
Abstract
Aims
Late in-stent restenosis (ISR) has become increasingly important, in particular due to neo-atherosclerosis. CCTA is a highly sensitive method for detecting coronary plaques. Its diagnostic accuracy regarding ISR is controversial. Stent artifacts can impede image quality, but recent developments in CT-technology may help to overcome some of these problems and allow for improved diagnostic accuracy.
Methods
Consecutive patients after previous coronary revascularization who had stable symptoms or signs of possible disease progression were examined using a third-generation dual-source CT scanner. After the scan, patients were followed for clinical events (MACE) over a mean of 399 days. Patients with high-grade stenoses were referred for invasive coronary angiography (ICA), unclear findings were further evaluated either by ICA or functional testing.
Results
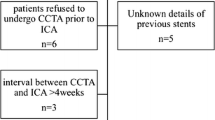
Overall, 226 patients were included. A total of 457 stents were evaluated (2.0 ± 1.4 per patient). Mean stent diameter was 2.9 ± 0.45 mm. In 61%, a high-pitch protocol was employed. Mean dose-length product (DLP) of CCTA was 159.2 mGy cm, corresponding to 2.2 mSv using a conversion factor of k = 0.014. Mean amount of contrast agent was 58.3 ± 12.5 ml. In 145 patients (64%), CCTA was negative. In this group, one MACE occurred (acute coronary syndrome) during follow-up in a patient who had also undergone unremarkable ICA. In 23 patients (10%), CCTA detected 28 ISR which were confirmed and treated by ICA (true positive). In 27 patients (12%), ISR was suspected by CCTA but excluded by ICA (false positive), 30 patients (13%) had unclear findings and normal non-invasive tests. No MACE occurred during follow-up in these patients. One patient was misclassified in CCTA as having intermediate and not high-grade ISR who underwent revascularization within 3 months. Eleven patients (5%) were lost to follow-up. During follow-up, eight patients had myocardial infarctions due to five ISRs and three de novo lesions. No patient died. In cases with unclear or false-positive findings, the amount of stents was significantly higher, stents were smaller and patients had a higher BMI.
Conclusion
In almost two-thirds of symptomatic patients with previous coronary stent implantation, ISR could be ruled out by CCTA. 10% of patients had definite ISR. The rate of false-negative findings was low (< 1%), whereas the rate of false positive or inconclusive findings was 25%, leading to invasive rule-out of ISR by ICA in 12%. CCTA appears valuable as a tool for safely excluding ISR. It might help to avoid invasive diagnostic procedures. Further analyses are warranted, in particular regarding the influence of stent dimensions and the total amount of stents in a patient.





Similar content being viewed by others

References
Park S-J, Kang S-J, Virmani R, Nakano M, Ueda Y (2012) In-stent neoatherosclerosis: a final common pathway of late stent failure. J Am Coll Cardiol 59(23):2051–2057
Palmerini T, Biondi-Zoccai G, Della Riva D, Stettler C, Sangiorgi D, D’Ascenzo F et al (2012) Stent thrombosis with drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. Lancet Lond Engl 379(9824):1393–1402
Smits PC, Vlachojannis GJ, McFadden EP, Royaards K-J, Wassing J, Joesoef KS et al (2015) Final 5-year follow-up of a randomized controlled trial of everolimus- and paclitaxel-eluting stents for coronary revascularization in daily practice: the COMPARE Trial (A Trial of Everolimus-Eluting Stents and Paclitaxel Stents for Coronary Revascularization in Daily Practice). JACC Cardiovasc Interv 8(9):1157–1165
Otsuka F, Byrne RA, Yahagi K, Mori H, Ladich E, Fowler DR et al (2015) Neoatherosclerosis: overview of histopathologic findings and implications for intravascular imaging assessment. Eur Heart J 36(32):2147–2159
Byrne RA, Serruys PW, Baumbach A, Escaned J, Fajadet J, James S et al (2015) Report of a European Society of Cardiology-European Association of Percutaneous Cardiovascular Interventions task force on the evaluation of coronary stents in Europe: executive summary. Eur Heart J 36(38):2608–2620
Members TF, Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C et al (2013) 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 34(38):2949–3003
Andreini D, Pontone G, Bartorelli AL, Trabattoni D, Mushtaq S, Bertella E et al (2009) Comparison of feasibility and diagnostic accuracy of 64-slice multidetector computed tomographic coronary angiography versus invasive coronary angiography versus intravascular ultrasound for evaluation of in-stent restenosis. Am J Cardiol 103(10):1349–1358
Cademartiri F, Schuijf JD, Pugliese F, Mollet NR, Jukema JW, Maffei E et al (2007) Usefulness of 64-slice multislice computed tomography coronary angiography to assess in-stent restenosis. J Am Coll Cardiol 49(22):2204–2210
Ehara M, Kawai M, Surmely J-F, Matsubara T, Terashima M, Tsuchikane E et al (2007) Diagnostic accuracy of coronary in-stent restenosis using 64-slice computed tomography: comparison with invasive coronary angiography. J Am Coll Cardiol 49(9):951–959
Kumbhani DJ, Ingelmo CP, Schoenhagen P, Curtin RJ, Flamm SD, Desai MY (2009) Meta-analysis of diagnostic efficacy of 64-slice computed tomography in the evaluation of coronary in-stent restenosis. Am J Cardiol 103(12):1675–1681
Rixe J, Achenbach S, Ropers D, Baum U, Kuettner A, Ropers U et al (2006) Assessment of coronary artery stent restenosis by 64-slice multi-detector computed tomography. Eur Heart J 27(21):2567–2572
Sun Z, Almutairi AMD (2010) Diagnostic accuracy of 64 multislice CT angiography in the assessment of coronary in-stent restenosis: a meta-analysis. Eur J Radiol 73(2):266–273
Eisentopf J, Achenbach S, Ulzheimer S, Layritz C, Wuest W, May M et al (2013) Low-dose dual-source CT angiography with iterative reconstruction for coronary artery stent evaluation. JACC Cardiovasc Imaging 6(4):458–465
Pugliese F, Weustink AC, Van Mieghem C, Alberghina F, Otsuka M, Meijboom WB et al (2008) Dual source coronary computed tomography angiography for detecting in-stent restenosis. Heart Br Card Soc 94(7):848–854
Wuest W, May MS, Scharf M, Layritz C, Eisentopf J, Ropers D et al (2013) Stent evaluation in low-dose coronary CT angiography: effect of different iterative reconstruction settings. J Cardiovasc Comput Tomogr 7(5):319–325
Ochs MM, Siepen FAD, Fritz T, Andre F, Gitsioudis G, Korosoglou G et al (2017) Limits of the possible: diagnostic image quality in coronary angiography with third-generation dual-source CT. Clin Res Cardiol 106(7):485–492
Schmermund A, Marwan M, Hausleiter J, Barth S, Bruder O, Kerber S et al (2017) Declining radiation dose of coronary computed tomography angiography: German cardiac CT registry experience 2009–2014. Clin Res Cardiol Off J Ger Card Soc 106(11):905–912
Taniwaki M, Windecker S, Zaugg S, Stefanini GG, Baumgartner S, Zanchin T et al (2015) The association between in-stent neoatherosclerosis and native coronary artery disease progression: a long-term angiographic and optical coherence tomography cohort study. Eur Heart J 36(32):2167–2176
Gassenmaier T, Petri N, Allmendinger T, Flohr T, Maintz D, Voelker W et al (2014) Next generation coronary CT angiography: in vitro evaluation of 27 coronary stents. Eur Radiol 24(11):2953–2961
Amanuma M, Kondo T, Sano T, Takayanagi T, Matsutani H, Sekine T et al (2016) Assessment of coronary in-stent restenosis: value of subtraction coronary computed tomography angiography. Int J Cardiovasc Imaging 32(4):661–670
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest of any of the contributing authors.
Rights and permissions
About this article

Cite this article
Eckert, J., Renczes-Janetzko, P., Schmidt, M. et al. Coronary CT angiography (CCTA) using third-generation dual-source CT for ruling out in-stent restenosis. Clin Res Cardiol 108, 402–410 (2019). https://doi.org/10.1007/s00392-018-1369-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-018-1369-1