
Abstract
Background
There is a paucity of literature comparing laparoscopic to robotic inguinal hernia repair. We present a single surgeon’s transition from laparoscopic totally extraperitoneal (L-TEP) to robotic transabdominal preperitoneal (R-TAPP) inguinal hernia repair and compare outcomes from the two approaches.
Methods
This retrospective review and analysis of prospectively collected data compare outcomes during the transition from L-TEP to R-TAPP inguinal hernia repair by a single surgeon at one institution. Operating times and surgical outcomes and complications are analyzed. All consecutive L-TEP cases from November 2012 to August 2014 and all consecutive R-TAPP cases from March 2013 to October 2015 were included in the analysis.
Results
A total of 157 and 118 patients underwent L-TEP and R-TAPP inguinal hernia repair, respectively. The groups were similar regarding demographics and ASA class. A significantly higher number of complex cases were performed in the R-TAPP group compared to L-TEP group (n = 11 vs. n = 1, p = 0.0001). Mean surgical times were nearly identical (69.12 ± 35.13 min, R-TAPP; 69.05 ± 26.31, L-TEP) as were intraoperative and postoperative complication rates—despite the significantly higher number of complex cases in the R-TAPP group.
Conclusions
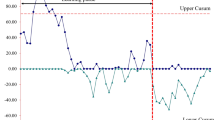
This is the largest study in the literature comparing a single surgeon’s experience transitioning from L-TEP to R-TAPP inguinal hernia repair. Results from the R-TAPP cases were similar to those achieved from laparoscopic cases. The robotic platform may have facilitated the execution of complex hernia cases during the proficiency phase.

Similar content being viewed by others


References
Bittner R, Montgomery MA, Arregui E, Bansal V et al (2015) Update of guidelines on laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia (International Endohernia Society). Surg Endosc 29(2):289–321. doi:10.1007/s00464-014-3917-8
Neumayer L, Giobbie-Hurder A, Jonasson O et al (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350(18):1819–1827. doi:10.1056/NEJMoa040093
McCormack K, Scott NW, Go PM et al (2003) Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev 1:CD001785. doi:10.1002/14651858.CD001785
Trevisonno M, Kaneva P, Watanabe Y et al (2015) A survey of general surgeons regarding laparoscopic inguinal hernia repair: practice patterns, barriers, and educational needs. Hernia 19(5):719–724. doi:10.1007/s10029-014-1287-8
Haidenberg J, Kendrick ML, Meile T et al (2003) Totally extraperitoneal (TEP) approach for inguinal hernia: the favorable learning curve for trainees. Curr Surg 60(1):65–68. doi:10.1016/S0149-7944(02)00657-8
Schouten N, Simmermacher RK, van Dalen T et al (2013) Is there an end of the “learning curve” of endoscopic totally extraperitoneal (TEP) hernia repair? Surg Endosc 27(3):789–794. doi:10.1007/s00464-012-2512-0
McCormack K, Wake B, Perez J et al (2005) Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess 9(14):1–203
Yohannes P, Rotariu P, Pinto P et al (2002) Comparison of robotic versus laparoscopic skills: is there a difference in the learning curve? Urology 60(1):39–45 discussion 45
Chandra V, Nehra D, Parent R et al (2010) A comparison of laparoscopic and robotic assisted suturing performance by experts and novices. Surgery 147(6):830–839. doi:10.1016/j.surg.2009.11.002
Schreuder HW, Wolswijk R, Zweemer RP et al (2012) Training and learning robotic surgery, time for a more structured approach: a systematic review. BJOG 119(2):137–149. doi:10.1111/j.1471-0528.2011.03139.x
Catchpole K, Perkins C, Bresee C et al (2015) Safety, efficiency and learning curves in robotic surgery: a human factors analysis. Surg Endosc. doi:10.1007/s00464-015-4671-2
Choi YY, Kim Z, Hur KY (2012) Learning curve for laparoscopic totally extraperitoneal repair of inguinal hernia. Can J Surg 55(1):33–36. doi:10.1503/cjs.019610
Escobar Dominguez JE, Ramos MG, Seetharamaiah R et al (2015) Feasibility of robotic inguinal hernia repair, a single-institution experience. Surg Endosc. doi:10.1007/s00464-015-4717-5
Satterthwaite FE (1946) An approximate distribution of estimates of variance components. Biom Bull 2:110–114
Cavazzola LT, Rosen MJ (2013) Laparoscopic versus open inguinal hernia repair. Surg Clin North Am 93(5):1269–1279. doi:10.1016/j.suc.2013.06.013
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Kudsi is a proctor and consultant for Intuitive Surgical and a consultant for Bard and Medtronic. Drs. McCarty, Paluvoi, and Mabardy have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Kudsi, O.Y., McCarty, J.C., Paluvoi, N. et al. Transition from Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair to Robotic Transabdominal Preperitoneal Inguinal Hernia Repair: A Retrospective Review of a Single Surgeon’s Experience. World J Surg 41, 2251–2257 (2017). https://doi.org/10.1007/s00268-017-3998-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-3998-3