
Abstract
Osteomas are the most common benign sinonasal lesion with the frontal sinus the most common location. On sinus MRI, dried secretions show as hyperintense on T1, hypointense on T2, and polyps show hypointense on T1, hyperintense on T2. Rhinoscleroma is caused by Klebsiella rhinoscleromatis with histopathology showing Mikulicz cells (macrophages containing pathogen) and Russell bodies (plasma cells).
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Frontal Sinus
- Primary Ciliary Dyskinesia
- Middle Turbinate
- Functional Endoscopic Sinus Surgery
- Frontal Recess
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Pearls
-
Osteomas are the most common benign sinonasal lesion with the frontal sinus the most common location
-
On sinus MRI, dried secretions show as hyperintense on T1, hypointense on T2, and polyps show hypointense on T1, hyperintense on T2
-
Rhinoscleroma is caused by Klebsiella rhinoscleromatis with histopathology showing Mikulicz cells (macrophages containing pathogen) and Russell bodies (plasma cells)
Anatomy
-
Nasal Framework
-
Cartilages: Upper lateral, lower lateral, accessory sesamoid, quadrilateral septal
-
Bones: Nasal bones, vomer, perpendicular plate of the ethmoid, maxillary crest, palatine bone, anterior nasal spine of maxilla
-
Lateral nasal wall: inferior, middle, superior (sometimes supreme) turbinates
-
Inferior meatus (inferior to inferior turbinate): nasolacrimal duct opening (valve of Hasner)
-
Middle meatus (inferior to middle turbinate): Semilunar hiatus opens to ethmoid infundibulum which receives drainage from maxillary, anterior ethmoid, and frontal sinuses
-
Superior meatus (anteroinferior to superior turbinate): opening to posterior ethmoid sinuses
-
Sphenoethmoidal recess (posterosuperior to superior turbinate): opening to sphenoid sinuses
-
-
-
Blood supply
-
External carotid system
-
Facial artery
-
Angular artery (located in alar-facial groove): nasal sidewall, tip, and dorsum
-
Superior labial artery: columella, lateral wall
-
Internal maxillary artery (divides into terminal branches in pterygopalatine fossa)
-
Sphenopalatine artery (enters sphenopalatine foramen on lateral wall at junction of middle turbinate basal lamella and orbital wall)
-
Lateral nasal artery: anterior portion of lateral nasal wall
-
Posterior septal artery: courses over sphenoid face and supplies nasal septum
-
Descending palatine artery (found in greater palatine canal, then enters nasal cavity via incisive foramen): anterior nasal septum and nasal floor
-
-
-
Internal Carotid System
-
Ophthalmic artery terminates into anterior and posterior ethmoid arteries
-
Anterior ethmoid: Anterior and superior septum, lateral wall, and roof of nasal cavity
-
Posterior ethmoid: Superior turbinate, posterior septum
-
-
-
Nasal Plexuses
-
Kiesselbach’s plexus (Little’s area): anteroinferior 1/3 of nasal septum; junction of sphenopalatine, greater palatine, anterior ethmoid, and superior labial arteries
-
Woodruff’s plexus: posterior portion of inferior meatus and nasopharynx; junction of posterior nasal, sphenopalatine, and ascending pharyngeal veins
-
-
Venous drainage
-
Corresponds to arterial supply
-
“Danger triangle” = area of skin from the corners of the mouth to the bridge of the nose. Veins draining this region are valveless, so skin infection can easily spread retrograde intracranially via angular vein → inferior ophthalmic vein → cavernous sinus
-
-
-
Lymphatics
-
Anterior → facial nodes or upper cervical nodes
-
Posterior → retropharyngeal nodes
-
-
Innervation
-
Muscles of facial expression: CN VII
-
Sensory: branches of V1 and V2 for pain, temperature, and touch; CN I at roof of nasal cavity for olfaction
-
Parasympathetic (acetylcholine and VIP): superior salivatory nucleus of CN VII →greater superficial petrosal nerve → vidian nerve → sphenopalatine ganglion (synapse) → terminates on blood vessels and glands of the nasal mucosa (induces vasodilation and secretion)
-
Sympathetic (NE): superior cervical ganglion (synapse) → deep petrosal nerve → vidian nerve → terminates on blood vessels and glands of the nasal mucosa (induces vasoconstriction)
-
-
Paranasal sinuses
-
Maxillary sinus
-
Two periods of growth: age 3 and age 7–12, coincides with dental growth periods
-
Volume 15 cm3, triangular space completely bound within bone of maxilla
-
Ostium drains into middle meatus; accessory ostia present up to 30 % of the time
-
Separated from first and second molars by thin layer of bone, can be dehiscent; dental infections can spread to sinus via this route and chronic infection or removal of these teeth can cause an oroantral fistula
-
-
Ethmoid sinuses
-
Reach adult size by age 12, separated into anterior (2–8 cells)/posterior (1–5 cells) by basal lamella of middle turbinate, volume 15 cm3
-
Bound by sphenoid face posteriorly, lamina papyracea laterally, middle and superior turbinates medially, and skull base superiorly
-
Keros classification: can assist in determining risk of violating skull base during FESS
-
I: Cribriform plate 1–3 mm inferior to fovea ethmoidalis
-
II: 4–7 mm inferior
-
III: 8–16 mm inferior
-
-
Lamellae of ethmoid sinus:
-
Uncinate process (forms medial wall of ethmoid infundibulum)
-
Ethmoid bulla (largest anterior ethmoid air cell)
-
Basal lamella of middle turbinate (separates anterior from posterior ethmoid)
-
Lamella of superior turbinate
-
-
Retrobullar recess = space posterior to ethmoid bulla if bulla not fused to basal lamella
-
Suprabullar recess = space superior to ethmoid bulla if not fused to skull base
-
Agger nasi = most anterior ethmoid air cell, pneumatization of lacrimal bone, can block frontal recess
-
Supraorbital ethmoid cell = always posterolateral to true frontal sinus ostium can be confused for frontal sinus septation
-
Haller cell = infraorbital ethmoid cell pneumatizing into the maxillary sinus, can block maxillary sinus ostium
-
Onodi cell = posterior ethmoid cell located superolateral to sphenoid sinus, may interface with or contain the internal carotid and optic nerve
-
Ostiomeatal complex vs. ethmoid infundibulum vs. semilunar hiatus
-
Semilunar hiatus = 2D gap between uncinate and ethmoid bulla
-
Infundibulum = 3D space bounded by uncinate medially, lamina papyracea laterally, and frontal process of maxilla anterosuperiorly = route of drainage for maxillary, anterior ethmoid, and frontal sinuses
-
Ostiomeatal complex = includes middle turbinate, uncinate process, semilunar hiatus, ethmoid bulla, and infundibulum = functional drainage pathway for maxillary, anterior ethmoid, and frontal sinuses
-
-
-
Frontal sinus
-
Pneumatized portion of frontal bone
-
Drains through ostium into frontal recess (bounded by agger nasi anteriorly, ethmoid bulla posteriorly, lamina papyracea laterally, middle turbinate medially, skull base superiorly)
-
Drainage pattern determined by attachment of uncinate process (UP)
-
Attached to lamina papyracea (most common 60–70 %) → drains medial to UP
-
Attached to skull base (5–15 %) or middle turbinate (10–20 %) → drains lateral to UP
-
-
Visible on X-rays by age 2–6, continues growth into adolescence
-
Types of frontal cells:
-
I: Single cell above the agger nasi
-
II: Two or more cells above the agger nasi
-
III: Single cell extending from the agger nasi superiorly into frontal sinus
-
IV: Cell isolated within frontal sinus
-
-
-
Sphenoid sinus
-
Pneumatization from age 3–18
-
Landmarks: 30° angle relative to nasal floor, 1/3 distance superiorly from choana to skull base, 7 cm from nasal sill, at the same latitude as the roof of the maxillary sinus
-
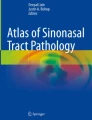
Closely related to internal carotid, optic nerve, vidian canal, foramen rotundum, cavernous sinus; extremely variable intersinus septum (Fig. 6.1)
Fig. 6.1 
Sphenoid sinus surrounded by critical structures (seen bilaterally, named from superior to inferior): optic nerve, carotid artery, V2, vidian nerve
-
-

Physiology
-
Histology
-
Pseudostratified ciliated columnar epithelium covers majority of nasal cavity except nasal vestibule (covered by stratified squamous epithelium)
-
Ciliated columnar cells (9 + 2 microtubules w/dynein arms, beat 10–20×/s), nonciliated columnar cells (microvilli covering surface increase surface area for humidification and warming), basal cells, and goblet cells (produce mucin which traps irritants)
-
-
-
Mucin physiology
-
Sol layer = deep lubricating layer, produced by microvilli
-
Gel layer = superficial viscous layer, produced by goblet cells, traps particles
-
Mucus flows → nasopharynx → secretions swallowed
-
-
Olfactory epithelium
-
Located along upper 1/3 of septum, medial superior/supreme turbinates, roof of nasal cavity
-
Gets roughly 15 % of nasal airflow
-
Neural sensory contributions from CN I and small contribution from CN V
-
Pseudostratified columnar epithelium with multiple different cell types:
-
Bipolar olfactory neurons (develop from neuroblasts; have cilia that do NOT beat)
-
Sustentacular cells (support cells, have microvilli, protective function)
-
Bowman’s glands (produce secretions that bathe olfactory epithelium, required to dissolve odorants prior to nerve stimulation)
-
Basal cells (differentiate into neurons or sustentacular cells)
-
-
-
Hyposmia/Anosmia: Caused by damage to nerve itself, inflammation, or obstruction of airflow preventing odorants from reaching the nerve
-
Most common causes are obstructive sinonasal disease/polyps or URI with suspected viral attack on nerve causing inflammation and dysfunction
-
Also consider trauma, tumors, iatrogenic surgical damage, chemical irritant or medication-induced damage, endocrine or metabolic disorders (e.g., hypothyroidism), age-related loss of smell (presbyosmia), or early signs of neurologic disease (Alzheimer’s or Parkinson’s disease)
-
Foster Kennedy Syndrome = unilateral anosmia, optic atrophy, and papilledema due to frontal lobe masses
-
Kallman’s syndrome = hypogonadotropic hypogonadism and anosmia (failure of hypothalamus to secrete GnRH, several types of inheritance including x-linked and autosomal dominant)
-
Evaluation and management of hyposmia/anosmia
-
Full history and physical examination including neurologic exam and rigid nasal endoscopy to identify any obvious possible underlying causes
-
Treat patients medically with course of oral steroids, nasal steroid spray, and nasal saline irrigations, then reevaluate in clinic to assess symptoms. Consider MRI for persistent symptoms to rule out masses/tumors.
-
UPSIT (University of Pennsylvania Smell Identification Test) can be used to identify malingering (score <10/40), for workman’s compensation documentation, and for research purposes
-
-
-
Evaluation of the nasal airway
-
Main functions: humidification, warming, filtration, olfaction, alteration of airway resistance
-
Nasal air flow = accounts for 50 % of total airway resistance
-
Internal nasal valve = most narrow part of nasal airway; bounded by nasal septum, upper lateral cartilage, head of inferior turbinate, and nasal floor
-
Evaluated by Cottle maneuver (subjective improvement in nasal breathing with lateral distraction of the ipsilateral cheek indicates internal valve collapse)
-
Nasal cycle = physiologic variation in vascular flow and sympathetic tone of nasal airway, engorgement of nasal tissue which alternates from one side to the other every 2–6 h
-
-
Objective measures of nasal airway resistance (commonly used only in research)
-
Rhinomanometry = placement of sensors in the nose or nasopharynx which calculate pressure generated by nasal airflow through the nose before and after nasal decongestant administered. Cannot localize site of obstruction, used in research only.
-
> 35 % decrease in airway resistance = mucosal congestion
-
< 35 % decrease in airway resistance = structural abnormality
-
-
Acoustic rhinometry = uses sound waves to measure the cross-sectional area at points along the nasal airway. Can identify narrow points in airway but unable to determine whether these narrow areas have any effect on nasal airflow.
-
-
Imaging
-
Air-fluid level = purulent secretions or blood after trauma (Fig. 6.2)
Fig. 6.2 
Air-fluid level seen in left maxillary sinus, indicating purulent secretion (and not blood) in this case, as there is no history or sign of trauma
-
Dried secretions = hyperintense on T1, hypointense on T2
-
Polyps = hypointense on T1, hyperintense on T2
-
Mycetoma (fungal ball) shows bony thickening of sinus walls on CT, hypointense on T1/T2
-
Allergic fungal sinusitis CT findings include a rim of low density within sinus with central mucin, calcifications, and bony expansion/erosion (Fig. 6.3)
Fig. 6.3 
Typical AFS imaging showing heterogeneous opacification of the sinuses and hypertelorism (fish eye effect) as the sinus cavity expands outwards, displacing the orbits laterally, to accommodate accumulating polyps and fungal mucin
-
Inverting papilloma shows bony thickening at attachment site on CT
-
Juvenile nasal angiofibroma enhances on CT (Fig. 6.4), hyperintense on MRI with flow voids; Holman-Miller sign = anterior bowing of posterior maxillary sinus wall
Fig. 6.4 
Right maxillary sinus, obstructed by enhancing mass seen within the right nasal cavity and ethmoid region, showing accumulation of post-obstructive secretions
-
Fibrous dysplasia has ground-glass appearance on CT, hypointense on T2 MRI (Fig. 6.5)
Fig. 6.5 
Classic “ground-glass” appearance of the bone in fibrous dysplasia




Rhinitis
-
Inflammation of nasal mucosa, affects 25 % of general population
-
Allergic: IgE-mediated release of immune mediators (histamine, leukotrienes, etc.) from mast cells in response to allergen exposure, type I hypersensitivity reaction
-
Symptoms = nasal congestion, sneezing, eye irritation, thin clear rhinorrhea
-
Immediate phase = within 5 min
-
Cross-linking of IgE and degranulation of mast cells releases histamine, leukotrienes, prostaglandin, and platelet activating factor (PAF)
-
Increases vascular permeability, produces main symptoms of rhinorrhea, sneezing, and congestion
-
-
Late phase = peaks at 6 h, lasts up to 24 h
-
Recurrence of symptoms due to recruitment of inflammatory cells by previously released cytokines
-
-
Perennial (i.e., dust mites, insects, dogs, or cats) versus seasonal (i.e., trees, grasses)
-
Diagnosed via history, skin prick testing or serum RAST
-
Treatment
-
Avoidance of specific allergens, topical antihistamine, anticholinergic, or steroid nasal sprays, oral antihistamines, antileukotrienes, antibody-directed immunomodulators, and subcutaneous or sublingual immunotherapy
-
-
-
Atrophic rhinitis
-
Seen after radical nasal surgery with over-resection of inferior and middle turbinate tissue, termed by some “empty nose syndrome”
-
Symptoms = mucosal atrophy, thick foul-smelling crust (ozena)
-
Pathology = transformation of respiratory epithelium into keratinized squamous epithelium, +/− superinfection with Klebsiella ozoena
-
Treatment = saline irrigations or gels, topical oil-based lubrication, alternative irrigations such as xylitol or alkalol. Surgical intervention limited to restructuring turbinate morphology
-
-
Nonallergic Rhinitis with Eosinophilia (NARES) = rhinorrhea, nasal pruritus, and sneezing related to asthma and aspirin sensitivity
-
No association with IgE-mediated hypersensitivity, negative allergy tests
-
Treatment = Symptomatic relief with nasal steroid spray, antihistamines
-
-
Vasomotor = excessive parasympathetic tone of nasal mucosa
-
Symptoms similar to allergic rhinitis (with hypersecretion of clear, thin mucus as main symptom) but allergy does not play a role
-
Triggers include exercise, anxiety, foods (gustatory rhinitis) or changes in temperature
-
Can also be seen in autonomic dysregulation, commonly seen in elderly patients, or after stroke
-
Treatment = Elimination of triggers and environmental irritants if possible, topical nasal steroid or anticholinergic sprays, or surgery (surface turbinate cautery, partial turbinectomy, or nasal branches of vidian neuronectomy)
-
-
Medication-induced
-
Antihypertensives, antidepressants, anti-inflammatory drugs
-
Rhinitis medicamentosa = rebound congestion caused by prolonged use of topical alpha adrenergic medications
-
Treatment = stop use of topical vasoconstrictors, begin nasal saline +/− nasal steroid spray, may use oral steroid burst for severe nasal obstruction
-
-
Hormone-induced (pregnancy, menstruation, oral contraceptives, hypothyroidism)
-
Estrogen inhibits ACh-esterase → elevated ACh levels → increased parasympathetic tone
-
Treatment = conservative measures including nasal saline, avoid decongestants while pregnant
-
-
Infectious
-
Usually viral (most commonly rhinovirus, coronavirus) but can predispose to bacterial superinfection, managed symptomatically
-
Bacterial colonization:
-
MRSA colonization of anterior nasal cavity commonly found in health care workers, hospitalized patients, treated with Mupirocin ointment to nasal cavity
-
Rhinosporidiosis
-
Rhinosporidium seeberi, a eukaryotic parasitic pathogen
-
Symptoms = unilateral nasal obstruction, epistaxis, friable polyps
-
Pathology = pseudoepitheliomatous hyperplasia, chitinous shells
-
Treatment = surgical excision
-
-
Rhinoscleroma
-
Klebsiella rhinoscleromatis
-
Symptoms = three stages
-
Catarrhal (nonspecific crusting)
-
Granulomatous (epistaxis, friable mucosa, nodules throughout upper respiratory tract)
-
Sclerotic (sclerosis and fibrosis)
-
Pathology = Mikulicz cells (macrophages containing pathogen) and Russell bodies (plasma cells)
-
Common in Central America, Africa, India
-
Treatment = long-term antibiotics
-
-
-
-
Rhinosinusitis
-
Fungal Sinusitis
-
Invasive
-
Acute
-
Occurs in immunocompromised patients (AIDS, malignancy, DM, immunosuppressive meds); fungal invasion into mucosa, soft tissues, and bone, seen as invasion of blood vessels on microscopy
-
Presents as pallor or eschar in nasal cavity or along palate +/− numbness or pain, CT findings of mucosal thickening, sinus opacification (usually maxillary sinus), and infiltration of retroantral fat
-
Rapidly progressive (over hours) and can be fatal due to intracranial extension
-
Mucormycosis: more common in uncontrolled DM (diabetic ketoacidosis), broad-based ribbon-like nonseptate hyphae with 90° branching
-
Aspergillus fumigatus: more common in immunocompromised patients, narrow septate hyphae with branching at acute 45° angles
-
Treatment = aggressive surgical debridement until healthy bleeding tissue is reached, IV antifungals, treatment of underlying disease process or adjustment of medications to alleviate immunosuppression
-
-
Chronic Granulomatous
-
Fungal invasion of sinonasal tissue with indolent course, produces granulomatous inflammatory response
-
Aspergillus flavus most common
-
Treatment = surgical debridement + systemic antifungals
-
-
-
Noninvasive
-
Mycetoma (fungus ball)
-
Isolated sinus opacification, usually maxillary or sphenoid
-
Aspergillus common, although fungal cultures can be negative
-
Treatment = surgical removal
-
-
Allergic fungal rhinosinusitis
-
Bent & Kuhn Criteria for diagnosis:
-
History of Type I Hypersensitivity
-
Nasal polyps
-
Allergic mucin (contains eosinophils or their breakdown products Charcot-Leyden crystals)
-
Presence of fungal elements on stain or culture (Aspergillus or dematiaceous fungi)
-
Characteristic CT findings (unilateral opacification, sinus wall erosion or expansion, heterogeneous density)
-
Lack of invasion
-
-
Treatment = FESS to open sinuses and remove accumulated thick mucus and polyps, allergy testing and immunotherapy if positive to prevent relapse, often these patients benefit from steroid, whether oral or topical
-
-
-
-
Rhinosinusitis
-
Classification
-
Acute < 4 weeks
-
Recurrent ARS requires four or more episodes with complete resolution of symptoms between episodes
-
-
Subacute 4–12 weeks
-
Chronic > 12 weeks
-
CRSsNP (without nasal polyps) +/− eosinophilia or CRSwNP (with nasal polyps) +/− eosinophilia
-
Acute exacerbation of CRS = worsening of chronic symptoms with return to baseline after treatment but without complete resolution of symptoms
-
-
Criteria for diagnosis: inflammation of nose and paranasal sinuses characterized by specific symptoms
-
Older classification required two major factors (facial pain, nasal congestion, nasal discharge, hyposmia, purulence in nasal cavity) or one major factor and two minor factors (headache, fever, fatigue, cough, ear pain, or pressure)
-
2012 European Position Paper on rhinology classification requires two symptoms—one must be nasal congestion or nasal discharge (other sx = endoscopic signs of edema, purulent discharge, polyps, and mucosal changes on CT)
-
Diagnosis should be supported by endoscopic or CT evidence of disease
-
-
-
-
-
Acute rhinosinusitis
-
Etiology
-
Viral (most commonly rhinovirus, coronavirus) or bacterial (most commonly Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis)
-
Pathophysiology: Viral infection causes upregulation of inflammatory factors and leads to mucus hypersecretion and mucosal edema. In combination with a variety of predisposing factors (e.g., trauma, anatomic obstruction, ciliary dysmotility, immune factors), this can lead to mucus stasis or obstruction of sinus outflow tracts → provides ideal setting for bacterial growth
-
Treatment
-
Supportive care and reassurance for mild symptoms
-
Antibiotics for severe symptoms (first line = amoxicillin or cephalosporins; if symptoms do not improve then second line = amoxicillin-clavulanate or respiratory quinolones), culture-directed, if possible
-
Nasal saline irrigations
-
Intranasal steroids, short course oral steroids (can improve facial pain, headache)
-
Oral analgesics and mucolytics
-
-
Complications:
-
Orbital complications—described in increasing severity by Chandler’s classification
-
Preseptal cellulitis
-
Periorbital soft tissue erythema/edema
-
No chemosis, vision changes, or dysmotility
-
Tx = oral antibiotics
-
-
Orbital cellulitis
-
Inflammation within orbit
-
Presence of chemosis, proptosis, limited mobility, and/or vision changes
-
Tx = IV antibiotics + functional endoscopic sinus surgery (FESS)
-
-
Subperiosteal abscess
-
Similar to orbital cellulitis WITH presence of pus between orbital periosteum and bone
-
Tx = IV antibiotics + FESS and surgical drainage of abscess. Can consider antibiotics alone for a small abscess in a clinically stable patient <2–4 years old without vision change, but should monitor closely with immediate surgical intervention available for signs of progression
-
-
Orbital abscess
-
Pus located within the orbit
-
Severe proptosis and ophthalmoplegia
-
Tx = IV antibiotics + FESS and surgical drainage
-
-
Cavernous sinus thrombosis
-
Structures which pass through cavernous sinus: CN III, IV, V1, V2, VI, internal carotid artery, and multiple venous channels
-
Symptoms = ophthalmoplagia, headache, periorbital sensory loss, papilledema/proptosis/periorbital edema/vision loss (from venous congestion); CN VI first to show effects
-
Tx = IV antibiotics + FESS (+/− anti-thrombotics, controversial)
-
Infections from sinuses spread directly or via hematogenous spread, most commonly from ethmoids
-
Always obtain ophthalmology consultation and document visual acuity, extent of proptosis, measurement of pressure, and eye movements (important to perform forced duction testing to examine if limit to EOM is due to pain or pathology)
-
General indications for OR = change in or loss of vision or EOM, or any other cranial nerve deficit
-
-
-
Intracranial complications
-
Epidural, subdural, or intracranial abscess (Tx = IV antibiotics +/− neurosurgical drainage)
-
Meningitis = headache, altered mental status, high fever, neck stiffness (Tx = first obtain head CT, LP if no intracranial mass seen on CT, IV antibiotics)
-
Infection spreads via direct extension, along olfactory nerve sheath, or hematogenously (foramina of Breschet = venous perforators connecting intracranial and extracranial vascular supply), most common from frontal sinus
-
-
Pott’s Puffy Tumor
-
Osteomyelitis of anterior table of frontal sinus
-
Infection transmitted via diploic veins → swelling of adjacent forehead soft tissue
-
Tx = IV antibiotics, FESS and surgical debridement of sequestered bone
-
-
Mucocele
-
Expansile collection of secretions trapped within an obstructed sinus
-
CT = sinus expansion and bony erosion; MRI T2 = hyperintense
-
Tx = FESS, with open procedures for inaccessible lesions
-
-
Superior Orbital Fissure Syndrome
-
Due to infectious spread to or trauma involving superior orbital fissure
-
Structures included: III, IV, V1, VI, ophthalmic vein, and sympathetic fibers
-
Symptoms = ophthalmoplegia, ptosis, proptosis, ipsilateral forehead paresthesia, and fixed dilated pupil
-
-
Orbital Apex Syndrome
-
Symptoms of superior orbital fissure syndrome + involvement of CN II (vision change or blindness)
-
-
-
-
-
Chronic Rhinosinusitis (CRS)
-
Contributing factors
-
Microbial factors
-
Biofilms = aggregate of bacteria encased in self-produced polysaccharide matrix which confers antibiotic resistance
-
Superantigens = bacterial exotoxins which trigger a much larger downstream T-cell activation than traditional exotoxins without requiring antigen specificity
-
-
Environmental factors (smoking, pollution, allergens)
-
Anatomic factors (septal deviation, concha bullosa, infraorbital cells, scarring, etc.)
-
Mucociliary dysfunction
-
Primary ciliary dyskinesia (PCD) = AR defect in dynein arms of cilia of respiratory tract and reproductive system → URIs, otitis media, infertility
-
Kartagener’s syndrome = PCD + situs inversus and bronchiectasis
-
Cystic fibrosis = AR mutation in CFTR gene which impairs chloride transport → thick mucus prevents clearing of bacteria (diagnosed with sweat chloride test)
-
-
Immunologic factors
-
Allergy
-
Nasal mucosal congestion which occurs in allergic rhinitis → obstruction of sinus ostia → impaired sinus ventilation → mucus retention and infection
-
-
Samter’s Triad
-
Sinonasal polyposis, asthma, and aspirin sensitivity
-
ASA ingestion → inhibits cyclo-oxygenase metabolism of arachidonic acid → stimulates 5-lipo-oxygenase and production of leukotrienes → asthma and allergy effects
-
-
-
-
Pathophysiology is complex and multifactorial, involving any of the above listed factors which contribute to mucosal inflammation
-
Treatment
-
3–6 weeks treatment with antibiotics (amoxicillin-clavulanate, respiratory quinolones, second-generation cephalosporins, etc.)
-
Topical nasal steroid spray, oral steroid taper, nasal saline irrigation, mucolytics
-
Treatment of any underlying allergy
-
Surgery for patients refractory to medical management, mucoceles, or signs of orbital/intracranial complications
-
-
Epistaxis
-
Anterior source 90 % of the time
-
Etiologies
-
Local
-
Digital trauma, facial trauma
-
Inflammation or infection
-
Septal deviation or perforation (aberrant airflow causes drying of tissues which become friable)
-
Dry nasal environment (CPAP, decongestants, dry climates)
-
Foreign bodies (local irritation or secondary to attempts at removal)
-
Tumors (secondary to erosion into vessels)
-
Carotid aneurysm (rare, usually a late complication occurring several years after trauma accompanied by monocular blindness)
-
-
Systemic
-
TB, Wegener’s granulomatosis (respiratory tract granulomas, vasculitis, and glomerulonephritis), sarcoidosis (noncaseating granulomas), syphilis
-
Symptoms = crusting, friable mucosa, septal perforation
-
Osler Weber Rendu Disease (Hereditary hemorrhagic telangiectasia)
-
Autosomal dominant, numerous small vascular malformations of the skin and mucosal linings of the aerodigestive tract, AVMs of larger organs (lung, liver, brain)
-
Epistaxis and GI bleeding common, onset at puberty and worsens with age
-
Lack of normal vascular smooth muscle, impairs ability to contract
-
Treated with bipolar cautery or laser ablation, septodermoplasty, or nasal closure as a last resort
-
Use of bevacizumab (Avastin), a VEGF inhibitor, increasing, currently under study
-
-
-
Blood dyscrasias
-
Alcoholism, malnutrition, malignancy, immunodeficiency, liver or kidney failure
-
Characterized by reduced platelet aggregation, prolonged bleeding time; treat with platelet transfusion for severe bleeds
-
Von Willebrand disease
-
Deficiency of von Willebrand protein leads to defective platelet adhesion and decreased activity of clotting factor VIII; treat with DDAVP, cryoprecipitate, or von Willebrand protein concentrate for severe bleeds
-
-
Hemophilia
-
Deficiency in clotting factor VIII (type A) or IX (type B); treat with factor VIII or IX concentrate
-
-
Drugs (i.e., NSAIDs, Plavix, Coumadin)
-
NSAIDs, ASA, and Plavix characterized by reduced platelet function; treat with platelet transfusion
-
Coumadin inhibits formation of multiple clotting factors; reverse with Vitamin K and FFP
-
-
-
-
Management: Determine acuity and remember ABCs; ensure patient is stable and address any systemic disease or obvious associated comorbidity
-
Topical vasoconstriction (e.g., oxymetazoline) and manual pressure for minor bleeds
-
Cauterization (silver nitrate, electric, or KTP/argon laser)
-
Nasal packing can be anterior or posterior, ranging from a variety of nasal tampon devices to vaseline gauze packing
-
Anterior packing
-
Removed after 2–5 days depending on severity and etiology
-
Can be managed as an outpatient unless patient is elderly or has underlying coagulopathy which requires treatment
-
Complications: toxic shock syndrome (give anti-staphylococcal antibiotic while packing in place), sinusitis from blockage of sinus ostia, septal necrosis/perforation
-
-
Posterior packing
-
Often requires sedation due to discomfort
-
Requires inpatient stay to monitor airway; elderly or frail patients and those with underlying cardiopulmonary disease should be monitored in intensive care unit with low threshold for intubation
-
Complications: airway compromise, nasal-vagal reflex (hypotension and bradycardia), alar necrosis
-
-
-
Greater palatine foramen injection (local anesthetic 1 % lidocaine 1:100,000 epinephrine infiltrated into foramen—must aspirate prior to injection to ensure not in the vessel) helps control posterior bleeds
-
Surgical evaluation with ligation of bleeding vessel(s)
-
Internal maxillary artery (IMA): open posterior maxillary sinus wall, identify branches of IMA in pterygopalatine foramen and ligate with clips
-
Sphenopalatine artery (SPA): endoscopically dissect in a subperiosteal plane along the medial inferior maxillary wall just anterior to lammellar attachment of middle turbinate, identify SPA as it exits at crista ethmoidalis and ligate with clip or cauterize
-
Anterior/posterior ethmoid arteries (AEA/PEA): can either identify endoscopically and cauterize with bipolar cautery within the nasal cavity or perform Lynch incision and dissect periorbita off medial orbital wall; AEA located 8–12 mm from lacrimal crest, PEA 10–12 mm from AEA, and optic nerve 4–6 mm from PEA
-
-
Angiography and embolization
-
Angiography identifies site of active bleed, interventional radiologist performs embolization of specific branch or branches of external carotid
-
Complications: Blindness (more common with internal carotid branches, and embolization of these branches would only be undertaken in a life saving procedure), necrosis, stroke, facial pain, paresthesia
-
-
-
Benign Masses/Abnormalities
-
Nasopharyngeal cysts
-
Rathke’s pouch cyst or craniopharyngioma
-
Remnant of ectodermal tissue precursor of anterior pituitary gland
-
Tx = reassurance versus endoscopic marsupialization if symptomatic
-
-
Tornwaldt cyst
-
Remnant of caudal notochord
-
Tx = reassurance versus endoscopic marsupialization if symptomatic
-
-
-
Midline nasal masses
-
Arise as a result of failure of closure of anterior nasopore
-
Persistence of fonticulus frontalis (opening between nasal and frontal bones in the embryo) allows for intracranial connection to prenasal space
-
MRI = allows for assessment of intracranial extension
-
Biopsy of midline nasal mass in children contraindicated due to risk of IC extension
-
Tx = open vs. endoscopic surgical excision, depending on whether or not external nasal structures involved.
-
Glioma
-
60 % Extranasal, 30 % intranasal, 10 % combined
-
“Pinched off” glial tissue; can appear red and be confused with hemangioma
-
Symptoms = firm, nontender, noncompressible mass that does not transilluminate or change in size
-
-
Encephalocele, meningocele, meningoencephalocele
-
Herniation of meninges (meningocele), meninges + brain (meningoencephalocele), or meninges + brain + part of ventricular system (meningoencephalocytocele) through skull base defect
-
Sac of glial tissue lined with ependymal cells
-
25 % Anterior (sincipital/external versus basal/internal) and 75 % posterior, or occipital in location
-
Sincipital/external: herniation occurs anterior to crista galli between frontal and ethmoid bones, presenting as external mass over nose or glabella
-
Basal/internal (less common): herniation occurs posterior to cribriform plate, presenting as an intranasal mass
-
-
Symptoms: soft, compressible mass that transilluminates and increases in size with crying (positive Furstenberg test)
-
-
Dermoid Cyst
-
Sequestration of ectodermal and mesodermal elements anywhere along a tract extending from foramen cecum to nasal tip
-
Symptoms = Fistulous tract, nasal pit with tuft of hair
-
-
Fibro-osseous lesions (find also in Chap. 8)
-
Osteoma = most common benign sinonasal lesion
-
Frontal sinus most common
-
Gardner’s syndrome = skull osteomas, colonic polyps, and soft tissue tumors
-
-
Fibrous dysplasia
-
Two types: Monostotic (most common, 70–80 %) and polyostotic
-
McCune-Albright Syndrome = polyostotic lesions, precocious puberty, pigmented skin lesions
-
CT findings: Early = radiolucent; Late = “ground-glass” + calcifications
-
Tx = surgery only if symptomatic (debilitating pain or cosmetic deformity effecting quality of life), bisphosphonates
-
-
Ossifying fibroma
-
Solitary encapsulated slow growing monostotic tumor
-
CT findings = central lucency with eggshell rim
-
Tx = surgery
-
-
-
Sinonasal Malignancy
See Head and Neck section
Surgical Approaches
-
Endoscopic approach (Functional endoscopic sinus surgery or FESS)
-
Technique = Rigid nasal endoscopy +/− stereotactic image guidance, typical steps include medialization of middle turbinate, removal of uncinate process, maxillary antrostomy, ethmoidectomy, sphenoidotomy, and frontal recess exploration with sinosotomy as needed
-
Four lamellae encountered (anterior → posterior) = uncinate process → ethmoid bulla → vertical portion of middle turbinate basal lamella → vertical portion of superior turbinate basal lamella
-
Should be considered for any lesion or disease process (congenital, inflammatory, neoplastic, traumatic, etc.) which can be accessed endoscopically, but the rhinologic surgeon must be familiar with open approaches for lesions which are inaccessible or incompletely addressed via this approach
-
Complications = bleeding, synechiae, injury to the eye including blindness, CSF leak, nasolacrimal duct injury, brain injury
-
Specific endoscopic approaches to the frontal sinus:
-
Draf I: complete removal of the anterior ethmoid cells and uncinate process within the frontal recess leading to the frontal ostium. Obstructing frontal cells, if present, are removed. The frontal sinus ostium may then drain into a patent frontal recess, but the frontal sinus ostium itself is not instrumented.
-
Draf IIa: resecting all included in Draf I with the addition of widening the frontal sinus ostium itself, resecting all of the frontal sinus floor from lamina to the insertion of the middle turbinate medially
-
Draf IIb: resecting all included in Draf IIa with the addition of resecting the middle turbinate up to skull base and widening the frontal sinus medially to the septum
-
Draf III (aka Modified Lothrop): resecting all included in Draf II, with the addition of removing the intersinus septum and connecting bilateral frontal sinuses into one horseshoe-shaped sinus with a common drainage pathway
-
-
Open Approaches
-
Caldwell Luc
-
Used most often to gain access to the anterior wall of the maxillary sinus
-
Performed through canine fossa with incision at gingivobuccal sulcus
-
Can augment endoscopic surgery; good for anteriorly attached IP or other tumors, broader access to orbital floor and PPF
-
Complications = cheek edema/ecchymosis, numbness or pain with infraorbital nerve injury, oroantral fistula, epiphora if damage to nasolacrimal duct
-
-
External ethmoidectomy
-
Provides access to ethmoid cavity, medial orbit, cribriform plate, and frontonasal area if endoscopy is not an option; can be employed to decompress subperiosteal abscess
-
Complications = eye injury including blindness and corneal abrasions, CSF leak, skull base injury, bleeding from AEA +/− retraction of vessel into eye
-
-
External frontoethmoidectomy (Lynch procedure) or frontal trephine
-
Indications: uncommonly used now, when endoscopic approach is for any reason insufficient to address frontoethmoid mucocele, mucopyocele, rhinosinusitis with orbital complications, frontoethmoid or anterior skull base tumor, CSF leak repair, acute sinusitis with intracranial or orbital complications or not responsive to medical management and unable to access endoscopically, lateral frontal mucocele
-
Complications = bleeding, epiphora, frontal sinusitis, diplopia, blindness, CSF leak, intracranial hemorrhage
-
-
Osteoplastic flap with frontal sinus obliteration or cranialization
-
Indications = when endoscopic approaches are insufficient or have failed to address osteomyelitis, frontal sinus tumor, recurrent persistent frontal sinusitis, trauma with comminuted anterior or posterior table fractures
-
-
Open approaches to sphenoid sinus (historically used by neurosurgeons in pituitary surgery)
-
Transseptal: incision can be endonasal, sublabial, or transcolumellar
-
-
Transfacial incisions
-
Lateral rhinotomy (incision made in naso-facial crease for small lesions of nasal cavity and medial maxilla), historically used for IP, no longer “gold standard”
-
Weber-Ferguson (incision for lateral rhinotomy extended laterally in subciliary crease and inferiorly along philtrum through vermilion border to split lip, provides wide access for most sinonasal tumors)
-
-
Craniofacial resection
-
Bifrontal craniotomy with transfacial exposure of sinonasal cavity and orbits, allows for access to anterior cranial fossa
-
Used to approach skull base pathology including malignancy that cannot, for whatever reason, be accessed via the endoscopic approach
-
Major Complications of Sinus Surgery
-
Orbital
-
Includes blindness (direct injury or hematoma), penetration of orbit (may see fat herniation), diplopia (muscle injury), and epiphora (damage to lacrimal system)
-
Retrobulbar hematoma is an acute complication which must be recognized immediately and treated to avoid blindness
-
Cause = most commonly from venous injury near lamina papyracea or arterial injury to AEA during endoscopic surgery → retraction of vessel into orbit where pressure from hematoma compresses optic nerve
-
Sx = proptosis, chemosis, ecchymosis, vision change (if awake)
-
Treatment = immediate ophthalmology consult, ice packs, mannitol, remove any nasal packing if it has been placed, surgical intervention (lateral canthotomy, +/− medial orbital wall decompression)
-
Prevention = keep eyes visible during surgery and evaluate any imaging preoperatively to identify AEAs which run below skull base
-
-
-
CSF leak
-
If identified at the time of surgery the defect should be repaired at that time (most common site of iatrogenic injury = lateral lamella of ethmoid roof)
-
If identified postoperatively (beta-2 transferrin positive thin watery rhinorrhea) can try conservative management first, although many surgeons would opt to go straight to surgery for repair
-
Conservative treatment = 7–10 days of bed rest, head elevation, stool softeners to avoid straining, lumbar drain for diversion (+/− antibiotics (prophylaxis for meningitis), no evidence to support use however most continue to use)
-
Surgical repair
-
Intracranial approach (50–70 % success rate) requires a coronal approach and carries risks of frontal lobe dysfunction, cerebral edema, seizures, and anosmia
-
Extracranial approach (80 % success rate) uses transfacial incisions, providing better visualization of the site of CSF leak but resulting in facial scarring
-
Endoscopic endonasal approach (95 % success rate) has the least morbidity
-
Overlay versus underlay repair (similar results) or both, using pedicled or free mucosal graft, pericranial flap, fat/fascia, synthetic dura are all options, with tissue glue/nasal packing per surgeon preference
-
Pedicled nasoseptal flaps when performing an endoscopic repair have dramatically reduced rate of recurrent CSF leak in the literature
-
-
-
References
Bland KI, Csendes A, et al. General surgery: principles and international practice, vol. 1. London: Springer; 2009.
Bradley P, Jones N, Robertson I. Diagnosis and management of esthesioneuroblastoma. Curr Opin Otolaryngol Head Neck Surg. 2003;11:112–8.
Bailey BJ, editor. Head and neck surgery-otolaryngology. Philadelphia, PA: J.B. Lippincott Co.; 1993.
Chandra RK, Pearlman A, Conley DB, et al. Significance of osteomeatal complex obstruction. J Otolaryngol Head Neck Surg. 2010;39(2):171–4.
Cummings C, editor. Otolaryngology-head and neck surgery. St. Louis, MO: Mosby-Year Book, Inc.; 1993.
Devaiah A, Larsen C, Tawfik O, et al. Esthesioneuroblastoma: endoscopic nasal and anterior craniotomy resection. Laryngoscope. 2003;113(12):2086–90.
Ercan I, Cakir BO, Sayin I, et al. Relationship between the superior attachment type of uncinate process and presence of agger nasi cell: a computer-assisted anatomic study. Otolaryngol Head Neck Surg. 2006;134:1010–4.
Fokkens WJ, Lund VJ, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1):1–12.
Hegazy H, Carrau R, Snyderman C. Transnasal endoscopic repair of cerebrospinal fluid rhinorrhea: a meta-analysis. Laryngoscope. 2000;110(7):1166–72.
Holbrook E. Anosmia: diagnosis and management. Curr Opin Otolaryngol Head Neck Surg. 2003;11:54–60.
Knipping S, Holzhausen HJ, Koesling S, Bloching M. Invasive aspergillosis of the paranasal sinuses and the skull base. Eur Arch Otorhinolaryngol. 2007;264(10):1163–9.
Kraft M, Simmen D, Kaufmann T, et al. Long-term results of endonasal sinus surgery in sinonasal papillomas. Laryngoscope. 2003;113(9):1541–7.
Krouse JH. Allergy and chronic rhinosinusitis. Otolaryngol Clin North Am. 2005;38(6):1257–66.
Kupferberg SB, Bent JP, Kuhn FA. Prognosis for allergic fungal sinusitis. Otolaryngol Head Neck Surg. 1997;117(1):35–41.
Landsberg R, Friedman M. A computer-assisted anatomical study of the nasofrontal region. Laryngoscope. 2001;111:2125–30.
Lanza D, O’Brien D, Kennedy D. Endoscopic repair of cerebrospinal fluid fistulae and encephaloceles. Laryngoscope. 1996;106(9):1119–25.
Lee S, Lane AP. Chronic rhinosinusitis as a multifactorial inflammatory disorder. Curr Infect Dis Rep. 2011;8(1):132–40.
Lindstrom R, Toohill R, Loehrl T. Management of cerebrospinal fluid rhinorrhea: the medical college of Wisconsin experience. Laryngoscope. 2004;114(6):969–74.
Lowe LH, Booth TN, Joglar JM, Rollins NK. Midface anomalies in children. Radiographics. 2000;20:907–22.
McGarry GW. Relation between alcohol and nosebleeds. BMJ. 1994;309:640.
Myers E, Suen J. Neoplasms of the nose and paranasal sinuses. In: cancer of the head and neck. 3rd ed. Philadelphia, PA: W.B. Saunders Company; 1996.
Myers L, Nussenbaum B, Bradford C, et al. Paranasal sinus malignancies: an 18-year single institution experience. Laryngoscope. 2002;112(11):1964–9.
Poetker DM, Smith TL. Adult chronic rhinosinusitis: surgical outcomes and the role of endoscopic sinus surgery. Curr Opin Otolaryngol Head Neck Surg. 2007;15(1):6–9.
Ramadan HH, Sanclement JA, Thomas JG. Chronic rhinosinusitis and biofilms. Otolaryngol Head Neck Surg. 2005;132:414–7.
Rogers GM, Melicher Larson J, Carter KD. Invasive Fungal Orbitorhinocerebral Mucormycosis. 2010. http://www.EyeRounds.org/cases/108-Orbitorhinocerebral-Mucormycosis.htm. Accessed 16 Feb 2010
Ruiz JW, Saint-Victor S, Tessema B, Eloy JA, Anstead A. Coblation assisted endoscopic juvenile nasopharyngeal angiofibroma resection. International Journal of Ped Otorhinolaryngol. 2012;76(3):439–42.
Scadding GK. Non-allergic rhinitis: diagnosis and management. Curr Opin Allergy Clin Immunol. 2001;1:15–20.
Scadding GK. Medical management of chronic rhinosinusitis. Immunol Allergy Clin North Am. 2004;24(1):103–18.
Settipane RA, Lieberman P. Update on non-allergic rhinitis. Ann Allergy Asthma Immunol. 2001;86:494.
Stammberger HR, Kennedy DW. Paranasal sinuses: anatomic terminology and nomenclature. Anatomic terminology group. Ann Otol Rhinol Laryngol Suppl. 1995;167:7–16.
Stucker FJ, Souza C, et al., editors. Rhinology and facial plastic surgery. Berlin: Springer; 2009.
Welsh LW, Welsh JJ, Scogna JE, Gregor FA. Role of angiography in the management of refractory epistaxis. Ann Otol Rhinol Laryngol. 1990;99:69–73.
Winstead W. Sphenopalatine arterial ligation: an alternative to internal maxillary artery ligation for intractable posterior epistaxis. Laryngoscope. 1996;106:667–9.
Wurman LH, Sack JG, Flannery JV, Lipsman RA. The management of epistaxis. Am J Otolaryngol. 1992;13(4):193–209.
Zhang L, Han D, Ge W, et al. Anatomical and computed tomographic analysis of the interaction between the uncinate process and the agger nasi cell. Acta Otolaryngol. 2006;126:845–52.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Hayes, K., Patel, Z.M. (2014). Rhinology. In: Lin, F., Patel, Z. (eds) ENT Board Prep. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8354-0_6
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8354-0_6
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8353-3
Online ISBN: 978-1-4614-8354-0
eBook Packages: MedicineMedicine (R0)