
Abstract
Purpose
Aromatase inhibitors (AI), which decrease circulating estradiol concentrations in post-menopausal women, are associated with toxicities that limit adherence. Approximately one-third of patients will tolerate a different AI after not tolerating the first. We report the effect of crossover from exemestane to letrozole or vice versa on patient-reported outcomes (PROs) and whether the success of crossover is due to lack of estrogen suppression.
Methods
Post-menopausal women enrolled on a prospective trial initiating AI therapy for early-stage breast cancer were randomized to exemestane or letrozole. Those that discontinued for intolerance were offered protocol-directed crossover to the other AI after a washout period. Changes in PROs, including pain [Visual Analog Scale (VAS)] and functional status [Health Assessment Questionnaire (HAQ)], were compared after 3 months on the first versus the second AI. Estradiol and drug concentrations were measured.
Results
Eighty-three patients participated in the crossover protocol, of whom 91.3% reported improvement in symptoms prior to starting the second AI. Functional status worsened less after 3 months with the second AI (HAQ mean change AI #1: 0.2 [SD 0.41] vs. AI #2: −0.05 [SD 0.36]; p = 0.001); change in pain scores was similar between the first and second AI (VAS mean change AI #1: 0.8 [SD 2.7] vs. AI #2: −0.2 [SD 2.8]; p = 0.19). No statistical differences in estradiol or drug concentrations were found between those that continued or discontinued AI after crossover.
Conclusions
Although all AIs act via the same mechanism, a subset of patients intolerant to one AI report improved PROs with a different one. The mechanism of this tolerance remains unknown, but does not appear to be due to non-adherence to, or insufficient estrogen suppression by, the second AI.



Similar content being viewed by others


References
Johnston SRD, Dowsett M (2003) Aromatase inhibitors for breast cancer: lessons from the laboratory. Nat Rev Cancer 3:821–831. doi:10.1038/nrc1211
Rugo HS, Rumble RB, Macrae E et al (2016) Endocrine therapy for hormone receptor-positive metastatic breast cancer: American Society of Clinical Oncology guideline. J Clin Oncol 34:3069–3103. doi:10.1200/JCO.2016.67.1487
Burstein HJ, Lacchetti C, Anderson H et al (2016) Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology clinical practice guideline update on ovarian suppression. J Clin Oncol 34:1689–1701. doi:10.1200/JCO.2015.65.9573
Henry NL, Azzouz F, Desta Z et al (2012) Predictors of aromatase inhibitor discontinuation as a result of treatment-emergent symptoms in early-stage breast cancer. J Clin Oncol 30:936–942. doi:10.1200/JCO.2011.38.0261
Crew KD, Greenlee H, Capodice J et al (2007) Prevalence of joint symptoms in postmenopausal women taking aromatase inhibitors for early-stage breast cancer. J Clin Oncol 25:3877–3883. doi:10.1200/JCO.2007.10.7573
Makubate B, Donnan PT, Dewar JA et al (2013) Cohort study of adherence to adjuvant endocrine therapy, breast cancer recurrence and mortality. Br J Cancer 108:1515–1524. doi:10.1038/bjc.2013.116
Yardley D, Green NB, Papish S, et al (2009) Rheumatologic Evaluation of Adjuvant Letrozole in Post-Menopausal Breast Cancer Patients Discontinuing Anastrozole Due to Grade 2-3 Arthralgia—Myalgia. In: San Antonio Breast Cancer Symp. p Cancer Res 2009;69(24 Suppl):Abstract nr 805
Renshaw L, McHugh R, Williams L (2007) Comparison of joint problems reported by patients in a randomized adjuvant trial of anastrozole and letrozole. In: Breast Can Res Treat. p 106(Suppl 1):S108–S109. Abstract 2072
Henry NL, Chan H-P, Dantzer J et al (2013) Aromatase inhibitor-induced modulation of breast density: clinical and genetic effects. Br J Cancer 109:2331–2339. doi:10.1038/bjc.2013.587
Santen RJ, Demers L, Ohorodnik S et al (2007) Superiority of gas chromatography/tandem mass spectrometry assay (GC/MS/MS) for estradiol for monitoring of aromatase inhibitor therapy. Steroids 72:666–671. doi:10.1016/j.steroids.2007.05.003
Hertz DL, Kidwell KM, Seewald NJ et al (2016) Polymorphisms in drug-metabolizing enzymes and steady-state exemestane concentration in postmenopausal patients with breast cancer. Pharmacogenomics J. doi:10.1038/tpj.2016.60
Robarge JD, Desta Z, Nguyen AT et al (2017) Effects of exemestane and letrozole therapy on plasma concentrations of estrogens in a randomized trial of postmenopausal women with breast cancer. Breast Cancer Res Treat 161:453–461. doi:10.1007/s10549-016-4077-4
Desta Z, Kreutz Y, Nguyen AT et al (2011) Plasma letrozole concentrations in postmenopausal women with breast cancer are associated with CYP2A6 genetic variants, body mass index, and age. Clin Pharmacol Ther 90:693–700. doi:10.1038/clpt.2011.174
Bruce B, Fries JF (2003) The Stanford Health Assessment Questionnaire: a review of its history, issues, progress, and documentation. J Rheumatol 30:167–178
Pickard AS, Wilke CT, Lin H-W, Lloyd A (2007) Health utilities using the EQ-5D in studies of cancer. Pharmacoeconomics 25:365–384
Carpenter JS, Andrykowski MA, Wilson J, et al Psychometrics for two short forms of the center for epidemiologic studies-depression scale. Issues Ment Health Nurs 19:481–94
Stafford L, Judd F, Gibson P et al (2014) Comparison of the hospital anxiety and depression scale and the center for epidemiological studies depression scale for detecting depression in women with breast or gynecologic cancer. Gen Hosp Psychiatry 36:74–80. doi:10.1016/j.genhosppsych.2013.08.010
Ganz PA, Day R, Ware JE et al (1995) Base-line quality-of-life assessment in the National Surgical Adjuvant Breast and Bowel Project Breast Cancer Prevention Trial. J Natl Cancer Inst 87:1372–1382
Farrar JT, Pritchett YL, Robinson M et al (2010) The clinical importance of changes in the 0 to 10 numeric rating scale for worst, least, and average pain intensity: analyses of data from clinical trials of duloxetine in pain disorders. J Pain 11:109–118. doi:10.1016/j.jpain.2009.06.007
Wolfe F, Michaud K, Strand V (2005) Expanding the definition of clinical differences: from minimally clinically important differences to really important differences. Analyses in 8931 patients with rheumatoid arthritis. J Rheumatol 32:583–589
Kadakia KC, Snyder CF, Kidwell KM et al (2016) Patient-reported outcomes and early discontinuation in aromatase inhibitor-treated postmenopausal women with early stage breast cancer. Oncologist. doi:10.1634/theoncologist.2015-0349
Henry NL, Skaar TC, Dantzer J et al (2013) Genetic associations with toxicity-related discontinuation of aromatase inhibitor therapy for breast cancer. Breast Cancer Res Treat 138:807–816. doi:10.1007/s10549-013-2504-3
Briot K, Tubiana-Hulin M, Bastit L et al (2010) Effect of a switch of aromatase inhibitors on musculoskeletal symptoms in postmenopausal women with hormone-receptor-positive breast cancer: the ATOLL (articular tolerance of letrozole) study. Breast Cancer Res Treat 120:127–134. doi:10.1007/s10549-009-0692-7
Duric VM, Fallowfield LJ, Saunders C et al (2005) Patients’ preferences for adjuvant endocrine therapy in early breast cancer: what makes it worthwhile? Br J Cancer 93:1319–1323. doi:10.1038/sj.bjc.6602874
Ravdin PM, Siminoff IA, Harvey JA (1998) Survey of breast cancer patients concerning their knowledge and expectations of adjuvant therapy. J Clin Oncol 16:515–521
Acknowledgements
This study was supported in part by U01-GM61373 and 5T32-GM08425 (DAF), M01-RR00042 (UM), M01-RR00750 (IU), and M01-RR00052 (JHU). NJS was supported (in part) by Cancer Center Biostatistics Training Grant 5T32-CA083654 (to J. Taylor). NLH was a Damon Runyon-Lilly Clinical Investigator supported (in part) by the Damon Runyon Cancer Research Foundation (Grant number CI-53-10) and by an American Cancer Society Research Scholar Grant. Additional support was provided by Fashion Footwear Association of New York/QVC Presents Shoes on Sale (DFH). In addition, the ELPh trial was supported by grants from Pfizer, Inc. and Novartis Pharma AG, who provided study medication.
Funding
Abbvie, Merck, Pfizer, MedImmune, Celgene, Puma Biotechnology, and Novartis (VS); Pfizer and Novartis (AMS); AstraZeneca, Janssen Research and Development, Puma Biotechnology, Pfizer, Eli Lilly Company (DFH); WellPoint and Genentech (CFS).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Employment or Leadership Position: None, Consultant or Advisory Role: Walgreens and Pfizer (CFS); Pfizer (DFH), Stock Ownership: Immunomedics (CFS) Oncoimmune and InBiomotion (DFH), Honoraria: Pfizer (AMS); Lilly (DFH), All other authors had no conflicts of interest to disclose.
Additional information
David A. Flockhart was Deceased.
Electronic supplementary material
Below is the link to the electronic supplementary material.
10549_2017_4260_MOESM1_ESM.docx
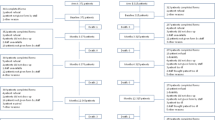
Supplementary material 1 (DOCX 73 kb) Online Supplement 1—Diagram of the primary patient reported outcome analysis. PRO patient reported outcomes, AI aromatase inhibitor; Δ change
Rights and permissions
About this article

Cite this article
Kadakia, K.C., Kidwell, K.M., Seewald, N.J. et al. Prospective assessment of patient-reported outcomes and estradiol and drug concentrations in patients experiencing toxicity from adjuvant aromatase inhibitors. Breast Cancer Res Treat 164, 411–419 (2017). https://doi.org/10.1007/s10549-017-4260-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-017-4260-2