF)-α, IL-1, IL-2 and IFN-γ. Type 1 reactions typically occur at the onset or after the completion of MDT treatment. An analysis of patient records from India between 1983 and 1998 revealed widespread disease and multibacillary cases as the main risk factors for Type 1 reactions, with the incidences typically recorded after 6–12 months of MDT [40]. Type 2 reaction, also known as erythema nodosum leprosum (ENL), is a cellular dysfunction characterised by acute fever and acute nerve, eye, lymph node and skin (painful subcutaneous nodules) inflammation and is primarily associated with BL and LL forms of the disease [4, 7, 41]. The levels of C3 immune complexes in serum and its complement activation product C3d in plasma were higher in ENL patients, showing a hyper-catabolism of C3 as a feature of ENL that could be useful for early diagnosis [42]. ENL can occur during different periods of the disease and during MDT treatment, with some patients experiencing Type 2 reactions after being cured. Kumar et al. [40] found the occurrence of ENL reactions during the second or third year of MDT treatment in patients in Chandigarh, India, and identified LL and a bacterial index ≥3 as risk factors for ENL. Interestingly, Kumar et al. [40] identified the female gender as the common risk factor for both Type 1 and ENL reactions. Diffuse lepromatous leprosy is a non-nodular form of lepromatous leprosy characterised by diffuse skin infiltration and soft wrinkles [38, 43]. This clinical form is also termed as “pretty leprosy”. Lucio phenomenon is a thrombotic reaction associated with the diffuse lepromatous leprosy characterised by the presence of nodules and diffuse infiltration and pure diffuse leprosy. Patients with the Lucio phenomenon suffer from fever, anaemia, hepatosplenomegaly, lymphadenopathy and painful irregular lesions [38, 43].
4 Diagnosis and Treatment
Leprosy can be cured with timely diagnosis and MDT treatment [44]. Untreated, it can cause progressive and permanent damage to the skin, nerves, limbs and eyes. According to the WHO, a case of leprosy was identified as hypopigmented or reddish skin lesions, thickening of peripheral nerves and loss of sensation and skin-smear positive for acid fast bacilli. Skin lesions as the dermatological condition are the indicators in 90% of leprosy cases [9]. A clinical review by Moschella et al. [45] discussed the limitations of using only skin lesions as a diagnostic sign. In multibacillary infections presenting with reduced hypopigmentation and reduced lesions, following the diagnostic sign of skin lesions resulted in non-identification of around 30% of leprosy cases. Moschella et al. [45] proposed a combination of diagnostic signs including the presence of thickened nerve and hypopigmented or erythematous skin lesions with and without sensory loss, or impaired nerve function, to improve diagnostic efficacy. Certain leprosy cases can show solely neuronal symptoms without skin lesions termed as neuritic leprosy, and a nerve biopsy is a 100% confirmatory diagnosis for this. Lepromin is a widely used skin antigen test used to measure the ability of an individual to develop a granulomatous response to a mixture of antigens derived from M. leprae from different sources [4, 39]. However, lepromin test is not 100% leprosy-specific, as individuals without any contact with M. leprae can also show a positive lepromin reaction [4]. Skin lesions are used for smear tests and biopsies, which are gold standard laboratory diagnostic tests for leprosy. The smear test is rapid and effective for earlobe smears, but this test is usually negative for paucibacillary and tuberculoid leprosy [9]. Microscopic examination using Ziehl-Neelsen staining for acid-fast bacilli is a standard diagnostic technique for samples such as tissue fluid smears and skin biopsies. Slit-skin smear is a commonly used procedure for assessing acid-fast bacilli in infected skin lesions during and after treatment [4].
Skin biopsies used to detect multibacillary and relapse infections are highly specific with almost 100% diagnostic accuracy, but the sensitivity of this test is around 50%. The reduced sensitivity is caused by the technicalities of the test including sample handling, staining and interpretation [45]. Other diagnostic tests include histological examination, serological anti-PGL-1 antigen, skin, fluorescent leprosy antibody (FLA)-abs and PCR tests. The PGL-1 serological test is highly sensitive and specific for patients with multibacillary disease, but not for paucibacillary cases. This test cannot predict who amongst the close contacts will develop the disease. PCR is a highly sensitive molecular diagnostic test with 100% specificity and sensitivity between 34% and 74% for tuberculoid forms of the disease and 80% in lepromatous diseases [15, 46, 47]. Several gene targets including Pra-36 KDa, Pra-18 KDa, RLEP, Ag85B, 16SRNA, folP, rpoB and gyrA are used [9, 48]. PCR was useful in confirming cases with atypical clinical and histopathological features. However, PCR diagnosis is limited when it comes to detecting paucibacillary cases and cannot distinguish between live and dead bacteria [15]. Clinical diagnosis also includes examination of patient’s medical history, e.g. if they lived in nations with endemic leprosy.
Dapsone, the first drug discovered for treating leprosy in 1941, was a breakthrough for leprosy cure. Clofazimine and rifampicin (discovered later than dapsone) were the other two effective antibiotics for leprosy treatment. MDT was first approved in 1981 by the WHO and consists of these three first-line antibiotics. The recommended duration for MDT treatment for multibacillary (LL, BL and BB disease forms) is 12–24 months and for paucibacillary cases is 6 months. This treatment regime has been proven to produce effective clinical responses and low rates of relapses [9, 38, 49, 50]. Dapsone at a dose of 100 mg daily and rifampicin at 600 mg monthly are prescribed for paucibacillary cases in adults, and clofazimine at 50 mg daily along with dapsone (100 mg daily) and rifampicin (600 mg daily) are prescribed for multibacillary cases [38, 50]. Fluoroquinolones are the second-line antibiotics administered to patients showing intolerance, resistance such as rifampicin-resistant leprosy and clinical failures to first-line antibiotics [9]. A combination of ofloxacin (400 mg/day), minocycline (100 mg/day), clofazimine (50 mg/day) or clarithromycin (500 mg/day) is used to treat rifampicin-resistant cases [38]. Rifampicin- and ofloxacin-resistant cases are treated with a combination of minocycline (100 mg/day), clarithromycin (500 mg/day) and clofazimine (50 mg/day) [38].
Leprosy relapses are also treated with standard MDT [9]. There are geographical variations in the relapse rate of the infection. The risk of relapse is very low for both paucibacillary and multibacillary patients who have completed MDT [51, 52]. The risk of relapses is higher in patients with irregular and inadequate therapy, in patients with failure to respond to therapies and in patients with persistent M. leprae infection and co-infections such as human immunodeficiency virus (HIV). Relapse cases are identified by the reappearance of positive acid-fast bacilli, appearance of active lesions and increase in bacterial index after the patient has been negative [51]. Techniques such as measuring bacterial viability through cultivation of M. leprae in mouse foot pads and through staining microscopy and PCR analysis are used to monitor relapses during treatment. Immunological tests such as anti-PGL1 and anti-35 kD antibodies and PGL-1 serum antigen ELISA are used to monitor treatment and to detect early infection and relapse cases [51]. Cell-mediated immunological response such as Th1 and Th2 levels can aid in identifying the type of relapses, e.g. the relapse of BL/LL patients to TT/BT is associated with an elevated Th1 response (increased IFN-γ and IL-2 cytokines and IgG2 antibodies), while relapse of TT/BT to BL/LL is associated with an elevated Th2 response (increases in IL-4, IL-5, IL-6 and IL-10 cytokines and IgG1 antibodies) [51].
Early detection and treatment of nerve damage are critical to preventing deformity in leprosy patients. Patients should be assessed routinely during and after MDT treatment for peripheral nerve function and damage [50, 53]. Steroids have been used to treat neuropathy in leprosy since the 1970s [53]. Corticosteroids are administered to treat Type 1 and 2 leprosy reactions with a treatment duration of more than 12 weeks [9]. Prednisolone at a dose of 40–60 mg daily is recommended for treating sensory loss and muscle weakness in Type 1 reactions. For treating Type 2 reactions, thalidomide is administered at a dose of 400 mg daily [50, 54, 55]. It is important to monitor the response of patients to steroid treatments, and alternative therapies would be required to overcome the non-responsiveness and any adverse effects. In some cases, intolerance and adverse side effects are observed with corticosteroid treatments. A case study by Biosca et al. [55] investigated the use of methotrexate at a low dose of 5–7.5 mg per week as an alternative to corticosteroid treatment, which had adverse effects (such as insulin-dependent diabetes, hypertension, heart failure, depression, polyphagia, centripetal obesity and facial plethora) on a 58-year-old patient suffering from borderline lepromatous leprosy. Methotrexate improved Type 1 reaction treatment in this patient; skin lesions were reduced, and bacterial index was reduced from 5+ to 1+ [55].
Prevention of leprosy infection requires appropriate monitoring and management of the transmission process and tracing contacts of both symptomatic and asymptomatic individuals. There are several risk factors for close contacts of patients to acquire leprosy such as genetic relationship (children, parents, siblings) and physical distance (living under the same roof and next-door neighbours). A cohort study of 1037 newly diagnosed patients and their 21,870 contacts identified age of the contact and disease classification of the patient as two other factors, in addition to genetic relationship and physical distance associated with the risk of the contact in acquiring leprosy [56]. Contacts with older ages and those that have been in close contact with paucibacillary (2–5 lesions) and multibacillary patients are at a higher risk in acquiring the disease [56]. Moet et al. [56] recommended contact surveys to be extended beyond the household contacts to neighbours and consanguineous relatives of patients with paucibacillary (2–5 lesions) and multibacillary leprosy. There is a need to develop better diagnostic approaches to detect early-stage infection in contacts. MDT alone is insufficient to prevent new cases of leprosy or relapse. Follow-up post-treatment is important to evaluate the efficacy of MDT. According to Smith et al. [44], symptomatic contacts should be given the MDT regimen, and a combination of chemoprophylaxis and rifampicin was recommended for asymptomatic contacts. Rifampicin used at a single dose for contacts in a randomized control trial provided a protective efficacy of ~60% [57]. Administration of immunoprophylaxis with Bacillus Calmette-Guérin (BCG) vaccination along with single dose of rifampicin had a greater protective efficacy of ~80% [57].
5 Challenges and Future Direction
5.1 The WHO Roadmap
According to the current WHO strategy to end leprosy by 2030, the following roadmap and targets are outlined: 120 countries with zero new autochthonous cases; 70% reduction in annual number of new cases detected; 90% reduction in rate per million population of new cases with grade 2 disability; 90% reduction in rate per million children of new child cases with leprosy [5, 58]. To achieve these targets, integrated efforts and national and international partnerships are required. For example, the WHO has listed political commitment for resources, engaging stakeholders; improving healthcare systems, surveillance and data management; and monitoring transmission, treatment and drug reactions, research and innovation for developing vaccines, preventative chemotherapy and management of leprosy reactions, neuritis and disabilities. It is important to develop interventions to monitor and reduce discrimination and stigma associated with leprosy-affected individuals [5, 58].
To improve diagnosis, treatment, management and monitoring of leprosy, a government and public/private sector intervention is required to meet the political, health and financial requirements to tackle the endemic. Interventions such as school surveys and epidemiological mapping can provide an alternative for systematic contact tracing [44, 57]. Leprosy education in schools such as signs and symptoms of the disease could provide a way of increasing social and disease awareness in endemic regions. Screening of school children with the support of healthcare systems could enhance case detection in families and communities [59, 60].
Poverty and socio-economic status are major risk factors for leprosy, and complete elimination of leprosy will require addressing these factors in affected communities [9, 22, 61]. There are multiple social determinants such as undernutrition and poverty in the transmission of leprosy. Poverty and leprosy are linked; disease transmission is higher at an individual level, such as living in a crowded household, and at community level, such as living in an endemic area with high population [36, 49, 62]. People living in poor conditions with inadequate housing, contaminated water, insufficient diet and co-infections or other diseases affecting the immune system are at a high risk of acquiring leprosy [22]. Implementation of poverty reduction programmes such as identification of factors responsible for poverty and inequality will need to be incorporated into public health approaches to eliminate leprosy [36]. Measurement of detection rates provides information about the known prevalence of the disease and helps to implement control measures. Between 2005 and 2007, Penna et al. [63] used spatial span statistics to demonstrate that detection rates varied significantly in the north, north-east and central-west endemic regions of Brazil. The study concluded a time-dependent behaviour of case detection across the three regions, which may be attributed to the ease of access to primary healthcare [63]. Identification of such spatial distribution of leprosy prevalence will help to implement control measures. Chemoprophylaxis and immunoprophylaxis of “contacts” of leprosy patients could be used routinely in referral centres to break any transmission chain [10, 57, 64].
The services for diagnosis, treatment, care, rehabilitation and management for leprosy reactions need to be made easily and equally accessible to patients [10]. The main challenge for under-developed countries is that patients suffer delays in detection, treatment and care. Nerve damage can occur any time before, during or after treatment, and the degree of damage reflects the delay between the onset of symptoms and diagnosis, which can occur over many years [10]. A survey conducted by Raffe et al. [65] amongst patients in Nepal revealed a delay of up to 24 months from detection to receiving drugs such as corticosteroids for treating leprosy reactions. Raffe et al. [65] found inconsistencies in drug availabilities and treatment follow-ups. Research on epidemiology and clinical trials would need to adopt standardized tools, so that the outcomes from various research studies can be compared. Genetic studies on heterogenous populations could identify risk factors for the development of disease and neuropathy across different endemic regions of the world [53]. Identification of biomarkers of the disease would lead to rapid diagnosis and early treatment to prevent nerve damage and deformity [66].
5.2 Stigma and Discrimination
Stigma and discrimination are two major problems faced by leprosy patients. “The biggest disease today is not leprosy or tuberculosis, but rather the feeling of being unwanted” (Mother Teresa). The stigma associated with leprosy is the perception of physical deformity that leads to social discrimination and reduced opportunities [67]. The stigma and disabilities in individuals with leprosy patients lead to many devastating problems such as loss of employment, community rejection and in some cases forced isolation [36]. In endemic nations such as Brazil and India, leprosy-affected individuals are isolated into communities because of the lack of housing and employment opportunities [66, 68,69,70]. There is a need to place laws against discrimination to fight the stigma of leprosy and to adopt measures such as introducing patients with leprosy into the community [36]. A way to remove stigma and change perception is to eliminate the fear and prejudice about deformity through education about the disease in communities. An understanding and knowledge of leprosy will reduce misconceptions around the cause, transmission and treatment of the disease [67]. The effects of stigma and discrimination are greater in women patients than in men [67, 71]. Social awareness, health programmes and future research are needed to identify the factors contributing to gender inequalities and to improve women’s compliance with anti-leprosy therapy [12]. Alves et al. [72] reviewed the importance of having knowledge, information and training about leprosy in education and in healthcare settings to improve patient care. In particular, the involvement of dermatologists in training sessions for healthcare professionals working at different levels and in education such as undergraduate courses is essential to raise awareness about this neglected disease and to remove social stigma and discrimination of affected individuals. The role of dermatologists is important for leprosy patient treatment and care as they can identify and treat deformities and skin lesions and assure patients about the treatment and cure [73]. Programmes that involve training of dermatologists to assess neurological damage, sensory testing, use of monofilaments and physiotherapy has been suggested for improving leprosy treatment and patient care [50]. The current COVID-19 pandemic had adverse effects on other infectious diseases including leprosy in terms of care, disease control, treatment and management. Leprosy patients may suffer from elevated reactions because of COVID-19 infection. In addition, leprosy treatment may interfere with inflammatory responses and make leprosy patients more susceptible to contracting COVID-19 [74].
5.3 Alternative Therapies
These are needed to overcome the limitations of current regimens [44]. There are commonly associated side effects with the current MDT such as haemolytic anaemia, hepatotoxicity, gastrointestinal symptoms, headaches, dizziness, renal failure and pigmentation [38, 53, 75]. New drugs such as ofloxacin and minocycline have reduced adverse effects and have enhanced bactericidal activity in mice and in humans [53]. Multidrug-resistant strains exhibiting resistance to dapsone, rifampicin and in some cases fluoroquinolone have emerged and added to the threat of leprosy. Dapsone resistance in M. leprae is due to a mutation in the dihydropteroate synthase, folP1 gene; rifampicin resistance is due to mutations in the sub-unit B of the RNA polymerase rpoB gene; quinolone resistance is due to mutation in the DNA gyrase gyrA gene [9]. There are adverse effects also with steroid therapy such as bruising, muscle weakness, peripheral neuropathy, teratogenicity, drowsiness, mood disorder and insulin resistance [38].
5.4 Animal and Ex Vivo Models
The inability to culture M. leprae in vitro has limited research on this pathogen [2]. There is no suitable animal model, and disease pathogenesis in mice is different to that in humans, and the use of armadillos is not practical for drug and vaccine testing [10]. There have been some efforts to identify the physiology and metabolism of M. leprae during its intracellular growth in human host cells [2, 18]. Borah et al. [18] used isotopic tracing in a M. leprae-Schwann cell model and demonstrated that M. leprae used host glucose pools to synthesize amino acids during infection. Although the metabolic profile of the pathogen could be predicted in this ex vivo model system, the intracellular metabolic fluxes of the pathogen and the vulnerable metabolic nodes that can be targeted for novel drug development could not be measured.
The inability to culture M. leprae in vitro has also hampered investigations on drug resistance and screening for new drugs. Mouse foot pads have been the only feasible method to measure drug susceptibility of a M. leprae strain [9]. However, using mouse foot pads for M. leprae cultivation is lengthy and technically challenging and is therefore of limited use for studying drug resistance and for compound screening. New antibiotic therapy such as bedaquiline (newly approved for tuberculosis treatment) has shown similar anti-leprosy efficacy as rifampicin in mouse models, but clinical trials on leprosy patients are outstanding.
5.5 Diagnostics
PCR as a diagnostic tool is one of the most reliable and robust techniques. However, PCR primer targets, amplicon sizes and primers need to be standardized across various diagnostic settings and reference centres to achieve comparable epidemiological data across endemic regions of the world. Real-time PCR has been used for diagnostic purposes and holds greater promise for sensitive detection than conventional PCR [64]. However, the equipment and reagents needed for this technique are expensive, and the availability of appropriate laboratory facilities such as storage of RNA at −80 °C for analysis will need to be considered. Recent research efforts have made breakthroughs in developing sensitive and efficient techniques such as nanotechnology-based biosensors and imaging. However, we need to consider the applicability of such tools across various reference centres and laboratories in endemic regions and if they are cost effective.
5.6 M. leprae Vaccine
There is no specific vaccine against M. leprae, and this makes disease prevention a major challenge. There are several bottlenecks for leprosy vaccine research, including our incomplete knowledge about the immunological processes that are responsible for pathogenesis and nerve damage. Identification of M. leprae antigens is required to develop a leprosy-specific vaccine. The available information about the M. leprae genome enables the engineering of antigens that can be expressed in fast-growing bacteria and their follow-on assessment for vaccine development. Young et al. [76] used such a strategy and constructed a M. leprae recombinant DNA library using bacteriophage λgt11 to drive recombinant DNA expression in Escherichia coli. Antigens were isolated from the recombinant DNA library using monoclonal antibodies that recognized the M. leprae epitopes produced in E. coli [76]. In addition to identification of suitable antigens, extensive research will be required to identify the complex immunoregulatory mechanisms to avoid any immune reactions that can elicit nerve injury from exposure to antigens. The currently used preventative strategy that includes using BCG vaccine needs reviewing, and more research is needed to improve the efficacy of this vaccine. Multiple trials have highlighted ambiguities in the efficacy of BCG vaccine to protect against leprosy [1, 75]. For example, a low protection of 20% was reported in Myanmar, and a high protection rate of 80% was reported in Uganda [1].
Vaccine development for leprosy has been severely hampered by the limited research on pathogen biology, mainly due to an inability to cultivate M. leprae in vitro. Recently, Borah et al. [2] provided a mixture of nutrients that could be used a starting point in the formulation of an axenic growth medium for M. leprae. This study used genome-scale modelling to investigate in vitro growth of the pathogen and nutritional requirements through interrogation of RNA-seq data of the pathogen isolated from mouse foot pads [2]. The usefulness of this media is yet to be tested experimentally.
6 Conclusions
Leprosy remains an endemic disease despite the availability of MDT therapy. To eradicate leprosy completely, we need to develop alternative therapies to overcome the problems of drug resistance and drug-associated side effects. New interventions are required to tackle the current limitations in disease diagnosis, treatment, management and care. Acceleration of research focused on the pathogen’s biology, and the nature of the host’s cellular immune response is needed to devise therapeutics such as new vaccines for disease prevention and management.
References
Lockwood DNJ, Suneetha S. Leprosy: too complex a disease for a simple elimination paradigm. Bull World Health Organ. 2005;83(3):230–5.
Borah K, Kearney JL, Banerjee R, Vats P, Wu H, Dahale S, et al. GSMN-ML-a genome scale metabolic network reconstruction of the obligate human pathogen Mycobacterium leprae. PLoS Neg Trop Dis. 2020;14(7):1–20.
Cole ST, Eiglmeier K, Parkhill J, James KD, Thomson NR, Wheeler PR, et al. Massive gene decay in the leprosy bacillus. Nature. 2001;409(6823):1007–11.
Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW, Williams DL. The continuing challenges of leprosy. Clin Microbiol Rev. 2006;19(2):338–81.
World Health Organization. Global leprosy strategy 2021-2030: overview global consultation of NLP managers, partners and affected persons; 2020, p. 26–30.
World Health Organization. Global leprosy update, 2014: need for early case detection. 2014. Weekly epidemiological record; 2015. p. 36.
White C, Franco-Paredes C. Leprosy in the 21st century. Clin Microbiol Rev. 2015;28(1):80–94.
Walker SL, Lockwood DNJ. Leprosy. Clin Dermatol. 2007;25(2):165–72.
Reibel F, Cambau E, Aubry A. Update on the epidemiology, diagnosis, and treatment of leprosy. Med Mal Infect. 2015;45(9):383–93.
Lockwood J, Rodrigues LC, Lockwood DNJ. Leprosy now: epidemiology, progress, challenges, and research gaps. Lancet Infect Dis. 2011;11(6):464–70.
Blok DJ, de Vlas SJ, Richardus JH. Global elimination of leprosy by 2020: are we. Parasit Vectors. 2015;8:548.
Le Grand A. Women and leprosy: a review. Lepr Rev. 1997;68(3):203–11.
Rees RJ, Mcdougall AC. Airborne infection with Mycobacterium leprae in mice. J Med Microbiol. 1977;10(1):63–8.
Lastória JC, de Abreu MAMM. Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects—part 1. An Bras Dermatol. 2014;89(2):205–18.
Ramaprasad P, Fernando A, Madhale S, Rao JR, Edward VK, Samson PD, et al. Transmission and protection in leprosy: indications of the role of mucosal immunity. Lepr Rev. 1997;68(4):301–15.
Walker SL, Lockwood DNJ. The clinical and immunological features of leprosy. Br Med Bull. 2006;77–78:103–21.
Medeiros RCA, de Vasconcelos Girardi KDC, Cardoso FKL, de Siqueira MB, de Toledo Pinto TG, Gomez LS, et al. Subversion of Schwann cell glucose metabolism by Mycobacterium leprae. J Biol Chem. 2016;291(41):21375–87.
Borah K, Girardi KCV, Mendum TA, Lery LMS, Beste DJV, Lara FA, et al. Intracellular Mycobacterium leprae utilizes host glucose as a carbon source in Schwann cells. mBio. 2019;10(6):e02351-19.
Marques MAM, Anto VL, Nio Ã, Sarno EN, Brennan PJ, Pessolani MC. Binding of α2-laminins by pathogenic and non-pathogenic mycobacteria and adherence to Schwann cells. J Med Microbiol. 2001;50(1):23–8.
Fava VM, Dallmann-Sauer M, Schurr E. Genetics of leprosy: today and beyond. Hum Genet. 2020;139(6–7):835–46.
Mi Z, Liu H, Zhang F. Advances in the immunology and genetics of leprosy. Front Immunol. 2020;11:567.
Bhat RM, Prakash C. Leprosy: an overview of pathophysiology. Interdiscip Perspect Infect Dis. 2012;2012:181089.
Misch EA, Berrington WR, Vary JC Jr, Hawn TR. Leprosy, and the human genome. Microbiol Mol Biol Rev. 2010;74(4):589–620.
Zhang F-R, Huang W, Chen S-M, Sun L-D, Liu H, Li Y, et al. Genomewide association study of leprosy. N Engl J Med. 2009;361(27):2609–18.
Yamamura M, Uyemura K, Deans R, Weinberg K, Rea T, Bloom B, et al. Defining protective responses to pathogens: cytokine profiles in leprosy lesions. Science. 1991;254(5029):277–9.
de Macedo CS, Lara FA, Pinheiro RO, Schmitz V, de Berrêdo-Pinho M, Pereira GM, et al. New insights into the pathogenesis of leprosy: contribution of subversion of host cell metabolism to bacterial persistence, disease progression, and transmission. F1000Res. 2020;9:F1000 Faculty Rev-70.
Russell DG, Cardona PJ, Kim MJ, Allain S, Altare F. Foamy macrophages and the progression of the human tuberculosis granuloma. Nat Immunol. 2009;10(9):943–8.
Mattos KA, Lara FA, Oliveira VGC, Rodrigues LS, D’Avila H, Melo RCN, et al. Modulation of lipid droplets by Mycobacterium leprae in Schwann cells: a putative mechanism for host lipid acquisition and bacterial survival in phagosomes. Cell Microbiol. 2011;13(2):259–73.
Mattos KA, D’Avila H, Rodrigues LS, Oliveira VGC, Sarno EN, Atella GC, et al. Lipid droplet formation in leprosy: Toll-like receptor-regulated organelles involved in eicosanoid formation and Mycobacterium leprae pathogenesis. J Leukoc Biol. 2010;87(3):371–84.
de Mattos Barbosa MG, da Silva Prata RB, Andrade PR, Ferreira H, de Andrade Silva BJ, da Paixão de Oliveira JA, et al. Indoleamine 2,3-dioxygenase and iron are required for Mycobacterium leprae survival. Microbes Infect. 2017;19(11):505–14.
Pardillo FEF, Fajardo TT, Abalos RM, Scollard D, Gelber RH. Methods for the classification of leprosy for treatment purposes. Clin Infect Dis. 2007;44(8):1096–9.
Ridley DS, Jopling WH. Classification of leprosy according to immunity. A five-group system. Int J Lepr Other Mycobact Dis. 1966;34(3):255–73.
Talhari C, Talhari S, Penna GO. Clinical aspects of leprosy. Clin Dermatol. 2015;33(1):26–37.
Alter A, Grant A, Abel L, Alcaïs A, Schurr E. Leprosy as a genetic disease. Mamm Genome. 2011;22(1–2):19–31.
Haanpää M, Lockwood DN, Hietaharju A. Neuropathic pain in leprosy. Lepr Rev. 2004;75(1):7–18. PMID: 15072122.
Rinaldi A. The global campaign to eliminate leprosy. PLoS Med. 2005;2(12):e341.
Walker SL, Lockwood DN. Leprosy type 1 (reversal) reactions and their management. Lepr Rev. 2008;79(4):372–86.
Maymone MBC, Venkatesh S, Laughter M, Abdat R, Hugh J, Dacso MM, Rao PN, Stryjewska BM, Dunnick CA, Dellavalle RP. Leprosy: treatment and management of complications. J Am Acad Dermatol. 2020;83(1):17–30.
Sansonetti P, Lagrange PH. The immunology of leprosy: speculations on the leprosy spectrum. Rev Infect Dis. 1981;3(3):422–69.
Kumar B, Dogra S, Kaur I. Epidemiological characteristics of leprosy reactions: 15 years experience from north India. Int J Lepr Other Mycobact Dis. 2004;72(2):125–33.
Ramien ML, Wong A, Keystone JS. Severe refractory erythema nodosum leprosum successfully treated with the tumor necrosis factor inhibitor etanercept. Clin Infect Dis. 2011;52(5):e133–5.
Bjorvatn B, Barnetson RS, Kronvall G, Zubler RH, Lambert PH. Immune complexes and complement hypercatabolism in patients with leprosy. Clin Exp Immunol. 1976;26(3):388–96.
Nunzie E, Ortega Cabrera LV, Macanchi Moncayo FM, Ortega Espinosa PF, Clapasson A, Massone C. Lucio leprosy with Lucio’s phenomenon, digital gangrene and anticardiolipin antibodies. Lepr Rev. 2014;85(3):194–200.
Smith CS, Noordeen SK, Richardus JH, Sansarricq H, Cole ST, Soares RC, Savioli L, Aerts A, Baruaf S. A strategy to halt leprosy transmission. Lancet Infect Dis. 2014;14(2):96–8.
Moschella SL. An update on the diagnosis and treatment of leprosy. J Am Acad Dermatol. 2004;51(3):417–26.
Scollard DM, Gillis TP, Williams DL. Polymerase chain reaction assay for the detection and identification of Mycobacterium leprae in patients in the United States. Am J Clin Pathol. 1998;109(5):642–6.
Ramos-e-Silva M, Rebello PF. Leprosy. Recognition and treatment. Am J Clin Dermatol. 2001;2(4):203–11.
Martinez AN, Talhari C, Moraes MO, Talhari S. PCR-based techniques for leprosy diagnosis: from the laboratory to the clinic. PLoS Negl Trop Dis. 2014;8(4):e2655.
Lockwood DNJ. Commentary: leprosy and poverty. Int J Epidemiol. 2004;33(2):269–70.
Lockwood DN, Kumar B. Treatment of leprosy. BMJ. 2004;328(7454):1447–8.
Kaimal S, Thappa DM. Relapse in leprosy. Indian J Dermatol Venereol Leprol. 2009;75(2):126–35.
Girdhar BK, Girdhar A, Kumar A. Relapses in multibacillary leprosy patients: effect of length of therapy. Lepr Rev. 2000;71(2):144–53.
Lockwood DN, Saunderson PR. Nerve damage in leprosy: a continuing challenge to scientists, clinicians and service providers. Int Health. 2012;4(2):77–85.
Upputuri B, Pallapati MS, Tarwater P, Srikantam A. Thalidomide in the treatment of erythema nodosum leprosum (ENL) in an outpatient setting: a five-year retrospective analysis from a leprosy referral centre in India. PLoS Neg Trop Dis. 2020;14(10):1–13.
Biosca G, Casallo S, López-Vélez R. Methotrexate treatment for type 1 (reversal) leprosy reactions. Clin Infect Dis. 2007;45(1):e7–9.
Moet FJ, Pahan D, Schuring RP, Oskam L, Richardus JH. Physical distance, genetic relationship, age, and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosy. J Infect Dis. 2006;193(3):346–53.
Richardus JH, Oskam L. Protecting people against leprosy: chemoprophylaxis and immunoprophylaxis. Clin Dermatol. 2015;33(1):19–25.
World Health Organization. Regional Office for South-East Asia. Leprosy: overcoming the remaining challenges. Geneva: World Health Organization; 2015. https://apps.who.int/iris/handle/10665/164331.
Pandey A. Current perspectives on leprosy as a public health challenge in India. Res Rep Trop Med. 2015;6:43–8.
Worobec S. Current approaches and future directions in the treatment of leprosy. Res Rep Trop Med. 2012;3:79–91.
Santos VS, de Souza CDF, Martins-Filho PRS, Cuevas LE. Leprosy: why does it persist among us? Expert Rev Anti-Infect Ther. 2020;18(7):613–5.
Lustosa AA, Nogueira LT, dos Santos Pedrosa JI, Teles JBM, Campelo V. The impact of leprosy on health-related quality of life. Rev Soc Bras Med Trop. 2011;44(5):621–6.
Penna ML, de Oliveira ML, Penna GO. The epidemiological behaviour of leprosy in Brazil. Lepr Rev. 2009;80(3):332–44.
Goulart IMB, Goulart LR. Leprosy: diagnostic and control challenges for a worldwide disease. Arch Dermatol Res. 2008;300:269–90.
Raffe SF, Thapa M, Khadge S, Tamang K, Hagge D, Lockwood DNJ. Diagnosis and treatment of leprosy reactions in integrated services—the patients’ perspective in Nepal. PLoS Neg Trop Dis. 2013;7(3):e2089.
Barrett R. Self-mortification and the stigma of leprosy in northern India. Med Anthropol Q. 2005;19(2):216–30.
Naaz F, Mohanty PS, Bansal AK, Kumar D, Gupta UD. Challenges beyond elimination in leprosy. Int J Mycobacteriol. 2017;6(3):222–8.
Kerr-Pontes LRS, Montenegro ACD, Barreto ML, Werneck GL, Feldmeier H. Inequality and leprosy in Northeast Brazil: an ecological study. Int J Epidemiol. 2004;33(2):262–9.
Rao PSS, John A. Nutritional status of leprosy patients in India. Indian J Lepr. 2012;84:17–22.
Barreto JG, Guimarães Lde S, Leão MR, Ferreira DV, Lima RA, Salgado CG. Anti-PGL-I seroepidemiology in leprosy cases: household contacts and school children from a hyperendemic municipality of the Brazilian Amazon. Lepr Rev. 2011;82(4):358–70.
Sarkar R, Pradhan S. Leprosy and women. Int J Womens Dermatol. 2016;2(4):117–21.
Alves CR, Ribeiro MM, Melo EM, Araújo MG. Teaching of leprosy: current challenges. An Bras Dermatol. 2014;89(3):454–9.
Palit A, Inamadar AC. Histoid leprosy as reservoir of the disease; a challenge to leprosy elimination. Lepr Rev. 2007;78(1):47–9.
Antunes DE, Goulart IMB, Goulart LR. Will cases of leprosy reaction increase with covid-19 infection? PLoS Neg Trop Dis. 2020;14(7):1–4.
Kar HK, Gupta R. Treatment of leprosy. Clin Dermatol. 2015;33(1):55–65.
Young RA, Mehra V, Sweetser D, Buchanan T, Clark-Curtiss J, Davis RW, et al. Genes for the major protein antigens of the leprosy parasite Mycobacterium leprae. Nature. 1985;316(6027):450–2.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The author declares no conflicts of interest.
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Borah Slater, K. (2023). A Current Perspective on Leprosy (Hansen’s Disease). In: Christodoulides, M. (eds) Vaccines for Neglected Pathogens: Strategies, Achievements and Challenges . Springer, Cham. https://doi.org/10.1007/978-3-031-24355-4_3
Download citation
DOI: https://doi.org/10.1007/978-3-031-24355-4_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24354-7
Online ISBN: 978-3-031-24355-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)