
Abstract
Lung injury can occur secondary to a myriad of causes, including infection, immunologic disorders, drug toxicity, or inhalational injury among others. Although the list of causative agents is long, the lung’s response to injury is limited resulting in similar patterns of disease irrespective of the cause. From a pathological perspective, acute lung injury refers to a group of entities that present with acute or subacute disease. These conditions are characterized by particular histological patterns including diffuse alveolar damage, acute fibrinous and organizing pneumonia, organizing pneumonia, and eosinophilic pneumonia and clinically correspond to the varying degrees of acute respiratory distress syndrome (Patel et al, Chest 125:197–202, 2004; Beasley et al, Arch Pathol Lab Med 126:1064–1070, 2002; Avecillas et al, Clin Chest Med 27:549–557, 2006; Cottin, Cordier, Semin Respir Crit Care Med 33:462–475, 2012; Ferguson et al, Intensive Care Med 38:1573–1582, 2012). In most cases, the underlying cause will not be apparent from the histological findings requiring close correlation with clinical history and laboratory findings to determine the etiology. Nevertheless, careful search for infectious organisms with application of histochemical and immunohistochemical stains should be performed in all cases in order to identify cases that benefit from more targeted treatment.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Lipoid pneumonia
- Eosinophilic pneumonia
- Aspiration pneumonia
- Organizing pneumonia
- Acute fibrinous and organizing pneumonia (AFOP)
- Diffuse alveolar damage
Lung injury can occur secondary to a myriad of causes, including infection, immunologic disorders, drug toxicity, or inhalational injury among others. Although the list of causative agents is long, the lung’s response to injury is limited resulting in similar patterns of disease irrespective of the cause. From a pathological perspective, acute lung injury refers to a group of entities that present with acute or subacute disease. These conditions are characterized by particular histological patterns including diffuse alveolar damage, acute fibrinous and organizing pneumonia, organizing pneumonia, and eosinophilic pneumonia and clinically correspond to the varying degrees of acute respiratory distress syndrome [1,2,3,4,5]. All these histological manifestations have in common an acute or subacute clinical course and an association with a wide range of underlying etiologic agents or an idiopathic setting. In most cases, the underlying cause will not be apparent from the histological findings requiring close correlation with clinical history and laboratory findings to determine the etiology. Nevertheless, careful search for infectious organisms with application of histochemical and immunohistochemical stains should be performed in all cases in order to identify cases that benefit from more targeted treatment. In this setting, large biopsy specimens (such as wedge biopsy) offer the best method to confirm the diagnosis as smaller samples may not yield sufficient diagnostic clues. Two other entities included in this chapter are aspiration pneumonia and lipoid pneumonia, representing pneumonias of non-infectious origin. These conditions develop secondary to aspiration or inhalation of food or particulate matter; however superimposed bacterial infection can occur as a complication in both entities.
1 Diffuse Alveolar Damage
Diffuse alveolar damage (DAD) is a response of the lung to acute injury that is characterized by damage to the alveolocapillary unit and represents the histopathological correlate of acute respiratory distress syndrome (ARDS) . There are numerous etiologic causes that can result in a pattern of DAD (Table 2.1). These include infection, sepsis, shock, trauma, transfusion, inhalational injury, drug reactions, metabolic disorders, and immunologic diseases, although the cause is often multifactorial [3, 6,7,8]. In cases in which no causative etiology can be elicited, the clinical term acute interstitial pneumonitis is applied [9,10,11]. DAD is generally a diffuse and bilateral process, but a subset of cases may demonstrate localized alveolar damage [12]. Histologically, DAD can be divided into an acute (exudative) and an organizing (proliferative) phase with some authors also recognizing a final fibrotic phase (Table 2.2). These phases are not necessarily progressive, and recovery can occur at any time [13, 14]. Furthermore, although most patients suffer only one episode of DAD, disease recurrence has been reported, especially in the setting of drug reactions [15].
1.1 Clinical Features
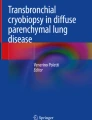
Patients with ARDS typically have an acute onset of their disease, characterized by dyspnea, cough, fever, and decreased diffusing capacity for carbon monoxide resulting in hypoxia. Radiographically, ARDS is classically described has showing diffuse bilateral pulmonary infiltrates (white out) in mid- and lower lobe distribution on chest X-ray. High-resolution computed tomography scans show scattered or diffuse areas of ground glass opacities in early ARDS (Fig. 2.1a, b) and marked architectural distortion and honeycombing in the later stages of the disease [16]. Fluid management, mechanical ventilation, corticosteroids, and vasodilators are the mainstay of treatment of ARDS [17,18,19]. Newer management approaches have reduced the mortality rate of patients with ARDS from approximately 50% to 35% [15]. While most survivors have no significant residual pulmonary deficits, in others, restrictive pulmonary disease may develop secondary to pulmonary fibrosis [17, 20].

(a) Computed tomography scan of the chest of a patient with acute respiratory distress syndrome demonstrates diffuse bilateral ground glass opacities and consolidation in the lung; (b) sagittal views show the extent of the disease involving all pulmonary lobes
1.2 Pathological Features
In the acute or exudative phase of lung injury in DAD, the lungs will be heavy and rigid with a dusky red-blue surface and hemorrhagic and airless parenchymal cut surface [13]. Histologically, the main findings include capillary congestion, interstitial and intraalveolar edema, and hyaline membranes (Fig. 2.2a, b). These hyaline membranes are composed of plasma proteins, surfactant components, and cellular debris which are condensed into glassy-appearing eosinophilic membranes that line the alveolar septa and alveolar ducts (Fig. 2.3). The alveolar septa are widened by edema and sparse inflammatory cells consisting of lymphocytes, plasma cells, and macrophages (Fig. 2.4). Microthrombi can be present quite extensively, and type II pneumocyte hyperplasia with regenerative cytologic atypia is another common finding (Fig. 2.5a, b). The proliferative phase is the phase of organization of the intraalveolar and interstitial exudate acquired in the acute phase [9, 13, 21]. Macroscopically, the lungs are solid and have a diffusely pale gray cut surface [13]. Microscopic examination shows formation of organized granulation tissue characterized by a loose proliferation of fibroblasts and myofibroblasts involving the alveolar septa and to a minor degree the alveolar spaces (Fig. 2.6a, b). Further changes include type II pneumocyte hyperplasia and squamous metaplasia, both of which can show striking cytologic atypia which should not be mistaken for malignancy (Fig. 2.7). Microthrombi, vascular remodeling, and wedge-shaped infarcts are further features, but hyaline membranes are not prominent [9, 13, 21]. In the fibrotic phase, gross examination shows a cobblestone appearance of the pleural surface and pale parenchymal cut surface with microcysts and scarring [13]. Histologically, the air spaces are enlarged and surrounded by thickened and fibrotic alveolar septa. The fibrosis is uniform and can be associated with areas of honeycombing (Fig. 2.8). Vascular changes in form of intimal or mural fibrosis or arterial muscularization can lead to pulmonary hypertension [9, 13, 21].

(a) Low power view of the pulmonary parenchyma affected by diffuse alveolar damage in the exudative phase; (b) higher magnification shows prominent capillary congestion and interstitial edema

Dense eosinophilic hyaline membranes lining the alveolar spaces are the pathognomonic histological feature of diffuse alveolar damage

Sparse inflammatory cells can usually be identified in the alveolar septa in diffuse alveolar damage

(a) Microthrombi in the vasculature of a lung with diffuse alveolar damage; (b) the lung parenchyma in diffuse alveolar damage can show striking type II pneumocyte hyperplasia

(a) Organizing granulation tissue characterizes the proliferative phase of diffuse alveolar damage; (b) higher power shows a proliferation of loose fibroblasts and myofibroblasts

Foci of squamous metaplasia are a common finding in diffuse alveolar damage

The fibrotic phase of diffuse alveolar damage is characterized by a non-specific uniform fibrotic process
1.3 Differential Diagnosis
The histological changes of DAD are non-specific and the underlying etiology is often not apparent. Close correlation with clinical history and laboratory findings and application of stains for fungi, mycobacteria, and bacteria or immunohistochemistry for viruses in immunocompromised patients is strongly recommended in the workup of any case of DAD. On a histologic level, the differential diagnosis includes acute fibrinous and organizing pneumonia (AFOP), organizing pneumonia (OP), and non-specific interstitial pneumonia (NSIP). AFOP is characterized by the presence of intraalveolar organizing fibrin balls and organizing fibroblastic tissue. Contrary to AFOP, the histologic hallmark of DAD is hyaline membranes, the presence of which is highly suggestive of the condition. Likewise, hyaline membranes are not a feature of OP in which the principal finding is organizing fibrous tissue. The fibrosis occurring in the organizing and fibrotic phases of DAD may be reminiscent of interstitial lung disease, especially NSIP. The fibrosis DAD is usually loose and myxoid and not as dense as that of NSIP. In addition, the striking type II pneumocyte hyperplasia seen in DAD is not as prominent a feature of NSIP.
2 Acute Fibrinous and Organizing Pneumonia
The pattern of acute fibrinous and organizing pneumonia (AFOP) was first reported by Beasley et al. in 2002 to describe a histologic pattern of acute lung injury that was distinct from those of diffuse alveolar damage (DAD), eosinophilic pneumonia, or organizing pneumonia [2]. AFOP is an uncommon response to lung injury characterized by intraalveolar fibrin deposition and organizing fibroblastic tissue but without the presence of hyaline membranes. The clinical course ranges from patients that present in a subacute fashion with eventual recovery to those with acute onset of respiratory distress and rapid progression to death. AFOP may be the consequence of a variety of different etiologies, including infection, collagen vascular disease, drug reaction, environmental exposure, and organ transplantation although idiopathic cases have also been described [2, 22,23,24,25,26]. While best treatment of the disease remains under investigation, the mortality rate continues to be high (50%) suggesting that AFOP may clinically and histologically represent a variant of DAD [2]. From a pathologist’s perspective, it should be noted that a diagnosis of AFOP requires large biopsy specimens (open lung biopsy or video-assisted thoracoscopic biopsy) as organizing alveolar fibrin may be a non-specific reaction to other processes and bronchoscopy and bronchoalveolar lavage (BAL) usually provide non-specific findings.
2.1 Clinical Features
Based on its association with a wide range of clinical conditions, AFOP can affect patients of any age but is most commonly reported in individuals between 50 and 70 years of age. Men are affected slightly more frequently than women [27]. Two different clinical patterns of AFOP have been described. In the acute form, there is rapid onset of the disease with fast development of respiratory failure and death with an average time from onset of symptoms to death of 29 days; in the subacute form, the clinical course is less aggressive with slower progression [2, 22, 28, 29]. Patients commonly present with dyspnea, cough, fever, pleural effusions, and progressive respiratory failure. The radiological findings of AFOP closely resemble those of DAD and comprise diffuse basilar-dependent consolidation, ground glass opacities, and interlobular septal thickening [2, 30] (Fig. 2.9). In the subacute form, imaging findings may be indistinguishable from those of organizing pneumonia and can include focal and diffuse parenchymal abnormalities [2, 31,32,33]. The treatment of AFOP is largely based on treating the underlying condition and often includes administration of corticosteroids and immunosuppressive therapy [22]. Despite this, patients with fulminant AFOP often succumb to their disease, while patients with subacute AFOP eventually recover [2].

On chest computed tomography, a case of acute fibrinous and organizing pneumonia presents with diffuse consolidation in the right lower lobe of the lung
2.2 Pathological Features
The dominant finding in specimens with AFOP is the presence of intraalveolar fibrin filling the alveolar spaces (Fig. 2.10). This often takes the form of “fibrin balls” (Fig. 2.11). The distribution of the fibrin is typically patchy with intervening uninvolved lung parenchyma showing minimal interstitial widening or inflammatory cell infiltration (Fig. 2.12). Classic hyaline membranes, however, as seen in DAD are not a feature of AFOP. In addition to the fibrin balls, AFOP will harbor intraluminal loose connective tissue within alveolar ducts and bronchioles (Fig. 2.13a, b). Other associated findings may include type II pneumocyte hyperplasia, alveolar edema, or vascular thrombi (Fig. 2.14). Of note, infiltrates consisting of neutrophils, eosinophils, and macrophages or fibrotic changes are typically absent [2].

Histologically, acute fibrinous and organizing pneumonia shows areas of intraalveolar fibrin deposition

The fibrin often assumes a ball-like configuration in acute fibrinous and organizing pneumonia

Areas of intervening normal lung parenchyma (left) typically alternate with involved lung (right) in acute fibrinous and organizing pneumonia

(a) Another characteristic feature of acute fibrinous and organizing pneumonia is the presence of intraluminal loose connective tissue; (b) higher magnification shows the polypoid nature of the fibrous plugs

Type II pneumocyte hyperplasia with reactive atypia is typically seen along the alveolar walls in acute fibrinous and organizing pneumonia
2.3 Differential Diagnosis
The differential diagnosis of AFOP includes other conditions associated with acute lung injury, including DAD, eosinophilic pneumonia, and organizing pneumonia (Table 2.3). The histopathological hallmark of DAD is the presence of hyaline membranes, which although they may be focal will invariably have to be present for the diagnosis to be made. Although AFOP is also characterized by organizing fibrin deposition, hyaline membranes are not a feature of this condition, and their presence would rather be indicative of DAD. Intraalveolar fibrin may also be found in eosinophilic pneumonia; however, the latter typically contains abundant eosinophils admixed with macrophages, the presence of which would preclude a diagnosis of AFOP. The dominant finding in organizing pneumonia is intraluminal fibroblastic plugs. Although organizing fibroblastic tissue is also seen in AFOP, the most striking histologic finding in this condition is the presence of organizing fibrin balls which in turn will be absent in organizing pneumonia.
3 Organizing Pneumonia
The term organizing pneumonia (OP), previously referred to as bronchiolitis obliterans organizing pneumonia (BOOP), is used to describe a characteristic histological pattern that is a non-specific response to lung injury. It is composed of polypoid plugs of proliferating fibroblasts and myofibroblasts within the lumen of small airways and alveolar spaces and associated interstitial inflammation [34, 35]. OP may be idiopathic in origin (clinically corresponding to cryptogenic organizing pneumonia) or a secondary process due to a wide range of underlying etiologies, such as infection, collagen vascular disease, drug reaction, radiation, environmental or occupational exposure, or organ transplantation [36]. Classically, OP presents in a subacute manner and with diffuse lung disease [37]; however, a rare form of the disease has been reported with an acute onset leading to rapid respiratory failure and need for mechanical ventilation (rapid progressive OP) [38, 39]. Another form of the disease presenting as a solitary lung nodule or multiple nodular masses has been termed localized OP or focal nodular OP [40,41,42,43]. This form accounts for 13–14% of all cases of OP and is easily mistaken for primary lung cancer or metastatic disease based on initial clinical and radiological investigations [44, 45]. Furthermore, OP may occur as an integral component of other conditions, such as hypersensitivity pneumonitis, acute and fibrinous organizing pneumonia (AFOP), or organizing diffuse alveolar damage (DAD), or it can be a non-specific reaction to an adjacent unrelated lesion [46].
3.1 Clinical Features
Due to the association with a variety of different etiologies, OP can affect patients of any age group. The most common form of OP however is the idiopathic form which tends to affect men and women equally and with an average age around 50 years. There appears to be no direct relationship with smoking. Presenting symptoms include cough, shortness of breath, or a flu-like illness with fever [38, 45, 47]. Patients with the localized form of the disease are often asymptomatic [41,42,43, 48, 49] while those with the accelerated form rapidly progress to respiratory failure [38, 39]. Pulmonary function tests often show a decrease in vital capacity and reduced diffusion capacity [38]. Radiologically, most patients present with various patterns of diffuse parenchymal abnormalities. These include bilateral consolidation, especially in a peripheral or peribronchial pattern, triangular-shaped bilateral ground glass opacities, or peribronchial or peribronchiolar nodules [50] (Fig. 2.15). Chest X-ray of rapid progressive OP will show a white-out of both lungs and CT findings include ground glass opacities and alveolar consolidation. In localized OP , chest radiographs and CT scans will reveal solitary or multiple lung nodules with an average size around 2–3 cm [48, 49]. These nodules are round or oval-shaped and have smooth, irregular, or spiculated margins (Fig. 2.16). Of note, fluorodeoxyglucose-positron emission tomography (FDG-PET) is often positive in these lesions making differentiation from primary or metastatic lung tumors even more difficult [48, 49, 51]. Surgery is the treatment of choice and usually curative in cases of localized OP while corticosteroids, antibiotics, and immunosuppressive therapy are typically administered in the remaining cases. With appropriate treatment, the prognosis is usually favorable in most cases of OP and the lung will heal without permanent damage [52,53,54]. However, in severe cases, lung injury can occur and can lead to permanent damage and interstitial fibrosis [44, 52, 53, 55,56,57].

Computed tomography scan of the chest of a patient with organizing pneumonia shows bilateral subpleural areas of consolidation

On a computed tomography scan, localized organizing pneumonia may present as a solitary pulmonary nodule closely resembling lung malignancy
3.2 Pathological Features
Irrespective of the clinical presentation of the disease, the histological hallmark of OP is polypoid intraluminal plugs of fibroblasts and myofibroblasts predominantly within airspaces and with varying degrees of bronchiolar involvement (Fig. 2.17). Their distribution is typically patchy, and on hematoxylin-eosin stains, they have a characteristic gray-blue hue (Fig. 2.18a, b). A mild to moderate interstitial infiltrate may be present in the septa of areas of organization and may lead to associated type II pneumocyte hyperplasia (Fig. 2.19). The general lung architecture, however, remains intact. Neutrophils, eosinophils, granulomas, and significant fibrosis should not be present, but foci of bronchial or squamous metaplasia can sometimes be identified [4, 37, 58,59,60] (Fig. 2.20).

Low power magnification of a case of organizing pneumonia shows scattered intraluminal plugs of granulation tissue

(a) The tissue plugs have a scattered distribution and (b) often have a bluish-gray appearance on hematoxylin-eosin staining

The lung adjacent to organizing pneumonia often shows hyperplastic changes of the alveolar lining cells (left)

Areas of squamous metaplasia in a case of organizing pneumonia (right lower)
3.3 Differential Diagnosis
Although the histologic pattern of OP is quite distinctive, one needs to remember that an OP-like reaction may form part of other disease entities that need to be excluded before a diagnosis of OP can be established. As mentioned above, hypersensitivity pneumonitis is defined by the histological triad of cellular bronchiolitis, ill-defined non-caseating granulomas, and localized areas of OP. Careful search for additional histologic findings as well as attention to the clinical findings such as antigen exposure and poorly defined centrilobular nodules on high-resolution CT are required to distinguish these entities [61]. Moreover, fibroblastic lesions (fibroblastic foci) similar to those seen in OP are commonly associated with usual interstitial pneumonia (UIP) and may be difficult to differentiate especially in small biopsy samples. However, in contrast to OP, UIP shows heterogeneous fibrotic lesions in a spatial distribution, variable degrees of smooth muscle proliferation, and honeycombing. In contrast, OP is more uniform in appearance with more prominent polypoid intraluminal lesions and architectural preservation. Another entity, DAD, may show granulation tissue polyps in bronchioles and alveolar ducts. However, in contrast to OP, DAD typically also contains hyaline membranes with or without organization. When these features are resolving in the later phase of DAD, the differential diagnosis on histologic features alone may be difficult and always requires close clinical correlation [62]. OP-like changes are also a component of a pattern of acute lung injury named AFOP. In addition to the OP-like changes, AFOP is defined by the presence of organizing fibrin in the alveolar spaces. While these organizing fibrin balls are the principal finding in AFOP, organizing fibroblastic tissue dominates the histological picture in OP.
4 Eosinophilic Pneumonia
Eosinophilic pneumonia, as defined by Liebow and Carrington in 1969 [63], refers to a pneumonic process caused by infiltration of the pulmonary parenchyma by eosinophils that may or may not be accompanied by eosinophilia in the peripheral blood. Eosinophilic pneumonia can be divided into two forms, acute eosinophilic pneumonia (AEP) and chronic eosinophilic pneumonia (CEP), based on clinical parameters and response to therapy [64]. AEP is a clinical entity characterized by an acute febrile illness, normal number of blood eosinophils, and dramatic response to corticosteroid therapy [64], while patients with CEP present with chronic and progressive clinical features, peripheral blood eosinophilia, and frequent relapse after discontinuation of corticosteroids [65]. Both forms of the disease may be the consequence of a range of different etiologies, including inhalation of toxins, drug reaction, or infection or may be idiopathic [66,67,68,69]. The development of AEP has also been reported in association with cigarette smoking and exposure to dust or smoke from fireworks [70,71,72].
4.1 Clinical Features
Patients with AEP typically present with an acute onset of respiratory insufficiency, hypoxemia, and fever. Peripheral blood eosinophil percentages are usually normal, but the number of eosinophils in bronchoalveolar lavage (BAL) fluid is increased. Pulmonary function testing during the acute phase often shows a restrictive pattern. In contrast, the onset of CEP is insidious with an average time from onset of symptoms to diagnosis of 7.7 months [65]. Patients are typically middle-aged and women are more commonly affected than men; about half of the patients have a history of asthma. Pulmonary functions tests are mostly normal but can also show restrictive defects [65, 73, 74]. Peripheral blood eosinophilia is typically present and usually mild to moderate and increased IgE levels can be found in two thirds of patients. Analogous to AEP, the percentage of eosinophils in BAL fluid is very high [65, 75, 76]. Radiographic findings in AEP include bilateral reticular densities and pleural effusion, while in CEP non-segmental airspace consolidation in a peripheral and upper lobe distribution is seen [16, 77]. CT scans demonstrate bilateral patchy areas of ground glass opacity, interlobular septal thickening, consolidation and poorly defined nodules in AEP, and areas of airspace consolidation, ground glass opacities, nodules, and reticulation in CEP. Contrary to AEP, pleural effusion is observed in CEP in less than 10% of cases [16, 77]. Both AEP and CEP are highly responsive to treatment with corticosteroids often achieving a rapid clinical response. Unlike patients with CEP who need to be treated with prolonged therapy due to a high short-term relapse rate, those with AEP usually do not experience disease recurrence after discontinuation of corticosteroids [68, 78].
4.2 Pathological Features
In general, eosinophilic pneumonia is characterized by diffuse infiltration of varying numbers of eosinophils, macrophages, and intraalveolar fibrin (Fig. 2.21). Eosinophils can also be seen in thickened interstitial spaces and the walls of blood vessels, or they can form small microabscesses (Fig. 2.22). Hyaline membranes reminiscent of those seen in diffuse alveolar damage may be seen in cases of AEP [68, 79], while in CEP intraluminal fibrosis is often identified [65, 68, 80, 81]. Additional findings can include type II pneumocyte hyperplasia, foci of intraalveolar necrosis, and Charcot-Leyden crystals [65, 79].

Diffuse tissue infiltration by eosinophils mixed with histiocytes is the histologic hallmark of eosinophilic pneumonia

In some areas, the eosinophilic infiltrate in eosinophilic pneumonia can form small microabscesses
4.3 Differential Diagnosis
The histopathological differential diagnosis of eosinophilic pneumonia primarily includes diffuse alveolar damage (DAD), acute fibrinous and organizing pneumonia (AFOP), and Churg-Strauss syndrome. Distinction from these entities is important due to the dramatic clinical response of patients with eosinophilic pneumonia upon administration of corticosteroid therapy. Cases of DAD and AFOP may share several histological features with eosinophilic pneumonia, such as hyaline membranes or intraalveolar fibrin deposition, respectively. Contrary to eosinophilic pneumonia, however, the presence of numerous eosinophils and macrophages is not characteristic for these entities, and their occurrence would rather point toward a diagnosis of eosinophilic pneumonia. Churg-Strauss syndrome on the other hand typically shows an eosinophilic parenchymal infiltrate coupled with the presence of a necrotizing vasculitis and granulomas; the latter features are not usually seen in cases of eosinophilic pneumonia.
5 Aspiration Pneumonia
Aspiration of food or other foreign material can be the cause of a chemical or bacterial pneumonia that most commonly occurs in patients with altered levels of consciousness and subsequent impairment of protective upper and lower airway reflexes. Predisposing factors include chronic debilitation, neurologic disorders, obstetric or emergency surgical intervention, drug overdoses, or syncopal episodes [82,83,84,85]. More recently, this disease process has also been described in previously healthy patients, in whom aspiration was unsuspected clinically and pathologically [84]. Most aspirated material is composed of food or other particulate matter such as seeds, vegetable peel or pits, chicken bones, gum, talc, and microcrystalline material among others [84, 86].
5.1 Clinical Features
Patients are often in the 6th or 7th decade of life, and males seem to be more frequently affected than females [84, 85]. Common presenting symptoms include dyspnea, fever, cough, weakness, or lethargy. The right lung is involved more commonly, due to the fact that the right main bronchus is wider and enters the lung at a steeper angle than the left one. Radiologically, aspiration pneumonia can manifest as confluent air space opacification in the dependent portions of the lungs or small nodular and branching opacities (tree-in-bud pattern) centered on the bronchioles [87]. The initial therapy for aspiration pneumonia depends on the rapid recognition of the event and treatment of hypoxemia with supplemental oxygen [88]. Antibiotic treatment is often administered empirically. Pleural drainage may be necessary in patients in whom complications of aspiration pneumonia occur such as lung abscess, empyema, or bronchopleural fistula [88].
5.2 Pathological Features
The most common pathological finding in aspiration pneumonia is organizing pneumonia (OP) characterized by intraluminal fibroblast plugs around small bronchioles, alveolar ducts, and peribronchiolar spaces. This OP-like reaction is often accompanied by multinucleate giant cells and/or acute inflammation, foreign body type granulomas engulfing the aspirated material, acute bronchopneumonia or bronchiolitis, and scattered microabscesses (Fig. 2.23a–d). In addition, suppurative granulomas with central necrotic neutrophils or necrosis surrounded by epithelioid histiocytes can be identified [84]. A relatively constant finding is the presence of aspirated foreign material with is usually located in the airspaces but may occasionally also be seen in the interstitium in which case fibrosis is a common related finding [84] (Fig. 2.24a, b). The particulate matter is often surrounded by giant cells and accompanied by a neutrophilic infiltrate. However, not all cases in which aspiration is clinically documented show the presence of particulate matter in the lung and a granulomatous tissue reaction may be absent [85]. In these cases, the pattern of lung injury can mimic diffuse alveolar damage characterized by fibrin exudation within air spaces leading to the formation of hyaline membranes. The microscopic appearance of the foreign matter depends on the type of aspirated material. Vegetable particles often consist of septate eosinophilic or basophilic structures rimmed by a hyaline cuticle and with a sieve-like inner structure whereas talc or crystalline material presents as refractile yellow-gray sheet-like material or large gray cord-like structures [85] (Fig. 2.25a, b). Hence the importance of examining all cases of suspected aspiration under polarized light in order to identify the potential presence of birefringent material within macrophages or multinucleate giant cells.

(a) Aspiration pneumonia showing the demarcation between affected and uninvolved lung; (b) the lung is replaced by an inflammatory process composed of aspirated material with associated fibrous reaction and foci of abscess formation; (c) aspirated vegetable matter surrounded by multinucleate foreign body-type giant cells; (d) granulomatous reaction around small inspissated foreign body material

(a) Vegetable matter often has a rigid sieve-like appearance in aspiration pneumonia; (b) aspirated vegetable material in the bronchial lumen of the lung

(a) Fragmented vegetable matter in an airway in a case of aspiration pneumonia; (b) birefringent starch particles with characteristic Maltese cross appearance in a case of aspiration pneumonia when viewed under polarized light
5.3 Differential Diagnosis
From a histologic point of view, the differential diagnosis includes other disease processes presenting with OP, granulomatous inflammation, multinucleate giant cells, and acute or subacute inflammatory changes. Infections causing a granulomatous response in particular can resemble aspiration pneumonia, and special stains and tissue cultures to search for infectious organisms are essential in the work up of such cases. Bronchocentric granulomatosis is another process that may enter the differential diagnosis due to the presence of a granulomatous process surrounding bronchioles. Mucoid impaction, tissue eosinophilia, and the absence of foreign material usually advocates a diagnosis of bronchocentric granulomatosis in this context. Another granulomatous disease, granulomatosis with polyangiitis (Wegener granulomatosis), consists of a combination of necrotizing granulomas, multinucleate giant cells, and suppuration and may hence mimic aspiration pneumonia. Necrotizing vasculitis, however, another feature that defines granulomatosis with polyangiitis is absent in aspiration pneumonia. Lastly, intravenous drug abuse may result in the deposition of foreign material in the lung. In these cases, however, the material will be deposited within the walls or the lumina of arterial vessels and not in the bronchioles thereby separating this process from aspiration pneumonia [84].
6 Lipoid Pneumonia
Lipoid pneumonia is an uncommon form of pneumonia that is characterized by the presence of lipid material within alveolar spaces and alveolar macrophages. In the past, lipoid pneumonia has been reported under various different names such as paraffinoma, cholesterol pneumonia, golden pneumonia, or lipoid granulomatosis [89,90,91]. Lipoid pneumonia can be divided into exogenous and endogenous types depending on the source of the lipid. Exogenous lipoid pneumonia usually occurs through ingestion or inhalation of vegetable or animal fats or mineral oils whereas endogenous lipoid pneumonia is the result of lipid accumulation within alveolar macrophages in the setting of bronchial obstruction, chronic pulmonary infection, pulmonary alveolar proteinosis, and fat storage diseases [92, 93]. The precise incidence of lipoid pneumonia is difficult to determine although an autopsy series reported a frequency of 1.0–2.5% [94].
6.1 Clinical Features
Aspiration or inhalation of fatty substances is the causative factor for exogenous lipoid pneumonia. Aspiration is often due to abnormality in deglutition or neuromuscular diseases affecting pharyngeal motility or the cough reflex. In healthy individuals, aspiration may be occupation related (fire eaters) or due to use of oil-based laxatives, oil-based nose drops, lip balm, or petroleum jelly among others. Patients most commonly present with dyspnea, cough, and fever. Radiologically, exogenous lipoid pneumonia can show airspace consolidation, ground glass attenuation, airspace nodules, and crazy-paving pattern (interlobular septal thickening), preferentially affecting the lower lobes [95]. Endogenous lipoid pneumonia is an obstructive type of pneumonitis that was first described in association with lung neoplasms [96]. It can also occur with diseases that are unassociated with bronchial obstruction such as infections, pulmonary alveolar proteinosis, or lipid storage disorders due to physical or chemical effects of airway blockage [97,98,99,100,101]. The clinical and radiological presentation largely depends on the underlying etiology. Exposure avoidance and supportive care are the treatment of choice for exogenous lipoid pneumonia. Systemic corticosteroids or whole-lung lavage may be indicated in more severe cases [102,103,104]. Surgical resection may be indicated in cases of endogenous lipoid pneumonia, especially in cases of suspected lung cancer. Lipoid pneumonia is generally an indolent condition that may regress spontaneously; however, rarely, disease progression is seen leading to superinfection, respiratory insufficiency, or cor pulmonale [105,106,107].
6.2 Pathological Features
Pathologically, the aspirated or inhaled material in exogenous lipoid pneumonia accumulates in alveolar macrophages which acquire a foamy or vacuolated look or elicits a foreign body giant cell reaction that can lead to the formation of giant cell granulomas (Fig. 2.26a–d). In addition, there may be varying degrees of inflammation in the alveolar walls and interlobular septa. Interstitial fibrosis with resulting architectural distortion may develop in lesions of longer duration. Lipid-containing vacuoles may be seen in the alveolar spaces or the interstitium especially in older lesions [108] (Fig. 2.27). In endogenous lipoid pneumonia, lipid material is derived from breakdown products related to obstruction, cancer cell disintegration, or anoxic tissue injury. Often this results in the formation of low-density lipoprotein cholesterol which is apparent on microscopy as cholesterol crystals [109,110,111,112].


(a) Low power view of lipoid pneumonia; (b) numerous lipid vacuoles can be seen in the alveolar spaces; (c) the vacuoles typically elicit a giant cell or granulomatous reaction; (d) high power magnification shows that the vacuoles are often engulfed by foreign body-type giant cells

In some cases of lipoid pneumonia, the lipid vacuoles can also be seen expanding the interstitial septa
6.3 Histochemical Features
The lipid material in alveolar macrophages or in the interstitial septa can be demonstrated using histochemical stains such as oil red O or Sudan black. Cholesterol crystals in cases of endogenous lipoid pneumonia can be visualized with a Schultz stain (sulfuric acid and acetic acid).
6.4 Differential Diagnosis
The histological pattern of lipoid pneumonia may be confused with other granulomatous or histiocytic conditions, especially infectious diseases. The absence of infectious organisms on special stains or cultures studies in combination with the presence of lipid material and clinical history usually confirm the diagnosis.
References
Patel SR, Karmpaliotis D, Ayas NT, et al. The role of open-lung biopsy in ARDS. Chest. 2004;125:197–202.
Beasley MB, Franks TJ, Galvin JR, et al. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002;126:1064–70.
Avecillas JF, Freire AX, Arroliga AC. Clinical epidemiology of acute lung injury and acute respiratory distress syndrome: incidence, diagnosis, and outcomes. Clin Chest Med. 2006;27:549–57.
Cottin V, Cordier JF. Cryptogenic organizing pneumonia. Semin Respir Crit Care Med. 2012;33:462–75.
Ferguson ND, Fan E, Camporota L, et al. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med. 2012;38:1573–82.
Bernard GR, Artigas A, Brigham KL, et al. Report of the American-European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee. Intensive Care Med. 1994;20:225–32.
Bernard GR. Acute respiratory distress syndrome: a historical perspective. Am J Respir Crit Care Med. 2005;172:798–806.
Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–49.
Katzenstein AL, Bloor CM, Liebow AA. Diffuse alveolar damage – the role of oxygen, shock, and related factors. A review. Am J Pathol. 1976;85:209–28.
American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. Am J Respir Crit Care Med. 2002;165:277–304.
Katzenstein AL, Myers JL, Mazur MT. Acute interstitial pneumonia. A clinicopathologic, ultrastructural, and cell kinetic study. Am J Surg Pathol. 1986;10:256–67.
Yazdy AM, Tomashefski JF Jr, Yagan R, et al. Regional alveolar damage (RAD). A localized counterpart of diffuse alveolar damage. Am J Clin Pathol. 1989;92:10–5.
Tomashefski JF Jr. Pulmonary pathology of acute respiratory distress syndrome. Clin Chest Med. 2000;21:435–66.
Meduri GU. Late adult respiratory distress syndrome. New Horiz. 1993;1:563–77.
Savici D, Katzenstein AL. Diffuse alveolar damage and recurrent respiratory failure: report of 6 cases. Hum Pathol. 2001;32:1398–402.
Rossi SE, Erasmus JJ, McAdams HP, et al. Pulmonary drug toxicity: radiologic and pathologic manifestations. Radiographics. 2000;20:1245–59.
Bellani G, Laffey JG, Pham T, et al. LUNG SAFE Investigators; ESICM Trials Group. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800.
Koh Y. Update in acute respiratory distress syndrome. J Intensive Care. 2014;2:2.
Hager DN. Recent advances in the management of the acute respiratory distress syndrome. Clin Chest Med. 2015;36:481–96.
Gattinoni L, Caironi P, Valenza F, et al. The role of CT-scan studies for the diagnosis and therapy of acute respiratory distress syndrome. Clin Chest Med. 2006;27:559–70.
Castro CY. ARDS and diffuse alveolar damage: a pathologist’s perspective. Semin Thorac Cardiovasc Surg. 2006;18:13–9.
Garcia BA, Goede T, Mohammed TL. Acute fibrinous organizing pneumonia: a case report and literature review. Curr Probl Diagn Radiol. 2015;44:469–71.
Hariri LP, Unizony S, Stone J, et al. Acute fibrinous and organizing pneumonia in systemic lupus erythematosus: a case report and review of the literature. Pathol Int. 2010;60:755–9.
Hariri LP, Mino-Kenudson M, Shea B, et al. Distinct histopathology of acute onset or abrupt exacerbation of hypersensitivity pneumonitis. Hum Pathol. 2012;43:660–8.
Otto C, Huzly D, Kemna L, Hüttel A, et al. Acute fibrinous and organizing pneumonia associated with influenza A/H1N1 pneumonia after lung transplantation. BMC Pulm Med. 2013;13:30.
Sauter JL, Butnor KJ. Expanding the spectrum of pulmonary histopathological manifestations of anti-synthetase syndrome: anti-EJ-associated acute fibrinous and organizing pneumonia. Histopathology. 2014;65:581–2.
Arnaud D, Surani Z, Vakil A, et al. Acute fibrinous and organizing pneumonia: a case report and review of the literature. Am J Case Rep. 2017;18:1242–6.
Saxena P, Kumar K, Mittal S, et al. Acute fibrinous and organizing pneumonia: a rare form of nonbacterial pneumonia. Indian J Crit Care Med. 2016;20:245–7.
Nguyen LP, Ahdoot S, Sriratanaviriyakul N, et al. Acute fibrinous and organizing pneumonia associated with allogenic hematopoietic stem cell transplant successfully treated with corticosteroids: a two-patient case series. J Investig Med High Impact Case Rep. 2016;4:2324709616643990.
Prahalad S, Bohnsack JF, Maloney CG, et al. Fatal acute fibrinous and organizing pneumonia in a child with juvenile dermatomyositis. J Pediatr. 2005;146:289–92.
Valim V, Rocha RH, Couto RB, et al. Acute fibrinous and organizing pneumonia and undifferentiated connective tissue disease: a case report. Case Rep Rheumatol. 2012;2012:549298.
Kobayashi H, Sugimoto C, Kanoh S, et al. Acute fibrinous and organizing pneumonia: initial presentation as a solitary nodule. J Thorac Imaging. 2005;20:291–3.
Tzouvelekis A, Koutsopoulos A, Oikonomou A, et al. Acute fibrinous and organising pneumonia: a case report and review of the literature. J Med Case Rep. 2009;3:74.
Cordier JF. Bronchiolitis obliterans organizing pneumonia. Semin Respir Crit Care Med. 2000;21:135–46.
Myers JL, Colby TV. Pathologic manifestations of bronchiolitis, constrictive bronchiolitis, cryptogenic organizing pneumonia, and diffuse panbronchiolitis. Clin Chest Med. 1993;14:611–22.
Epler GR. Bronchiolitis obliterans organizing pneumonia, 25 years: a variety of causes, but what are the treatment options? Expert Rev Respir Med. 2011;5:353–61.
Hughes KT, Beasley MB. Pulmonary manifestations of acute lung injury: more than just diffuse alveolar damage. Arch Pathol Lab Med. 2017;141:916–22.
Chang J, Han J, Kim DW, et al. Bronchiolitis obliterans organizing pneumonia: clinicopathologic review of a series of 45 Korean patients including rapidly progressive form. J Korean Med Sci. 2002;17:179–86.
Chakravorty I, Oldfield WL, Gómez CM. Rapidly progressive bronchiolitis obliterans organising pneumonia presenting with pneumothorax, persistent air leak, acute respiratory distress syndrome and multi-organ dysfunction: a case report. J Med Case Rep. 2008;2:145.
Cordier JF. Cryptogenic organizing pneumonitis. Bronchiolitis obliterans organizing pneumonia. Clin Chest Med. 1993;14:677–92.
Kohno N, Ikezoe J, Johkoh T, et al. Focal organizing pneumonia: CT appearance. Radiology. 1993;189:119–23.
Akira M, Yamamoto S, Sakatani M. Bronchiolitis obliterans organizing pneumonia manifesting as multiple large nodules or masses. AJR Am J Roentgenol. 1998;170:291–5.
Watanabe K, Harada T, Yoshida M, et al. Organizing pneumonia presenting as a solitary nodular shadow on a chest radiograph. Respiration. 2003;70:507–14.
Lohr RH, Boland BJ, Douglas WW, et al. Organizing pneumonia. Features and prognosis of cryptogenic, secondary, and focal variants. Arch Intern Med. 1997;157:1323–9.
Cazzato S, Zompatori M, Baruzzi G, et al. Bronchiolitis obliterans-organizing pneumonia: an Italian experience. Respir Med. 2000;94:702–8.
Beasley MB. The pathologist’s approach to acute lung injury. Arch Pathol Lab Med. 2010;134:719–27.
Oymak FS, Demirbaş HM, Mavili E, et al. Bronchiolitis obliterans organizing pneumonia. Clinical and roentgenological features in 26 cases. Respiration. 2005;72:254–62.
Melloni G, Cremona G, Bandiera A, et al. Localized organizing pneumonia: report of 21 cases. Ann Thorac Surg. 2007;83:1946–51.
Maldonado F, Daniels CE, Hoffman EA, et al. Focal organizing pneumonia on surgical lung biopsy: causes, clinicoradiologic features, and outcomes. Chest. 2007;132:1579–83.
Kligerman SJ, Franks TJ, Galvin JR. From the radiologic pathology archives: organization and fibrosis as a response to lung injury in diffuse alveolar damage, organizing pneumonia, and acute fibrinous and organizing pneumonia. Radiographics. 2013;33:1951–75.
Shin L, Katz DS, Yung E. Hypermetabolism on F-18 FDG PET of multiple pulmonary nodules resulting from bronchiolitis obliterans organizing pneumonia. Clin Nucl Med. 2004;29:654–6.
Cordier JF. Cryptogenic organising pneumonia. Eur Respir J. 2006;28:422–46.
Drakopanagiotakis F, Paschalaki K, Abu-Hijleh M, et al. Cryptogenic and secondary organizing pneumonia: clinical presentation, radiographic findings, treatment response, and prognosis. Chest. 2011;139:893–900.
Yoo JW, Song JW, Jang SJ, et al. Comparison between cryptogenic organizing pneumonia and connective tissue disease-related organizing pneumonia. Rheumatology (Oxford). 2011;50:932–8.
Myers JL, Katzenstein AL. Ultrastructural evidence of alveolar epithelial injury in idiopathic bronchiolitis obliterans-organizing pneumonia. Am J Pathol. 1988;132:102–9.
Davison AG, Heard BE, McAllister WA, et al. Cryptogenic organizing pneumonitis. Q J Med. 1983;52:382–94.
Epler GR, Colby TV, McLoud TC, et al. Bronchiolitis obliterans organizing pneumonia. N Engl J Med. 1985;312:152–8.
Yousem SA, Lohr RH, Colby TV. Idiopathic bronchiolitis obliterans organizing pneumonia/cryptogenic organizing pneumonia with unfavorable outcome: pathologic predictors. Mod Pathol. 1997;10:864–71.
Epler GR. Bronchiolitis obliterans organizing pneumonia. Arch Intern Med. 2001;161:158–64.
Epler GR. Bronchiolitis obliterans organizing pneumonia: definition and clinical features. Chest. 1992;102:2S–6S.
Herráez I, Gutierrez M, Alonso N, et al. Hypersensitivity pneumonitis producing a BOOP-like reaction: HRCT/pathologic correlation. J Thorac Imaging. 2002;17:81–3.
Kitaichi M. Differential diagnosis of bronchiolitis obliterans organizing pneumonia. Chest. 1992;102:44S–9S.
Liebow AA, Carrington CB. The eosinophilic pneumonias. Medicine (Baltimore). 1969;48:251–85.
Allen JN, Davis WB. Eosinophilic lung diseases. Am J Respir Crit Care Med. 1994;150:1423–38.
Jederlinic PJ, Sicilian L, Gaensler EA. Chronic eosinophilic pneumonia. A report of 19 cases and a review of the literature. Medicine (Baltimore). 1988;67:154–62.
Allen JN, Pacht ER, Gadek JE, et al. Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. N Engl J Med. 1989;321:569–74.
King MA, Pope-Harman AL, Allen JN, et al. Acute eosinophilic pneumonia: radiologic and clinical features. Radiology. 1997;203:715–9.
Philit F, Etienne-Mastroïanni B, Parrot A, et al. Idiopathic acute eosinophilic pneumonia: a study of 22 patients. Am J Respir Crit Care Med. 2002;166:1235–9.
Pope-Harman AL, Davis WB, Allen ED, et al. Acute eosinophilic pneumonia. A summary of 15 cases and review of the literature. Medicine (Baltimore). 1996;75:334–42.
Shintani H, Fujimura M, Yasui M, et al. Acute eosinophilic pneumonia caused by cigarette smoking. Intern Med. 2000;39:66–8.
Rom WN, Weiden M, Garcia R, et al. Acute eosinophilic pneumonia in a New York City firefighter exposed to World Trade Center dust. Am J Respir Crit Care Med. 2002;166:797–800.
Hirai K, Yamazaki Y, Okada K, et al. Acute eosinophilic pneumonia associated with smoke from fireworks. Intern Med. 2000;39:401–3.
Carrington CB, Addington WW, Goff AM, et al. Chronic eosinophilic pneumonia. N Engl J Med. 1969;280:787–98.
Fox B, Seed WA. Chronic eosinophilic pneumonia. Thorax. 1980;35:570–80.
Naughton M, Fahy J, FitzGerald MX. Chronic eosinophilic pneumonia. A long-term follow-up of 12 patients. Chest. 1993;103:162–5.
Dejaegher P, Demedts M. Bronchoalveolar lavage in eosinophilic pneumonia before and during corticosteroid therapy. Am Rev Respir Dis. 1984;129:631–2.
Jeong YJ, Kim KI, Seo IJ, et al. Eosinophilic lung diseases: a clinical, radiologic, and pathologic overview. Radiographics. 2007;27:617–37.
Ogawa H, Fujimura M, Matsuda T, et al. Transient wheeze. Eosinophilic bronchobronchiolitis in acute eosinophilic pneumonia. Chest. 1993;104:493–6.
Tazelaar HD, Linz LJ, Colby TV, et al. Acute eosinophilic pneumonia: histopathologic findings in nine patients. Am J Respir Crit Care Med. 1997;155:296–302.
Mochimaru H, Kawamoto M, Fukuda Y, et al. Clinicopathological differences between acute and chronic eosinophilic pneumonia. Respirology. 2005;10:76–85.
Allen J. Acute eosinophilic pneumonia. Semin Respir Crit Care Med. 2006;27:142–7.
Knoblich R. Pulmonary granulomatosis caused by vegetable particles. So-called lentil pulse pneumonia. Am Rev Respir Dis. 1969;99:380–9.
Passarino G, Ciccone G, Siragusa R, et al. Histopathological findings in 851 autopsies of drug addicts, with toxicologic and virologic correlations. Am J Forensic Med Pathol. 2005;26:106–16.
Mukhopadhyay S, Katzenstein AL. Pulmonary disease due to aspiration of food and other particulate matter: a clinicopathologic study of 59 cases diagnosed on biopsy or resection specimens. Am J Surg Pathol. 2007;31:752–9.
Yousem SA, Faber C. Histopathology of aspiration pneumonia not associated with food or other particulate matter: a clinicopathologic study of 10 cases diagnosed on biopsy. Am J Surg Pathol. 2011;35:426–31.
Kollef MH, Winn RE. Occult coiled drinking straw aspiration. Heart Lung. 1990;19:24–6.
Marom EM, McAdams HP, Sporn TA, et al. Lentil aspiration pneumonia: radiographic and CT findings. J Comput Assist Tomogr. 1998;22:598–600.
Johnson JL, Hirsch CS. Aspiration pneumonia. Recognizing and managing a potentially growing disorder. Postgrad Med. 2003;113:99–102.
Hoffman LR, Yen EH, Kanne JP, et al. Lipoid pneumonia due to Mexican folk remedies: cultural barriers to diagnosis. Arch Pediatr Adolesc Med. 2005;159:1043–8.
Gondouin A, Manzoni P, Ranfaing E, et al. Exogenous lipid pneumonia: a retrospective multicentre study of 44 cases in France. Eur Respir J. 1996;9:1463–9.
Bhagat R, Holmes IH, Kulaga A, et al. Self-injection with olive oil. A cause of lipoid pneumonia. Chest. 1995;107:875–6.
Baron SE, Haramati LB, Rivera VT. Radiological and clinical findings in acute and chronic exogenous lipoid pneumonia. J Thorac Imaging. 2003;18:217–24.
Woodhead M, Parkes WR. Disorders caused by other agents. In: Parkes WR, editor. Occupational lung disorders. 3rd ed. Oxford, UK: Butterworth-Heinemann; 1994. p. 778–93.
Rouffy J, Almosni M, Chelloul N, et al. Current aspects of exogenous pulmonary lipoidosis in adults. Review of the recent literature apropos of an exemplary case. Ann Med Interne (Paris). 1976;127:637–43.
Marchiori E, Zanetti G, Mano CM, et al. Exogenous lipoid pneumonia. Clinical and radiological manifestations. Respir Med. 2011;105:659–66.
McDonald JR, Woolner LB. Malignant tumors of the lung; their diagnosis by cytologic examination of sputum and bronchial secretions. Minn Med. 1949;32(12):1186–9.
Burke M, Fraser R. Obstructive pneumonitis: a pathologic and pathogenetic reappraisal. Radiology. 1988;166:699–704.
Cohen AB, Cline MJ. In vitro studies of the foamy macrophage of postobstructive endogenous lipoid pneumonia in man. Am Rev Respir Dis. 1972;106:69–78.
Gaerte SC, Meyer CA, Winer-Muram HT, et al. Fat-containing lesions of the chest. Radiographics. 2002;22:S61–78.
Nicholson AG, Wells AU, Hooper J, et al. Successful treatment of endogenous lipoid pneumonia due to Niemann-Pick Type B disease with whole-lung lavage. Am J Respir Crit Care Med. 2002;165:128–31.
Itoh Y, Segawa H, Kito K, et al. Lipoid pneumonia with chronic myelomonocytic leukemia. Pathol Res Pract. 2009;205:143–7.
Hadda V, Khilnani GC, Bhalla AS, et al. Lipoid pneumonia presenting as non-resolving community acquired pneumonia: a case report. Cases J. 2009;2:9332.
Chin NK, Hui KP, Sinniah R, et al. Idiopathic lipoid pneumonia in an adult treated with prednisolone. Chest. 1994;105:956–7.
Chang HY, Chen CW, Chen CY, et al. Successful treatment of diffuse lipoid pneumonitis with whole lung lavage. Thorax. 1993;48:947–8.
Greenberger PA, Katzenstein AL. Lipid pneumonia with atypical mycobacterial colonization. Association with allergic bronchopulmonary aspergillosis. Arch Intern Med. 1983;143:2003–5.
Dixon C, Bolivar R, Katz R, et al. Lipoid pneumonia and Mycobacterium fortuitum pulmonary infection: successful treatment with sulfisoxazole. Tex Med. 1985;81:57–60.
Casey JF. Chronic cor pulmonale associated with lipoid pneumonia. JAMA. 1961;177:896–8.
Laurent F, Philippe JC, Vergier B, et al. Exogenous lipoid pneumonia: HRCT, MR, and pathologic findings. Eur Radiol. 1999;9:1190–6.
Tamura A, Hebisawa A, Fukushima K, et al. Lipoid pneumonia in lung cancer: radiographic and pathological features. Jpn J Clin Oncol. 1998;28:492–6.
Taki T, Nakazima T, Emi Y, et al. Accumulation of surfactant phospholipids in lipid pneumonia induced with methylnaphthalene. Lipids. 1986;21:548–52.
Tölle A, Kolleck I, Schlame M, et al. Effect of hyperoxia on the composition of the alveolar surfactant and the turnover of surfactant phospholipids, cholesterol, plasmalogens and vitamin E. Biochim Biophys Acta. 1997;1346:198–204.
Evans AJ, Sawyez CG, Wolfe BM, et al. Evidence that cholesteryl ester and triglyceride accumulation in J774 macrophages induced by very low density lipoprotein subfractions occurs by different mechanisms. J Lipid Res. 1993;34:703–17.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Weissferdt, A. (2020). Acute Lung Injury and Non-infectious Pneumonias. In: Diagnostic Thoracic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-030-36438-0_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-36438-0_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-36437-3
Online ISBN: 978-3-030-36438-0
eBook Packages: MedicineMedicine (R0)