
Abstract
Background
Needle aponeurotomy and collagenase injection are alternative treatments of Dupuytren’s contracture to open partial fasciectomy; however, reported data are difficult to interpret without a formal systematic review.
Methods
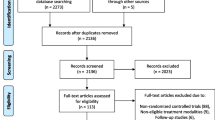
A Medline, EMBASE, and Cochrane database search was performed, and 277 articles were identified. Articles were stratified by level of evidence, and those of the highest level for each technique were included. Evidence available for needle aponeurotomy was of low quality so only cohorts larger than 100 patients were included.
Results
The sample size of patients for open partial fasciectomy ranged from 37–261. The recurrence rate ranged from 12–39%, with mean follow-up time of 1.5–7.3 years. The complication rate ranged from 14–67%. Complications included nerve division (2–5%), infection (4–12%), neurapraxia (0.4–52%), and regional pain syndrome (2–13%). For needle aponeurotomy the sample size ranged from 117–211. The recurrence rate ranged from 50–58%, with mean follow-up time of 3–5 years. With regard to collagenase injection, the sample size ranged from 13–204. The recurrence rate ranged from 10–31%, with mean follow-up time of 120 days to 4 years. For the two latter procedures, adverse effects consisted primarily of skin tears (9–25%). Kruskal–Wallis testing demonstrated that the recurrence rate was significantly higher for needle aponeurotomy than for open partial fasciectomy (p = 0.001), and the recurrence rate was significantly higher for open partial fasciectomy than for collagenase injection (p = 0.001).
Conclusions
The recurrence rates and types of complications differ between open partial fasciectomy and needle aponeurotomy or collagenase injection. Long-term outcomes have not been well reported.

Similar content being viewed by others

References
Badalamente MA, Hurst LC. Enzyme injection as nonsurgical treatment of Dupuytren's disease. J Hand Surg Am. 2000;25:629–36.
Badalamente MA, Hurst LC. Efficacy and safety of injectable mixed collagenase subtypes in the treatment of Dupuytren's contracture. J Hand Surg Am. 2007;32:767–74.
Badalamente MA, Hurst LC, Hentz VR. Collagen as a clinical target: nonoperative treatment of Dupuytren's disease. J Hand Surg Am. 2002;27:788–98.
Badois FJ, Lermusiaux JL, Masse C, Kuntz D. Non-surgical treatment of Dupuytren disease using needle fasciotomy. Rev Rhum Ed Fr. 1993;60:808–13.
Balaguer T, David S, Ihrai T, Cardot N, Daideri G, Lebreton E. Histological staging and Dupuytren's disease recurrence or extension after surgical treatment: a retrospective study of 124 patients. J Hand Surg Eur. 2009;34:493–6.
Becker GW, Davis TR. The outcome of surgical treatments for primary Dupuytren's disease—a systematic review. J Hand Surg Eur. 2010;35:623–6.
Bulstrode NW, Jemec B, Smith PJ. The complications of Dupuytren's contracture surgery. J Hand Surg Am. 2005;30:1021–5.
Citron ND, Nunez V. Recurrence after surgery for Dupuytren's disease: a randomized trial of two skin incisions. J Hand Surg Br. 2005;30:563–6.
Coert JH, Nerin JP, Meek MF. Results of partial fasciectomy for Dupuytren disease in 261 consecutive patients. Ann Plast Surg. 2006;57:13–7.
Foucher G, Medina J, Navarro R. Percutaneous needle aponeurotomy: complications and results. J Hand Surg Br. 2003;28:427–31.
Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase Clostridium histolyticum for Dupuytren's contracture. N Engl J Med. 2009;361:968–79.
Misra A, Jain A, Ghazanfar R, Johnston T, Nanchahal J. Predicting the outcome of surgery for the proximal interphalangeal joint in Dupuytren's disease. J Hand Surg Am. 2007;32:240–5.
Mushlin AI, Ghomrawi H. Health care reform and the need for comparative-effectiveness research. N Engl J Med. 2010;362:e6.
Rombouts JJ, Noel H, Legrain Y, Munting E. Prediction of recurrence in the treatment of Dupuytren's disease: evaluation of a histologic classification. J Hand Surg Am. 1989;14:644–52.
Roush TF, Stern PJ. Results following surgery for recurrent Dupuytren's disease. J Hand Surg Am. 2000;25:291–6.
Ullah AS, Dias JJ, Bhowal B. Does a 'firebreak' full-thickness skin graft prevent recurrence after surgery for Dupuytren's contracture?: a prospective, randomised trial. J Bone Joint Surg Br. 2009;91:374–8.
van Rijssen AL, Gerbrandy FS, Ter Linden H, Klip H, Werker PM. A comparison of the direct outcomes of percutaneous needle fasciotomy and limited fasciectomy for Dupuytren's disease: a 6-week follow-up study. J Hand Surg Am. 2006;31:717–25.
Watt AJ, Curtin CM, Hentz VR. Collagenase injection as nonsurgical treatment of Dupuytren's disease: 8-year follow-up. J Hand Surg Am. 2010;35:534–9. 9.e1.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Chen, N.C., Srinivasan, R.C., Shauver, M.J. et al. A systematic review of outcomes of fasciotomy, aponeurotomy, and collagenase treatments for Dupuytren’s contracture. HAND 6, 250–255 (2011). https://doi.org/10.1007/s11552-011-9326-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11552-011-9326-8