
Abstract
Diagnostic assays implemented in microfluidic devices have developed rapidly over the past decade and are expected to become commonplace in the next few years. Hundreds of microfluidics-based approaches towards clinical diagnostics and pathogen detection have been reported with a general theme of rapid and customizable assays that are potentially cost-effective. This chapter reviews microfluidics in molecular diagnostics based on application areas with a concise review of microfluidics in general. Basic principles of microfabrication are briefly reviewed and the transition to polymer fabricated devices is discussed. Most current microfluidic diagnostic devices are designed to target a single disease, such as a given cancer or a variety of pathogens, and there will likely be a large market for these focused devices; however, the future of molecular diagnostics lies in highly multiplexed microfluidic devices that can screen for potentially hundreds of diseases simultaneously.
You have full access to this open access chapter, Download protocol PDF
Similar content being viewed by others

Key words
- Microfluidics
- Micro-total-analysis-systems
- Lab-on-a-chip
- Point-of-care devices
- Sample preparation
- MEMS
- Rapid prototyping
- Biomarker detection
- Personalized medicine
- Global health care
1 Introduction
The role of molecular diagnostics is critical in today’s global health care environment. In the developing world, 95% of deaths are due to a lack of proper diagnostics and the associated follow-on treatment of infectious diseases; i.e., acute respiratory infections (ARIs), malaria, HIV, and tuberculosis (TB) (1). Recent pandemics like the 2009 H1N1 Influenza A pandemic, have accentuated the need for tools to effectively detect and control infectious diseases. Factors like “rapid pathogen mutation rates, transformation of nonhuman pathogens into human pathogens, and recombination of nonhuman pathogen with human pathogens” have added to the challenge of managing novel infectious diseases (2). Increased global mobility has aided the rapid spread of infectious diseases from region of origin to other parts of the world as seen during the 2009 H1N1 pandemic. This mobility has highlighted the need for rapid, portable diagnostic (point-of-care [POC]) devices at ports of entry to prevent global spread of infections. Current laboratory culture methods for pathogens take a day or more to provide results (2). Clearly, methods need to be developed to aid rapid and site-relevant diagnosis of disease.
For certain other types of infections, in both the developed and developing worlds, the diagnostic tests need to be repeated periodically to measure response to therapy and monitor the disease condition. One such case is monitoring the viral load (number of viral particles per milliliter of blood) for infections like HIV (Human immunodeficiency virus) and hepatitis C. Sub-Saharan Africa is a region heavily affected by the AIDS pandemic. The lack of standard laboratory facilities and trained laboratory technicians in these regions is a serious bottleneck (3). Similar problems exist in medically underserved areas of the USA. A simple POC platform could enable increased access to treatment for patients in such low-resource settings.
In the developed world, the strategy to deal with major disease burdens such as cancer is shifting from a therapeutic to diagnostic mode (4), as the cost of treating disease falls dramatically if it is found early. Ischemic heart diseases and cerebrovascular diseases, which are the major causes of mortality in the developed world, can be targeted by effective diagnostics (1). With projected US healthcare costs of $4.4 trillion by 2018, expanding conventional expensive diagnostic solutions is not a viable option (5). Rapid, low-cost diagnostic tools that can be dispersed throughout a community for easy access, possibly even in the home, would provide substantial benefit by allowing more rapid diagnosis and monitoring of disease and infection.
Homeland security is another key sector where portable molecular biology tools are needed to detect a variety of biological agents (6). The US Departments of Health and Human Services (HHS) and Agriculture (USDA) maintains a list of biological agents and toxins defined as select agents “that have the potential to pose a severe threat to public, animal or plant health, or to animal or plant products” (7). Again, there is a need for rapid, inexpensive detection, identification, and quantification of pathogens to help reduce this threat.
Hence, there is an unmet need for simple, low-cost/cost-effective, accurate, portable/point-of-care diagnostic tools for rapid identification of disease markers and pathogens in a variety of settings. The FDA (Food & Drug Administration), definition of a “simple test” provides a benchmark for features for an ideal diagnostic tool (Table 1, (1, 8)).
There is consensus that for such an ideal diagnostic tool, microfluidics will certainly be required and will likely make up the critical components of the device (9). Microfluidics can be defined as “science and technology of systems that process or manipulate small (10–9 to 10–18 liters) amounts of fluids, using channels with dimensions of tens to hundreds of micrometers” (10). Lab-on-a-chip (LOC) refers to the application of microfluidics in chemical, biological analysis and diagnostics. The ultimate objective of LOC devices is to integrate the entire gamut of laboratory capabilities on a microfluidic chip (11–13).
Some of the features of microfluidics that make the technology attractive for lab-on-a-chip point-of-care applications are:
-
The availability of fabrication methods to manufacture small hand-held devices on a large scale at a lower cost.
-
The ability to manipulate small volumes of sample, requiring lower amounts of reagents.
-
The ability to analyze small volumes for applications like single-cell analysis, multiplexed analysis, or forensic trace analysis (14).
-
Smaller length scales result in faster analyses and higher separation efficiencies, reducing response times. The high speed analysis also makes microfluidics a suitable candidate for high-throughput applications.
-
Straightforward integration of multiple components/functionalities (sample preparation, detection, data processing) on a single device.
-
Potentially fully automated and simple to use, enabling use by laypeople.
-
Portability and a small footprint should allow field and clinic use, as well as possibly allowing more widespread diagnostics. Pervasive diagnostics should greatly increase the likelihood of personalized medicine having a significant impact on society.
-
Highly parallel analyses will allow multiple tests to be run simultaneously, either on the same sample or multiple samples. Microfluidic devices can in principle be used to obtain parameters like proteomic, metabolomic, and genetic data of each individual for personalized care (15).
Figure 1 provides a basic generalized schematic of a microfluidic LOC device with sample-in/readout capabilities. The figure shows some of the various technologies that might be involved in sample preparation, analysis or separation, and detection. Figure 2 is an example of a real nucleotide analysis system developed at the State of Utah Center of Excellence for Biomedical Microfluidics.

A schematic diagram of a conceptual lab-on-a-chip device designed to perform a variety of unit operations and unit processing steps including: sample preparation (e.g., fluid handling, derivatization, lysis of cells, concentration, extraction, and amplification), sample separation (e.g., electrophoresis, liquid chromatography, molecular exclusion, field-flow fractionation), and detection (e.g., fluorescence, UV/Vis absorption, amperometric, conductivity, Raman, electrochemical).

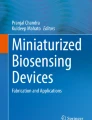
(a) Prototype of an automated nucleotide extraction platform. The microfluidic system consists of five different components: (i) a disposable microfluidic cartridge containing a glass fiber filter (inset figure); (ii) a PDMS-microfluidic chip for flow control; (iii) microfluidic chambers for mixing, metering, pumping, and reactions; (iv) a pneumatic micropump to deliver the eluted sample to downstream assays; and (v) a vacuum pump to control the on-chip valves. The extraction chip also has provision for thermal lysis and reverse transcription (not shown). (b) Prototype of a test socket for characterization of a carbon nanotube-based electrochemical nanosensor array. The test socket provides both fluidic and electrical interface to the nanosensor chip (inset figure) that detects nucleotide hybridization. (c) Prototype of a shuttle PCR chip with three temperature zones and which is fabricated using polycarbonate lamination. The heaters and thermocouples are shown with a manifold for on-chip fluidic control. The fluidic interface for the extraction system is designed so that it can be readily connected to the downstream assays such as hybridization and PCR.
2 Early Development of Microfluidics
Microfluidic devices have been steadily developing over the past 30 years, but most of the progress related to diagnostic applications has been made in about the past 15 years (10, 16). A major driver for microfluidic development was the focus on genomics and molecular biology in the 1980s especially on microanalysis techniques like high-throughput DNA sequencing. The initial microfluidic devices were inspired by the microelectronics industry and relied on photolithography and MEMS fabrication techniques. Hence, most of the earliest microfluidic devices were fabricated in silicon and glass.
The origins of microfluidics as used in diagnostic and molecular biology applications can be traced to microanalytical tools like gas-phase chromatography (GPC), high-pressure liquid chromatography (HPLC), and capillary electrophoresis (CE) developed in the mid-1990s (16). Rapid progress was made on these tools at this time and many of the developed concepts are still in use today. A summary of some of the best examples follow: Jacobson et al. reported separation of complexed metal ions in polyacrylamide-modified channels (17) using electrophoresis. Micellar electrokinetic capillary chromatography (MECC) separation of biological samples (18) and neutral dyes (19) were reported. Wooley et al. reported ultra-high-speed DNA sequencing and separation using microfabricated capillary electrophoresis chips (20). Surface passivation of silicon-based PCR chips to obtain amplifications comparable to conventional PCR systems was accomplished (21). Koutny et al. reported a competitive immunoassay for separation and quantification of free and bound labeled antigens by capillary electrophoresis (CE) (22). Hadd et al. presented an automated enzyme assay in which nanoliter volumes of substrate, enzyme, and inhibitor were mixed using electrokinetic flow (23). Microchip-based capillary electrophoresis (CE) for separation and relative quantitation of human serum proteins was achieved (24). Some of the other separation methods like free-flow electrophoresis (FFE) (25), capillary gel electrophoresis (26) and capillary array electrophoresis (CAE) (27) were reported. These devices were primarily fabricated in silicon and glass and lead to the work on related components like micropumps, microvalves and sensors.
There are a few examples of plastic devices before 2000. Delamarche et al. used elastomeric microfluidic networks to pattern immunoglobulin with high resolution on a variety of substrates (gold, glass, polystyrene) (28). Freaney et al. developed a prototype miniaturized chemical analysis system comprising biosensors and a microdialysis interface for on-line monitoring of glucose and lactate in blood (29).
In the 1990s, to counter the threat of biological and chemical weapons, the US Defense Advanced Research Projects Agency (DARPA) supported development of “field-deployable microfluidic“ devices and was a driver for academic research in microfluidics (10). The first lab-on-a-chip emerged with the concept of a “miniaturized total analysis system” or μTAS, involving a silicon chip analyzer with sampling, sample pretreatment, separation, and detection functionalities embedded on an integrated system (30). Electroosmotic pumping was the primary actuation mode used in these early μTAS systems especially since separation was one of the objectives and pumping could be controlled using simple electronics and no moving parts (31). Seiler et al. reported amino-acid separation on chip and their detection using laser-induced fluorescence (32). Other applications involving biomolecules and cells emerged during the period. These include flow cytometry (33), DNA amplification (PCR) (34) and cellular metabolism studies (35) on a microfabricated chip.
A host of innovations in microfluidic devices came forth in the period from 1994 to 1997. These include, “reactor chambers for continuous precolumn and postcolumn labeling reactions” (36, 37), high speed efficient separations (38), on-chip static mixing (39), separation of oligonucleotides (40), DNA (41), and amino acids (42), and cell manipulation by electrical fields (43). There was also work on separation modes like synchronized cyclic capillary electrophoresis (44) and free flow electrophoresis (FFE) (45). Verpoorte et al. devised a 3D microflow manifold system incorporating electrochemical and optical detection systems (46). Seiler et al. studied current and electroosmotic fluid flows in microchannels using Kirchhoff’s law (47). Jacobson et al. developed glass microchips with octadecylsilane surface modified channels as a stationary phase for open channel chromatography (48). Feustel et al. came up with a miniaturized mass spectrometer incorporating an integrated plasma chamber for electron generation, an ionization chamber, and an array of electrodes acting as the mass separator (49). All of these systems would find their way into later diagnostic microfluidic devices.
The introduction of polymer-based soft lithography offered a cheaper alternative to silicon and glass in microfluidic device fabrication (50). Most of the exploratory research in microfluidics is currently performed on polymer-based devices primarily made of poly(dimethylsiloxane) (PDMS), a soft elastomer (10). Soft lithography techniques for microfluidic devices have been reviewed multiple times along with many of the structures and devices than can be produced (51, 52). Related polymer-based methods like microcontact printing and microtransfer molding enabled rapid fabrication of micrometer scale structures (53). Three dimensional structures were reported using a layer-by-layer structuring using microtransfer molding (54).
Other plastics, hybrid materials, and packaging techniques were soon developed, including a variety of low cost plastic prototyping and manufacturing methods for microfluidics (55, 56). Martynova et al. reported microfluidic devices fabricated in Poly-(methyl methacrylate) (PMMA) by imprinting them with an inverse three-dimensional image of the device micromachined on silicon (57). Wang et al. developed a low temperature bonding process using a sodium silicate layer as an adhesive for glass microfluidic devices. Microfluidic interconnects for connecting vertically stacked micromachined channels and to external tubing on the same plane was demonstrated by Gonzalez and co-workers (58).
Additional landmark work included Johnson et al. fabricating nanometer wide channels on silicon, SiO2, and gold substrates by exposing them to a metastable argon atom beam in the presence of dilute vapors of trimethylpentaphenyltrisiloxane (59). Lorenz et al. reported the characterization of SU-8 negative photoresist for the fabrication of high aspect-ratio structures (60). Larsson et al. fabricated 3D microstructures by conventional CD-injection molding against a silicon master produced by wet and deep reactive ion etching (DRIE) (61). Silicon micromachining methods based on DRIE, silicon fusion bonding (SFB) (62), and electron cyclotron resonance (ECR) source were reported (63). Dozens of other techniques have also been reported, but cannot all be reviewed here.
3 Modern Microfluidics Fabrication
Microfluidics was inspired by the microelectronics industry and hence most of the initial devices were fabricated in silicon using photolithography and related technologies. The success of the microelectronics and MEMS industries in manufacturing thousands of miniaturized components in parallel at very low costs was thought to be applicable to microfluidics. While this may eventually prove to be true, low cost microfluidic devices made using photolithographic techniques have proven to be the exception rather than the rule, since the numbers of identical microfluidic chips manufactured for current and foreseeable markets tend to be more in the 10,000 s −100,000 s, where batch processing does not provide sufficient cost savings. Packaging and other post processing steps like reagent introduction have also proven challenging and expensive, and consequently other manufacturing methods currently appear to be more in favor. Thus, while most of the earliest work in microfluidics was in silicon, the majority of current devices are now made in glass or a variety of plastics. Nonetheless, silicon and glass manufacturing technique are important in microfluidics, because molds for rapid and inexpensive manufacturing of plastic devices are still often made of silicon or glass.
Standard silicon and glass manufacturing techniques are based on microlithography, subtractive techniques (etching), and additive techniques (64). Microlithography involves the use of an energy beam to transfer a geometric pattern to a substrate. Depending on the type of energy beam used, these can be divided into: photolithography, electron beam lithography, X-ray lithography, and ion lithography. Photolithography involves using light to transfer a geometric pattern from a photo mask to a light sensitive chemical called photoresist. This is followed by a development process using a developer solution to create a positive or negative image of pattern onto the photoresist. Other techniques like X-ray lithography, extreme ultraviolet (UV) lithography, ion particle lithography, scanning probe lithography, and nanoimprint lithography are being increasingly used due to their capability in producing sub-100 nm structures. Of these, nanoimprint lithography, a type of embossing, is a low cost, high throughput and high resolution method that has the potential to be used for low-cost mass manufacture of micro and nanofluidic devices in a variety of materials, but especially for direct embossing of plastics (65).
Subtractive techniques involve dry and wet etching, which are primarily used with glass and silicon devices. Wet etching involves chemical removal of layers from a material and is typically used to etch silicon, silicon dioxide, silicon nitride, metals, and glass. Dry etching refers to the removal of material by bombarding it with ions. Sputtering, ion beam milling and plasma etching (reactive ion etching and deep reactive ion etching) are some of other methods used in silicon etching.
Additive technologies involve techniques to deposit films. Methods to deposit thin films include: thermal oxidation of silicon, chemical vapor deposition (CVD), and physical vapor deposition (PVD). Methods to deposit thick films usually involve a spinning or electroplating technique. These thick films are often patterned using photolithography and then used as molds for microfluidic devices. The reader can refer to the text by Madou (64) for an in-depth description of the techniques described above, as well as a description of other micromanufacturing techniques.
In the past decade, silicon and glass have been largely displaced by plastics as the ideal substrate for microfluidic devices (10). Six primary considerations have been behind this transition. First, silicon is relatively expensive compared to plastics because microfluidics tends to take up larger areas than microelectronic chips (and silicon costs are measured by area). Second, the electronic advantages of silicon are not typically required in microfluidic devices. Third, silicon is not transparent, so troubleshooting microfluidic devices during development can be difficult and optical detection techniques cannot be employed. Fourth, silicon processing typically requires processes found in expensive cleanrooms that are also relatively slow. The development of rapid and inexpensive polymer processing methods has proven compelling. Fifth, silicon is relatively brittle and is not ideal for devices that experience significant “handling.” Sixth, silicon is incompatible with the strong potentials used in electrokinetic pumping and capillary electrophoresis (CE). Silicon does have some advantages, such as well controlled surface properties, but these have not proven sufficient to drive microfluidic development.
Polymers, due to their lower cost, ease of fabrication and physical properties, are now the primary materials used in microfluidic research. Many microfluidic components, such as pumps and valves, work better when fabricated in the less rigid polymer medium as compared with silicon. The permeability of polymer to gases make it suitable for work with living mammalian cells. PDMS, an optically transparent, soft elastomer has been used for various microfluidic devices since its introduction (10). Most polymer devices are made using a molding, embossing, or casting techniques, although direct processing means, such as laser-based or knife-based manufacturing is increasing (56). Soft lithography is the technique of replicating structures from a master mold or stamp onto an elastomeric (PDMS) substrate. Fabrication using PDMS is simple and does not require expensive facilities, and prototyping can often be done in less than a day. The reader can refer to in-depth reviews of soft lithography for detailed insight into the method (51, 52). Interestingly, not many commercial products use devices fabricated in PDMS due to a gap between academic and industrial practices, although this is starting to change (66). In addition, PDMS has limited application due to its hydrophobic surface and tendency to swell in organic solvents (67). Although polymers are the preferred material for most microfluidic applications today, silicon and glass are still relied upon for building specialized devices that need chemical and thermal stability (68). In the nascent field of nanofluidics, silicon and glass are used due to their mechanical stability (10). Some of other methods that are used in microfluidic fabrication are xerography (69), laser micromachining (70) and polymer stereolithography (71).
An innovative method for creating low cost disposable microfluidic diagnostic devices (paper-based analytical devices [μPADs]) was introduced by Martinez et al. (72, 73). The fluid movement is controlled primarily by evaporation and capillary forces. Although the technology is very promising, more work needs to be done to bring forth real world μPAD applications. Recently, microfluidic devices fabricated on engineered plastics, such as cyclo-olefin copolymers (COC) (74), and photocurable perfluoropolyether (PFPE) (65) have been reported.
4 Microfluidic Diagnostics in the Past Decade
A major boom in microfluidics research has occurred in the last 10–12 years as is reflected by the number of published journal papers using the term: 26 papers were published before 1990, 341 in the 1990s, 15773 in the 2000s and 3,322 in the first 2 years of this decade. While the number of papers each year appears to be leveling off, the impact of microfluidics is likely to continue to grow. Another consequence of this large body of literature is that it becomes infeasible to cover all the important papers and developments in a chapter such as this. As most reviews on microfluidics for diagnostic applications have focused on the physical methods behind the device operation and not as much on the applications, this work will focus on some specific diagnostic developments and application areas. We examine the microfluidic applications in diagnostics for diabetes, cardiac related conditions, and infections related to bacteria, virus, and HIV. We also review the applications in pharmacogenomics and devices for low resource settings. We discuss some of the methods used in fabricating these microfluidic devices and the challenges in mass production. Included is a section on some of the commercial diagnostic products using microfluidic technology. The reader may refer to supplemental reviews for the theory behind microfluidics (10, 75–78) and methods used in microfluidic LOC detection (14, 67, 79).
5 A Global Health Perspective
There is an increasing need in the developing and developed world for new cost-effective diagnostic technologies, albeit for different reasons. In developed countries, health care costs are rising rapidly, and containment is an issue. In developing countries, delivery of medical services to remote and resource poor areas is difficult and the needs are enormous, as infectious disease is a critical barrier to economic and social development. Interestingly, the two problems tend to converge towards one solution: microfluidic diagnostic devices. The Grand Challenges in Global Health (GCGH) initiative, a major effort to achieve scientific breakthroughs against infectious diseases that cause significant problems in the developing world, has identified seven long-term goals in global health (80), most of which revolve around eliminating infectious disease.
Infectious diseases constitute a huge burden in developing countries (32.1%) using disability-adjusted life year (DALY) metrics compared to developed countries (3.7%) and account for 50% of infant deaths (1, 81). The major concerns in terms of DALY are infections due to viruses (HIV/AIDS, measles, hepatitis B, hepatitis C, and viral gastroenteritis [rotavirus]); bacteria (cholera, tuberculosis, pertussis, tetanus, and meningitis); and parasites (malaria, Lymphatic filariasis, leishmaniasis, and trypanosomiasis). The three most devastating diseases are malaria, tuberculosis, and HIV. In 2009, there was an estimated 169–294 million cases of malaria worldwide, resulting in about 781,000 deaths. Of these 85% of deaths were in children under 5 years of age [82). There was an estimated 14 million people infected with TB and about 1.7 million related deaths in 2009. TB is a major cause of deaths in HIV infected patients with about 380,000 of the 1.7 million deaths being reported in people with HIV (83). An estimated 33.3 million people are living with HIV worldwide of which about 67.5% live in sub-Saharan Africa (84). There has been an estimated 1.8 million AIDS related deaths, 73% of those being in sub-Saharan Africa. Thus, early infectious disease detection and management is a high priority in low-resource settings and a major driver of microfluidic diagnostic devices. Infectious diseases are not limited to developing countries. Recent outbreaks like H1N1 influenza A demonstrate the rapid spread of infectious diseases from a country of origin to the rest of the world. In April 2009, USA and Mexico reported 38 cases of H1N1 influenza. By June 2009 when World Health Organization declared a pandemic, there were a reported 28,774 cases and 144 deaths in 74 countries. The H1N1 influenza pandemic had a total of 43,677 reported cases in the USA as of July 2010 (85). Estimates of unreported cases are a much higher figure at 1.8–5.7 million cases (86).
In contrast, chronic diseases that require consistent monitoring are the major disease burden for high-income countries. These diseases include: ischemic heart disease, cerebrovascular disease, cancers, and diabetes mellitus. Global mortality and disease burden projections suggest that these chronic conditions common to high-income countries will also become a priority for low-income countries by the year 2030 (1). Thus, the driver for microfluidic diagnostics in developed countries is the need for consistent, accurate, and affordable diagnostics for chronic disease.
6 Microfluidics in Diagnostics
6.1 Bacterial Detection
Bacterial detection is a key need in areas including: clinical diagnostics, monitoring of food-borne pathogens, and detection of biological threat agents. Harmful bacteria are the source of diseases like gastroenteritis and cholera. From a bioterrorism perspective, pathogenic bacteria pose serious risk. Under favorable temperature and in the presence of moisture and nutrition, bacteria spread rapidly. For a list of bacterial diseases and corresponding causative agents the reader can refer to a review by Ivnitski et al. (87).
Conventional methods to detect and identify bacteria require growing a small number of bacteria into colonies of higher numbers. Hence conventional methods take 18–24 h at a minimum (87). Also, conventional methods require complex equipment, highly trained technicians, and cannot be field deployable or used in point-of-care settings.
There are primarily two modes of pathogen detection: immunosensing and nucleic acid-based detection. In immunosensing, a binding interaction between probing antibodies and antigens of target cells (analyte) is detected. A variety of mechanisms can be used to detect this interaction, such as: optical, electrical or electrochemical impedance, cantilever, quartz crystalline microbalance, surface plasmon resonance (SPR), and magnetoresistivity. Nucleic acid-based sensors detect DNA or RNA targets from the analyte organisms (88, 89). The polymerase chain reaction (PCR) or reverse transcription PCR (RT-PCR) is used to amplify the nucleic acids to enhance the detection signal (90).
Optical detection methods are often preferred due to their high selectivity and sensitivity (91, 92). A variety of microfluidic devices have been developed for bacteria using optical means. A microfluidic system for detection of Escherichia coli using laser-optical fiber fluorescence detection was reported by Xiang et al. They reported detection limits an order of magnitude higher than that achieved for conventional fluorescence microscope (93). Gao et al. developed a multiplexed microfluidic device for the fluorescence detection of bacterial antibodies in human serum. TRITC-labeled detection antibodies were captured by antigens pre-patterned on the microchannels (94). An integrated microfluidic platform for fluorescence-based detection of Shiga toxin I (Shigella dysenteriae) and Staphylococcal enterotoxin B (Staphylococcus aureus) was developed by Meagher et al. (95).
Electrical and electrochemical modes of bacterial detection have also been widely reported. The primary advantage of the method is the ease of fabricating microelectrodes in the microchannel by lithography and the absence of labeling steps (96). A microfluidic sensor based on impedance measurement of E. coli was constructed by Boehm et al. (97). The selectivity of the sensor to different bacterial strains was demonstrated by positive identification of E. coli in a suspension of E. coli and M. catarrhalis. A microfabricated electrochemical sensor array for detection of bacterial pathogens in human clinical fluid samples was demonstrated. The device consisting of a set of 16 sensors was able to detect relevant bacterial urinary pathogens (E. coli, Proteus mirabilis, Pseudomonas aeruginosa, Enterocococcus spp., and Klebsiella–Enterobacter group) and could in principle be used as a point-of-care device for rapid diagnosis of urinary tract infections (98). Table 2 lists a number of detection methods for bacterial diagnostics and, for a comprehensive list of electrical and electrochemical bacterial detection, the reader can refer to a review by Jinseok et al. (96).
Microfluidic devices have also been applied to the detection of parasites. A “microfluidic flow-through membrane immunoassay with on-card dry reagent storage” was developed by Stevens et al. for the detection of Plasmodium falciparum (99).
6.2 Viral Detection and Disease Management
As noted earlier in this chapter, effective virus detection and disease management is critical in public health, the biotechnology industry, and biodefense. Some of the most deadly historical epidemics like smallpox, yellow fever, and Spanish flu were due to viral agents. In the twenty-first century, HIV, rotavirus, and measles are found to be among the leading contributors to global disease burden (100). Many deadly viruses such as Variola virus (small pox), Rift Valley fever virus, and Venezuelan Equine Encephalomyelitis virus have been known to be developed as potential biological agents (101). POC devices to detect these bio-agents are extremely critical for global biosecurity. The small size, simple biology, and lack of reproductive ability outside the host cell add to the complexity in detecting viruses.
The primary methods for virus detection are serology, viral antigen detection, and nucleic acid detection. Serologic tests detect the presence of antibodies that the immune system produces in response to viral infection. Viral antigen detection typically relies on immunoassays as described previously. Nucleic acid detection involves amplification of the viral genome using PCR and the subsequent detection of the amplified genome.
6.3 HIV Detection and Monitoring
HIV is one of the primary targets of microfluidic diagnostic research efforts. Conventional HIV diagnostic assays are based on an enzyme assay (EIA/ELISA) followed by western blot and requires trained laboratory personnel. Universal access to HIV diagnostics is stymied by the lack of trained technicians, patient motivation, and laboratory access especially in rural areas and the developing world. For instance, about 83% of HIV patients remain undiagnosed in Kenya (102). Thus, a simple, inexpensive diagnostic tool for HIV would be readily welcomed.
The number of CD4+ T-lymphocytes per microliter of HIV-infected blood is a critical monitor of disease state and this measurement is needed to make informed antiretroviral therapy (ART) treatment decisions. Therefore, the primary mechanisms for HIV detection in POC microfluidic devices are enumeration of CD4+ T-lymphocytes and HIV viral load quantification. To be successful, the POC device needs to detect around 200 CD4+ cells/μL and 400 copies/mL of HIV from whole blood (103). Towards this goal, Sia et al. reported a microfluidic immunoassay, “POCKET (portable and cost-effective)” for quantifying anti-HIV-1 antibodies in the sera of HIV-1 infected patients. The device consisted of a PDMS slab with microchannels placed orthogonally to a polystyrene stripe patterned with HIV-enveloped antigen. The HIV-1 infected patient serum sample is flowed through the microchannels to quantify anti-HIV-1 antibodies. Although the device was able to identify the sera of HIV-1-infected patients from those of non-infected patients, it could not make a correlation of the output data with HIV disease states (103). Lee et al. developed a RT-PCR-based POC diagnostic chip for HIV. The chip relies on HIV markers p24 (a major core protein encoded by the HIV gag gene) and gp120 (an external envelope protein encoded by envelope gene) for diagnostic purposes (104). Cheng et al. reported a POC microfluidic CD4+ T-cell counting device. The device works in two stages, initial depletion of monocytes from whole blood and subsequent CD4+ T cell capture. The strategy of contaminant (monocytes) depletion prior to CD4+ T cell isolation enhances the performance in low CD4 count (200 cells/μL) scenarios (105). Other label-free CD4+ T-lymphocyte capture techniques have been reported. Although the microfluidic devices themselves are disposable and usually cheap, they still require expensive optical microscopes to count the captured CD4+ T-cells (106, 107). A lensless portable CCD-based microfluidic platform developed by Demirci et al. overcomes this limitation. The captured label-free CD4+ T-lymphocytes are detected by a charge coupled device (CCD) sensor using lensless shadow imaging techniques and counted using automatic cell counting software in a few seconds (108). Cheng et al. developed a non-optical method of counting CD+ T-cells. The cell count is enumerated by measuring the changes in conductivity of the surrounding medium due to ions released from the surface-immobilized cells within a microfluidic channel (109). Gohring et al. demonstrated the detection of CD4+ and CD8+ T-Lymphocyte whole cells and CD4+ T-Lymphocyte cell lysis using an optofluidic ring resonator (OFRR) sensor. This sensor measures the presence of T cells based on a change in refractive index in the microfluidic channel due to the presence of immobilized T cells (110). Wang et al. reported a microfluidic chip with an integrated micromixer for fluorescent labeling of CD4+/CD8+ T-cells and their subsequent counting using a microflow cytometer (111).
6.4 Diagnostics for Other Viral Agents
Microfluidic diagnostics have been designed for other viral agent infections like influenza, severe acute respiratory syndrome (SARS) and dengue fever. These diseases have been of serious concern to global public health organizations especially in the last few years.
The influenza virus causes respiratory tract infection and is found to be severely morbid in children and the elderly (112). The challenge with diseases like influenza is that there is a large variety of the viruses and they are constantly changing. For example, the influenza A virus can subdivided into H1N1 and H1N3 based on the glycoproteins (hemagglutinin and neuraminidase) present in the viral envelope. The 2009 influenza pandemic was caused by a novel H1N1 strain with genes from five different flu viruses (113). Thus, the diagnosis of influenza alone is not sufficient; discovery of the type of influenza is also critical.
Some of the conventional diagnostic methods for influenza virus are enzyme-linked immunosorbent assays (ELISA), immunofluorescence assays, serological hemagglutination inhibition assays, real-time polymerase chain reaction (PCR) assays, and complement fixation tests. Most of these methods are complicated, relatively costly and require a lengthy process and expensive apparatus (114).
Several microfluidic systems have been shown for influenza detection. An immunomagnetic bead-based microfluidic system for detection of influenza A virus has been demonstrated recently. Influenza A viral particles are initially bound to monoclonal antibody (mAb)-conjugated immunomagnetic beads using a suction type micro-mixer. Subsequently the virus-bound magnetic complexes are fluorescently labeled by developing mAb with R-phycoerythrin. An external optical detection module is used to analyze the optical intensity of the magnetic complex. The system displayed better performance than conventional flow cytometry systems in terms of limit of detection (114). However, the expensive external optical detection module could restrict its use in POC low-resource settings. Yamanaka et al. reported a microfluidic RT-PCR chip for rapid detection of influenza (AH1pdm) virus of swine-origin. A disposable electrical printed chip was used for electrochemical detection of the PCR amplicon (112). The electrochemical method is better for use in low-resource settings compared to the optical methods reported above due to the absence of expensive external detection units. A Magnetic Integrated Microfluidic Electrochemical Detector (MIMED) for detection of H1N1 influenza virus from throat swab samples has recently been developed (115).
Microfluidics detection methods for other types of viral agents have been reported. Weiss et al. reported a microfluidic chip-based electrophoretic analysis and laser-induced fluorescence detection of human rhinovirus serotype 2 (116). Zhu et al. developed an optofluidic micro-ring resonator-based system for detection of bacteriophage M13 (117). They reported a detection limit of 2.3 × 103 PFU/mL. An on-chip surface enhanced Raman spectroscopy (SERS)-based biomolecular device for detection of Dengue virus sequences was developed by Huh et al. (118). The fluid is actuated using electrokinetic methods and the limit of detection was reported to be 30 pM. Weng et al. developed a suction-type, pneumatically driven microfluidic device for the detection of dengue infection (119). A detection limit of 10 PFU/ml was reported for the device. A “lab-on-a-disc” centrifugal microfluidics-based portable ELISA system was developed for detection of the antigen and the antibody of Hepatitis B virus (120). The limit of detection of antigen and antibody were reported as 0.51 ng/mL and 8.6 mIU/mL, respectively. Heinze et al. developed a microfluidic immunosensor for detection of bovine viral diarrhea virus (121). An integrated microfluidic assay for targeted ribonucleic acid (RNA) extraction and a one-step reverse transcription loop-mediated-isothermal-amplification (RT-LAMP) process for the detection of nervous necrosis viruses was reported by Wang et al. (122).
6.5 Cancer Biomarker Detection
In 2010, there were an estimated 1,500 cancer related deaths per day in the USA and about 1.4 million new cases of cancer were reported. By 2020, cancer related deaths are estimated to be 10.3 million globally. The cancer mortality rate per 100,000 Americans has dropped from 194 to 190 since 1950, an insignificant drop compared to drop in mortality rates for other diseases. Most of the improvements in cancer survival rates are due to improvements in early diagnosis rather than treatment. For instance, for cancers of the breast, colon, rectum, and cervix, early detection has proved to reduce mortality significantly. Hence, the National Cancer Institute has emphasized a shift from therapeutic to preventive mode in its 2010 vision document.
Existing methods of cancer diagnostics rely on invasive techniques like taking a biopsy and then examining the cell morphology. Further, conventional methods could be inconclusive in disease detection in its early stages (123). Other techniques like immunoassays (ELISA) have been used to detect cancer biomarkers. Although ELISAs are very sensitive, they can be time consuming, expensive and are mostly carried out in a laboratory requiring skilled personnel. In most cases, immunoassays look for only one biomarker and are not sensitive enough to detect very low biomarker levels especially at early stages of the disease. POC devices which are accurate, fast and economic are needed. This would enable improved diagnosis, monitoring of the progress of the disease, and response to therapy.
Advances in oncology have led to identification of biomarkers associated with different kinds of cancers. For a comprehensive list of cancer biomarkers, the reader can refer to reviews in literature (124–129). There are multiple factors responsible for carcinogenesis. This along with the “heterogeneity in oncogenic pathways” makes it imperative that a range of biomarkers need to be analyzed for cancer diagnostics (123, 130). Hence POC devices with multiplexed capability to detect multiple biomarkers are needed. Although research into cancer diagnostic devices is moving forward, commercialization of the technology still remains a challenge (123).
Here, we review some of the recent research in microfluidics POC devices for cancer diagnostics. Legendre et al. reported work into the design and development of a microfluidic device for diagnosis of T-cell lymphoma. The system accepts a whole blood sample as the input, extracts the DNA, amplifies target sequences of the T-cell receptor-gene, and eletrophoretically resolves the products for detection of a signature consistent with monoclonality (131). Diercks et al. demonstrated a microfluidic device that measured multiple proteins (tumor necrosis factor, CXC chemokine ligand 2, interleukin 6 and interleukin 1b) at pg/mL concentrations in nanoliter volumes. Antibody-coupled polystyrene microspheres labeled with embedded fluorophores were used to detect the analyte (proteins). Optical detection of captured analyte was performed off-chip using a confocal microscope, which proved to be a disadvantage in terms of lack of device portability (132). A similar fluorescence approach has been used to detect vascular endothelial growth factors in human plasma (133). An on-chip nuclear magnetic resonance (NMR)-based biosensor was developed for the multiplexed identification of cancer markers (epidermal growth factor receptors EGFR and Her2/neu). The design consists of a microcoil array for NMR measurements, microfluidic channels for sample handling and a permanent magnet to generate a polarizing magnetic field, all integrated into a handheld device (134). Mass spectroscopy-based microfluidic detection of cancer-specific biomarkers (proliferating cell nuclear antigen, cathepsin D, and keratins K8, K18, and K19) was demonstrated by Lazar (135).
Other mass-based methods like quartz crystal microbalance (QCM) have been used in cancer biomarker detection. For instance, Zhang et al. demonstrated detection of human lung carcinoma cells using a microfluidic surface modified piezoelectric sensor (136). Recently, Von Muhlen et al. have reported a microcantilever-based “suspended microchannel resonator” sensing device for detection of activated leukocyte cell adhesion molecules (137). Zani et al. demonstrated an electrochemical method for detection of prostate specific antigen (PSA) cancer markers. The method works based on the differential pulse voltammetry-based electrochemical detection of protein coated paramagnetic microparticles that selectively capture the analyte (PSA) (138). Similar electrochemical detection methods for breast cancer markers have been reported (139). A microfluidic-based amperometric electrochemical detection system for carcinoembryonic antigen (CEA) and cancer antigen 15–3 (CA15-3) was developed by Kellner et al. The on-chip fluid function is handled by computer controlled syringe pumps and reports enhanced performance due to fully automated fluidic operations (140). But the external computer control system and syringe pumps prove to be a bottleneck in their use for POC applications. Hence miniaturization and integration of the fluid handling functions within the microfluidic chip is necessary for POC use.
6.6 Cardiac Biomarker Detection
Cardiovascular diseases (CVD) are responsible for nearly half of the deaths in the western world. Studies suggest the acute and long term financial burden of cardiac disease to be substantial (141). It is reported that 5% of myocardial infarction (MI) patients are incorrectly discharged from emergency departments (ED). Hence for timely and effective intervention against cardiovascular diseases, there is a need for rapid and accurate diagnostic tools (142).
For the accurate “diagnosis, prognosis, monitoring and risk stratification of patients with acute coronary syndromes” (ACS), biochemical markers play a fundamental role (142). In clinical settings, in 50–70% of patients with ACS related cases, ECGs give ambiguous results. In such cases, cardiac marker levels could provide critical information for informed decision on the suitable treatment. As a definite indicator of disease condition a combination of cardiac markers need to be explored (143). For a review of cardiac biomarkers, the reader can refer to McDonnell et al. (142).
There is a difference of opinion with regard to the use of POC technologies for cardiac biomarker diagnostic, with some suggesting it to be an alternative to conventional lab analyzers (144, 145) and others questioning the accuracy of the technologies (146, 147). The following section provides a review of microfluidic devices used in cardiac biomarker detection.
Most of the diagnostic mechanisms for biomarkers involve two steps, an initial immunoassay to capture the analyte (biomarker) and subsequent detection of the captured analyte. Using optical methods, Jönsson et al. demonstrated a lateral flow polymer chip for detection of C Reactive Protein (CRP) (148). Gervais et al. demonstrated a microfluidic device for one step detection of CRP in serum. The device works based on capillary action for fluid actuation and does not need any external power requirements (149), which makes it extremely useful in a POC, low-cost setting. A multiplexed cardiac biomarker detection prototype device was developed by Hong et al. The MEMS-based device detected four different cardiac markers viz. myoglobin, CRP, cTnI and BNP using Au nanoparticle-based fluorescence detection (150). Bhattacharyya & Klapperich developed a disposable microfluidic chip for detection of CRP including an on-board detection module (151). A microfluidic chemiluminescence-based immunoassay system for detection of cardiac troponin I (cTnI) was reported by Cho et al. (152). Huang et al. demonstrated a microfluidic chemiluminescence-based detection sensor for alpha-fetoprotein (AFP). Super-paramagnetic microbeads were used to capture the biomarker (153). Use of magnetic microbeads results in higher surface to volume ratio for efficient analyte capture and enables on-chip actuation using an integrated electromagnet. A digital microfluidic platform detection device for cTnI was developed by Sista et al. (154). The fluidic actuation is performed by electrowetting, obviating the need for any off-chip fluid handling apparatus. SPR-based microfluidic detection of cardiac marker B-type natriuretic peptide (BNP) was reported by Kurita et al. (155).
Electrochemical methods have been applied to detection of cardiac markers. Unlike optical methods, these do not need an often expensive, off-chip optical detection device and could be suitable for POC applications. Tweedie et al. presented a microfluidic-based impedimetric sensing device for cardiac enzymes (156). The i-STAT system (Abbott Point of Care Inc., USA) is a commercial test cartridge for electrochemical detection of cTnI (157). The device can detect cTnI in the range of 0–50 ng/ml and has gained good acceptance as a diagnostic tool for MI (143). Other electrochemical-based detection methods for detection of myoglobin (158), cTnI (159) and CRP (160) have been reported. Recently, Mitsakakis and Gizeli have developed an integrated microfluidic surface acoustic wave (SAW) platform for detection of cardiac markers creatine kinase MB (CK-MB), CRP, and D-dimer (161).
Many commercial systems for cardiac marker detection are currently available, which could possibly limit the impact of microfluidic devices in this area. These include Triage® [Biosite Diagnostics Inc., USA] (myoglobin, CK-MB, and cTnI), Stratus® CS STAT fluorometric analyzer [Siemens Medical Diagnostics, USA] (myoglobin, CK-MB, and cTnI), Roche cardiac reader [Roche Diagnostics, USA] (cTnT, myoglobin), RAMP™ cardiac marker testing [Response Biomedical Inc., Canada] (cTnI, CK-MM), and Cardiac STATus™ device [Nanogen Inc., USA] (myoglobin, CK-MB mass, and cTnI) (157). Table 3 lists the set of published work and commercial devices for microfluidic cardiac marker detection.
6.7 High Throughput and Multiplexed Diagnostic Screening
Microfluidic-based technology is ideal for developing highly parallel diagnostic assays that would allow high-throughput screening, but there has been limited success in this area. The lack of success is not due to problems with microfluidic devices; for example, drug screening requires high-throughput methods to find and test different drug candidates. Microfluidic high-throughput screening (HTS) techniques have been applied to drug discovery to perform thousands of tests in parallel with some success (162–164). As of now these methods haven’t been applied in microfluidic diagnostics for several reasons. Current diagnostics are typically performed in large hospitals or reference labs. In these labs, most tests are batched and performed using robots in a highly parallel, high throughput approach. Replacing these robots by using microfluidics is unlikely in the short term due to the large infrastructure already developed. Essentially, a solution to this problem already exists, so adoption of microfluidics for these assays will only occur if there are compelling assay improvements. In addition, if an assay can be performed in a batch mode using microfluidics, it is likely to be able to be performed in the clinic or POC setting, and for nearly the same price. Thus, microfluidics is likely to be driven to the POC rather than to large reference laboratories.
The reverse of high-throughput screening (multiple samples with one target) is multiplexed screening, where one sample is tested for multiple agents or biomarkers. A few examples of multiplexed screening have already been provided, especially for cardiac biomarkers, but highly multiplexed diagnostics are still being developed. Multiplexed screening is likely to have a more significant impact on diagnostics than high throughput screening, especially with the move towards personalized medicine. Microfluidics has been combined with microarray technology, which is used regularly in genomics and proteomics, and which will likely have diagnostic applications in the future; however, this is beyond the scope of the chapter. More relevant are microfluidic devices that can diagnose multiple diseases simultaneously. A recently released product that uses “mesoscale” fluidics can simultaneously diagnose 15 respiratory diseases associated with viruses (165). A challenge with getting the device to commercialization is that regulatory agencies such as the FDA require individual validation of each assay, meaning that multiplexing must clear very challenging regulatory requirements, which will likely limit substantial multiplexing in the near future. Nevertheless, microfluidics will probably lead to highly multiplexed assays that can perform 100s or 1,000s of diagnostic assays on one sample.
7 Microfluidic Commercialization
About 1,200 patents related to microfluidics have been issued in the USA through 2010. In spite of immense academic interest in microfluidics and significant research investment directed towards both academic and industrial organizations, relatively few commercial products based on microfluidics have been introduced into the market (166, 167); however, the rate of introduction is increasing and many barriers are coming down. One of the reasons cited for lack of commercial success is the lack of a potential “blockbuster” end-user product that could generate billions of dollars in revenue. Until the industry can find a product with high volume demand, the fabrication costs due to lack of “economies of scale” are going to remain high. Existing materials like PDMS, which are hugely popular in research, have not succeeded in the industry due to issues with manufacturability and scaling (168). Most of the LOC products are still focused on the business-to-business segment and not the business-to-consumer (167). There needs to be more focused research on microfluidic product development including issues like manufacturability and cost dynamics and a simultaneous search for new application areas where microfluidics could be applied. Table 4 provides a sample of microfluidic companies and products in the market. More comprehensive lists are available (169).
8 Summary and Future Outlook
Microfluidic diagnostic devices have been developing at a rapid rate over the past few years. While the potential for these devices was first recognized more than 20 years ago, the realization of that potential has been slow, even though thousands of devices and methods have been published. The continuing development of applications and microfluidic manufacturing methods, including platform technologies that can be customized easily for each diagnostic test, will be the drivers of success. Very recent progress and an emphasis on global health has helped move the field towards POC devices that will likely become ubiquitous in the years ahead. While most microfluidic devices have one diagnostic target, devices capable of diagnosing 100s or 1,000s of diseases will likely be developed and commercialized in the next decade, making microfluidics a major driver of disease diagnostics.
References
Yager P, Domingo GJ, Gerdes J (2008) Point-of-care diagnostics for global health. Annu Rev Biomed Eng 10:107–144
Kiechle FL, Holland CA (2009) Point- of-Care Testing and Molecular Diagnostics: Miniaturization Required. Clin Lab Med 29(3):555–560
UNAIDS (2010) UNAIDS Report on the global AIDS epidemic, UNAIDS.
Steven J, Zullo SS, Patrick Looney J, Barker PE (2010) Nanotechnology: Emerging Developments and Early Detection of Cancer, A Two-Day Workshop sponsored by the National Cancer Institute and the National Institute of Standards and Technology, National Cancer Institute, Gaithersburg.
Foster RS, Heffler SK (2009) Updated and Extended National Health Expenditure Projections, 2010–2019, Office of the Actuary. Centers for Medicare & Medicaid Services, Maryland
Cirino NM, Musser KA, Egan C (2004) Multiplex diagnostic platforms for detection of biothreat agents. Expert Rev Mol Diagn 4:841–857
(USDA) U S D o HHS H a A (ed) (2011) National select agent registry: overview. Department of Health & Human Service, Washington DC
Food and Drug Administration (2008) Recommendations: Clinical Laboratory Improvement Amendments of 1988 (CLIA Waiver Applications for Manufacturers of In Vitro Diagnostic Devices.
Sia SK, Kricka LJ (2008) Microfluidics and point-of-care testing. Lab Chip 8:1982–1983
Whitesides GM (2006) The origins and the future of microfluidics. Nature 442:368–373
Arora A et al (2010) Latest developments in micro total analysis systems. Anal Chem 82:4830–4847
Salieb-Beugelaar GB et al (2010) Latest developments in microfluidic cell biology and analysis systems. Anal Chem 82:4848–4864
West J et al (2008) Micro total analysis systems: latest achievements. Anal Chem 80:4403–4419
Trietsch SJ et al (2011) Lab-on-a-chip technologies for massive parallel data generation in the life sciences: a review Chemometr Intell Lab 108:64–75.
Weston AD, Hood L (2004) Systems biology, proteomics, and the future of health care: toward predictive, preventative, and personalized medicine. J Proteome Res 3:179–196
Reyes DR (2002) Micro Total Analysis Systems. 1. Introduction. Theory, and Technology 74(12):2623–2636
Jacobson SC, Moore AW, Ramsey JM (1995) Fused quartz substrates for microchip electrophoresis. Anal Chem 67:2059–2063
von Heeren F et al (1996) Micellar electrokinetic chromatography separations and analyses of biological samples on a cyclic planar microstructure. Anal Chem 68:2044–2053
Moore AW Jr, Jacobson SC, Ramsey JM (1995) Microchip separations of neutral species via micellar electrokinetic capillary chromatography. Anal Chem 67:4184–4189
Woolley AT, Mathies RA (1995) Ultra-high-speed DNA sequencing using capillary electrophoresis chips. Anal Chem 67:3676–3680
Shoffner MA et al (1996) Chip PCR. I. Surface passivation of microfabricated silicon-glass chips for PCR. Nucleic Acids Res 24:375–379
Koutny LB et al (1996) Microchip electrophoretic immunoassay for serum cortisol. Anal Chem 68:18–22
Hadd AG et al (1997) Microchip device for performing enzyme assays. Anal Chem 69:3407–3412
Colyer CL, Mangru SD, Harrison DJ (1997) Microchip-based capillary electrophoresis of human serum proteins. J Chromatogr A 781:271–276
Raymond DE, Manz A, Widmer HM (1996) Continuous separation of high molecular weight compounds using a microliter volume free-flow electrophoresis microstructure. Anal Chem 68:2515–2522
von Heeren F et al (1996) Characterization of electrophoretic sample injection and separation in a gel filled cyclic planar microstructure. J Microcolumn Separations 8:373–381
Woolley AT, Sensabaugh GF, Mathies RA (1997) High-speed DNA genotyping using microfabricated capillary array electrophoresis chips. Anal Chem 69:2181–2186
Delamarche E et al (1997) Patterned delivery of immunoglobulins to surfaces using microfluidic networks. Science 276:779
Freaney R et al (1997) Novel instrumentation for real-time monitoring using miniaturized flow systems with integrated biosensors. Ann Clin Biochem 34:291–302
Manz A, Graber N, Widmer HM (1990) Miniaturized total chemical analysis systems: a novel concept for chemical sensing. Sensors Actuators B: Chemical 1:244–248
Harrison DJ, Manz A, Glavina PG (1991) Electroosmotic pumping within a chemical sensor system integrated on silicon. In: Proc. IEEE Int. Conf. Solid-State Sensors and Actuators (Transducers ‘91), San Francisco, USA, pp 792–795
Seiler K, Harrison DJ, Manz A (1993) Planar glass chips for capillary electrophoresis: repetitive sample injection, quantitation, and separation efficiency. Anal Chem 65:1481–1488
Sobek D et al. (1993) A microfabricated flow chamber for optical measurements in fluids. In: Proc. 6th IEEE MEMS, Fort Lauderdale, USA, pp 219–224
Northrup MA et al. (1993) DNA amplification with a microfabricated reaction chamber. In: Proc. of The 7th Int. Conf. on Solid-State Sensors and Actuators (Transducers ‘93), Yokohama, Japan, pp 924–926
Bousse L et al (1994) Micromachined multichannel systems for the measurement of cellular metabolism. Sensors Actuators B: Chemical 20:145–150
Jacobson SC et al (1994) Precolumn reactions with electrophoretic analysis integrated on a microchip. Anal Chem 66:4127–4132
Jacobson SC et al (1994) Microchip capillary electrophoresis with an integrated postcolumn reactor. Anal Chem 66:3472–3476
Jacobson SC et al (1994) High-speed separations on a microchip. Anal Chem 66:1114–1118
Mensinger H et al (1995) Microreactor with integrated static mixer and analysis system. Kluwer Academic Publishers, The Netherlands, p 237
Effenhauser CS et al (1994) High-speed separation of antisense oligonucleotides on a micromachined capillary electrophoresis device. Anal Chem 66:2949–2953
Woolley AT, Mathies RA (1994) Ultra-high-speed DNA fragment separations using microfabricated capillary array electrophoresis chips. Proc Natl Acad Sci 91:11348
Fan ZH, Harrison DJ (1994) Micromachining of capillary electrophoresis injectors and separators on glass chips and evaluation of flow at capillary intersections. Anal Chem 66:177–184
Fuhr G, and Wagner B. (1994) Electric field mediated cell manipulation, characterisation and cultivation in highly conductive media. Paper presented at the MicroTAS, University of Twente, Netherlands, 21–22 Nov 1994
Manz A et al (1994) Electroosmotic pumping and electrophoretic separations for miniaturized chemical analysis systems. J Micromech Microeng 4:257
Raymond DE, Manz A, Widmer HM (1994) Continuous sample pretreatment using a free-flow electrophoresis device integrated onto a silicon chip. Anal Chem 66:2858–2865
Verpoorte EMJ et al (1994) Three-dimensional micro flow manifolds for miniaturized chemical analysis systems. J Micromech Microeng 4:246
Seiler K et al (1994) Electroosmotic pumping and valveless control of fluid flow within a manifold of capillaries on a glass chip. Anal Chem 66:3485–3491
Jacobson SC et al (1994) Open channel electrochromatography on a microchip. Anal Chem 66:2369–2373
Feustel A, Muller J, Relling V (1995) A microsystem mass spectrometer. Springer, Berlin, p 299
Kim E, Xia Y, Whitesides GM (1995) Polymer microstructures formed by moulding in capillaries. Nature 376:581–584
Xia Y, Whitesides GM (1998) Soft lithography. Ann Rev Mat Sci 28:153–184
Whitesides GM et al (2001) Soft lithography in biology and biochemistry. Annu Rev Biomed Eng 3:335–373
Mrksich M, Whitesides GM (1995) Patterning self-assembled monolayers using microcontact printing: a new technology for biosensors? Trends Biotechnol 13:228–235
Zhao XM, Xia Y, Whitesides GM (1996) Fabrication of three dimensional micro structures: Microtransfer molding. Adv Mater 8:837–840
Bartholomeusz DA, Boutté RW, Gale BK (2009) Xurography: Microfluidic Prototyping with a Cutting Plotter. In: Herold K, Rasooly A (eds) Lab on a Chip Technology: Fabrication and Microfluidics. Caister Academic Press, United Kingdom, pp 65–82
Gale BK et al (2008) Fabrication and packaging: Low-cost MEMS technologies. In: Gianchandani YB, Tabata O, Zappe HP (eds) Comprehensive microsystems. Elsevier, Amsterdam, pp 341–378
Martynova L et al (1997) Fabrication of plastic microfluid channels by imprinting methods. Anal Chem 69:4783–4789
Gonzalez C, Collins SD, Smith RL (1998) Fluidic interconnects for modular assembly of chemical microsystems. Sens. Actuators B: Chemical 49:40–45
Johnson KS et al (1996) Using neutral metastable argon atoms and contamination lithography to form nanostructures in silicon, silicon dioxide, and gold. Appl Phys Lett 69:2773–2775
Lorenz H et al (1997) SU-8: a low-cost negative resist for MEMS. J Micromech Microeng 7:121
Larsson O et al (1997) Silicon based replication technology of 3D-microstructures by conventional CD-injection molding techniques. IEEE 1412:1415–1418
Klaassen EH et al. (1996) Silicon fusion bonding and deep reactive ion etching; a new technology for microstructures. Sens. Actuators A: Physical 52:132–139
Juan WH, Pang SW (1995) A novel etch-diffusion process for fabricating high aspect ratio Si microstructures. In: Proc. 8th Int. Conf. Solid-State Sensors and Actuators (Transducers ‘95), Stockholm, Sweden, pp 560–563
Madou MJ (2002) Fundamentals of microfabrication: the science of miniaturization. CRC, Boca Raton, FL
Rolland JP et al (2004) High Resolution Soft Lithography: Enabling Materials for Nanotechnologies. Angewandte Chemie 116:5920–5923
Wasatch Microfluidics, LLC, www.microfl.com. 12 Nov 2012
Rivet C et al (2010) Microfluidics for medical diagnostics and biosensors. Chem Engine Sci 66:1490–1507
Crews N, Wittwer C, Gale B (2008) Continuous-flow thermal gradient PCR. Biomed Microdevices 10:187–195
Bartholomeusz DA, Boutté RW, Andrade JD (2005) Xurography: rapid prototyping of microstructures using a cutting plotter. Microelectromechanical Syst J 14:1364–1374
Klank H, Kutter JP, Geschke O (2002) CO2-laser micromachining and back-end processing for rapid production of PMMA-based microfluidic systems. Lab Chip 2:242–246
Becker H, Gärtner C (2008) Polymer microfabrication technologies for microfluidic systems. Anal Bioanal Chem 390:89–111
Martinez AW, Phillips ST, Whitesides GM (2008) Three-dimensional microfluidic devices fabricated in layered paper and tape. Proc Natl Acad Sci 105:19606–19611
Martinez AW et al (2009) Diagnostics for the developing world: microfluidic paper-based analytical devices. Anal Chem 82:3–10
Bhattacharyya A, Klapperich CM (2006) Thermoplastic microfluidic device for on-chip purification of nucleic acids for disposable diagnostics. Anal Chem 78:788–792
Yager P et al (2006) Microfluidic diagnostic technologies for global public health. Nature 442:412–418
Squires TM, Quake SR (2005) Microfluidics: Fluid physics at the nanoliter scale. Rev Mod Phys 77:977
Psaltis D, Quake SR, Yang C (2006) Developing optofluidic technology through the fusion of microfluidics and optics. Nature 442:381–386
Demello AJ (2006) Control and detection of chemical reactions in microfluidic systems. Nature 442:394–402
Myers FB, Lee LP (2008) Innovations in optical microfluidic technologies for point-of-care diagnostics. Lab Chip 8:2015–2031
Singer PA et al (2007) Grand challenges in global health: the ethical, social and cultural program. PLoS Med 4:e265
Chin CD, Linder V, Sia SK (2007) Lab-on-a-chip devices for global health: past studies and future opportunities. Lab Chip 7:41–57
World Health Organization (2010) World malaria report: 2010. World Health Organization, Geneva
World Health Organization (2010) 2010/2011 Tuberculosis Global Facts, Geneva.
United Nations (2000) United Nations Millennium Declaration.
World Health Organization. (2009–2010) Situation updates - Pandemic (H1N1) 2009, World Health Organization, Geneva.
Reed C et al (2009) Estimates of the prevalence of pandemic (H1N1) 2009, United States, April-July 2009. Emerg Infect Dis 15:2004–2007
Ivnitski D et al (1999) Biosensors for detection of pathogenic bacteria. Biosens Bioelectron 14:599–624
Kim J et al. (2010) Sample to answer: a fully integrated nucleic acid identification system for bacteria monitoring. In: Becker H, Wang W (eds) Proc. SPIE, vol 7593, pp 75930S
Kim J et al (2009) Microfluidic sample preparation: cell lysis and nucleic acidpurification. Integr Biol 1:574–586
Sant HJ et al (2010) Integrated Microfluidics for Serotype Identification of Foot and Mouth Disease Virus, in Proceedings of The 14th International Conference on Miniaturized Systems for Chemistry and Life Sciences. Groningen, The Netherlands
Velusamy V et al (2010) An overview of foodborne pathogen detection: In the perspective of biosensors. Biotechnol Adv 28:232–254
Lazcka O, Campo F, Munoz FX (2007) Pathogen detection: A perspective of traditional methods and biosensors. Biosens Bioelectron 22:1205–1217
Xiang Q et al (2006) Miniaturized immunoassay microfluidic system with electrokinetic control. Biosens Bioelectron 21(10):2006–2009
Gao Y et al (2008) Multiplexed high-throughput electrokinetically-controlled immunoassay for the detection of specific bacterial antibodies in human serum. Anal Chim Acta 606:98–107
Meagher RJ et al (2008) An integrated microfluidic platform for sensitive and rapid detection of biological toxins. Lab Chip 8:2046–2053
JinSeok H, Hua SZ (2009) An overview of recent strategies in pathogen sensing. Sensors 9:4483–4502
Boehm DA, Gottlieb PA, Hua SZ (2007) On-chip microfluidic biosensor for bacterial detection and identification. Sensors Actuators B: Chemical 126:508–514
Liao JC et al (2006) Use of electrochemical DNA biosensors for rapid molecular identification of uropathogens in clinical urine specimens. J Clin Microbiol 44:561–570
Stevens DY et al (2008) Enabling a microfluidic immunoassay for the developing world by integration of on-card dry reagent storage. Lab Chip 8:2038–2045
Cheng X, Chen G, Rodriguez WR (2009) Micro-and nanotechnology for viral detection. Anal Bioanal Chem 393:487–501
Kortepeter MG, Parker GW (1999) Potential biological weapons threats. Emerg Infect Dis 5:523–527
Desai D, Wu G, Zaman MH (2010) Tackling HIV through robust diagnostics in the developing world: current status and future opportunities. Lab Chip 11(2):194–211
Lee WG et al (2010) Nano/Microfluidics for diagnosis of infectious diseases in developing countries. Adv Drug Deliv Rev 62:449–457
Lee SH et al (2008) A polymer lab-on-a-chip for reverse transcription (RT)-PCR based point-of-care clinical diagnostics. Lab Chip 8:2121–2127
Cheng X et al (2009) Enhancing the performance of a point-of-care CD4+ T-cell counting microchip through monocyte depletion for HIV/AIDS diagnostics. Lab Chip 9:1357–1364
Cheng X et al (2007) A microfluidic device for practical label-free CD4+ T cell counting of HIV-infected subjects. Lab Chip 7:170–178
Cheng X et al (2007) A microchip approach for practical label-free CD4+ T-cell counting of HIV-infected subjects in resource-poor settings. JAIDS J Acquired Immune Deficiency Syndrom 45:257–261
Moon SJ et al (2009) Integrating microfluidics and lensless imaging for point-of-care testing. Biosens Bioelectron 24:3208–3214
Cheng X et al (2007) Cell detection and counting through cell lysate impedance spectroscopy in microfluidic devices. Lab Chip 7:746–755
Gohring JT, Fan X (2010) Label Free Detection of CD4+ and CD8+ T Cells Using the Optofluidic Ring Resonator. Sensors 10:5798–5808
Wang JH et al (2011) An integrated microfluidic system for counting of CD4+/CD8+ T lymphocytes. Microfluid Nanofluid 10:531–541
Yamanaka K et al (2011) Rapid detection for primary screening of influenza A virus: microfluidic RT-PCR chip and electrochemical DNA sensor. Analyst 136(10):2064–2068
Neumann G, Noda T, Kawaoka Y (2009) Emergence and pandemic potential of swine-origin H1N1 influenza virus. Nature 459:931–939
Lien KY et al (2011) Rapid detection of influenza A virus infection utilizing an immunomagnetic bead-based microfluidic system. Biosens Bioelectron 26:3900–3907
Ferguson BS et al (2011) Genetic Analysis of H1N1 Influenza Virus from Throat Swab Samples in a Microfluidic System for Point-of-Care Diagnostics. J Am Chem Soc 133(23):9129–9135
Weiss VU et al (2007) Virus analysis by electrophoresis on a microfluidic chip. J Chromatogr B 860:173–179
Zhu H et al (2008) Opto-fluidic micro-ring resonator for sensitive label-free viral detection. Analyst 133:356–360
Huh YS et al (2008) Enhanced on-chip SERS based biomolecular detection using electrokinetically active microwells. Lab Chip 9:433–439
Weng CH et al (2011) A suction-type microfluidic immunosensing chip for rapid detection of the dengue virus. Biomed Microdevices 13(3):585–595
Lee BS et al (2009) A fully automated immunoassay from whole blood on a disc. Lab Chip 9:1548–1555
Heinze BC et al (2009) Microfluidic immunosensor for rapid and sensitive detection of bovine viral diarrhea virus. Sensors and Actuators B: Chemical 138:491–496
Wang C et al (2011) An integrated microfluidic loop-mediated-isothermal-amplification system for rapid sample pre-treatment and detection of viruses. Biosens Bioelectron 26(5):2045–2052
Tothill IE (2009) Biosensors for cancer markers diagnosis. Elsevier, Amsterdam, pp 55–62
Choi YE, Kwak JW, Park JW (2010) Nanotechnology for early cancer detection. Sensors 10:428–455
Kumar S, Mohan A, Guleria R (2006) Biomarkers in cancer screening, research and detection: present and future: a review. Biomarkers 11:385–405
Hanash SM, Pitteri SJ, Faca VM (2008) Mining the plasma proteome for cancer biomarkers. Nature 452:571–579
Saerens D et al (2008) Antibody fragments as probe in biosensor development. Sensors 8:4669–4686
D’Haeseleer P (2006) How does DNA sequence motif discovery work? Nat Biotechnol 24:959–961
Makarov DV et al (2009) Biomarkers for prostate cancer. Annu Rev Med 60:139–151
Wang J (2006) Electrochemical biosensors: towards point-of-care cancer diagnostics. Biosens Bioelectron 21:1887–1892
Legendre LA et al (2008) Toward a Simplified Microfluidic Device for Ultra-fast Genetic Analysis with Sample-In/Answer-Out Capability: Application to T-Cell Lymphoma Diagnosis. J Assoc Laboratory Automation 13:351–360
Diercks AH et al (2009) A microfluidic device for multiplexed protein detection in nano-liter volumes. Anal Biochem 386:30–35
Lin DH et al (2010) Internally calibrated quantification of VEGF in human plasma by fluorescence immunoassays in disposable elastomeric microfluidic devices. J Chromatogr B 878:258–263
Lee H et al (2008) Chip–NMR biosensor for detection and molecular analysis of cells. Nat Med 14:869–874
Lazar IM (2008) Microfluidic bioanalytical platforms with mass spectrometry detection for biomarker discovery and screening In: Severine le Gac, Albert van den Berg (eds) Miniaturization and Mass Spectrometry, Royal Society of Chemistry, 1st ed., pp 151–172
Zhang K et al (2010) A microfluidic system with surface modified piezoelectric sensor for trapping and detection of cancer cells. Biosens Bioelectron 26(2):935–939
von Muhlen MG et al (2010) Label-free biomarker sensing in undiluted serum with suspended microchannel resonators. Anal Chem 82:1905–1910
Zani A et al (2011) A New Electrochemical Multiplexed Assay for PSA Cancer Marker Detection. Electroanalysis 23:91–99
Fragoso A et al (2010) Integrated microfluidic platform for the electrochemical detection of breast cancer markers in patient serum samples. Lab Chip 11(4):625–631
Kellner C et al (2011) Automated microsystem for electrochemical detection of cancer markers. Electrophoresis 32:926–930
O’Sullivan A et al (2011) Cost Estimation of Cardiovascular Disease Events in the US. Pharmacoeconomics 29(8):693–704
McDonnell B et al (2009) Cardiac biomarkers and the case for point-of-care testing. Clin Biochem 42:549–561
Mohammed MI, Desmulliez MPY (2010) Lab-on-a-chip based immunosensor principles and technologies for the detection of cardiac biomarkers: a review. Lab Chip 11(4):569–595
Wu AHB et al (2004) Evaluation of a point-of-care assay for cardiac markers for patients suspected of acute myocardial infarction. Clin Chim Acta 346:211–219
Ordonez-Llanos J et al (2006) Risk stratification of chest pain patients by point-of-care cardiac troponin T and myoglobin measured in the emergency department. Clin Chim Acta 365:93–97
James SK et al (2004) A rapid troponin I assay is not optimal for determination of troponin status and prediction of subsequent cardiac events at suspicion of unstable coronary syndromes. Int J Cardiol 93:113–120
Cramer GE et al (2007) Lack of concordance between a rapid bedside and conventional laboratory method of cardiac troponin testing: impact on risk stratification of patients suspected of acute coronary syndrome. Clin Chim Acta 381:164–166
Jönsson C et al (2008) Silane–dextran chemistry on lateral flow polymer chips for immunoassays. Lab Chip 8:1191–1197
Gervais L, Delamarche E (2009) Toward one-step point-of-care immunodiagnostics using capillary-driven microfluidics and PDMS substrates. Lab Chip 9:3330–3337
Hong B et al (2008) Highly sensitive rapid, reliable, and automatic cardiovascular disease diagnosis with nanoparticle fluorescence enhancer and MEMS. Adv Exp Med Biol 614:265–273
Bhattacharyya A, Klapperich CM (2007) Design and testing of a disposable microfluidic chemiluminescent immunoassay for disease biomarkers in human serum samples. Biomed Microdevices 9:245–251
Cho IH et al (2009) Chemiluminometric enzyme-linked immunosorbent assays (ELISA)-on-a-chip biosensor based on cross-flow chromatography. Anal Chim Acta 632:247–255
Huang H et al (2009) Rapid analysis of alpha-fetoprotein by chemiluminescence microfluidic immunoassay system based on super-paramagnetic microbeads. Biomed Microdevices 11:213–216
Sista R et al (2008) Development of a digital microfluidic platform for point of care testing. Lab Chip 8:2091–2104
Kurita R et al (2006) On-chip enzyme immunoassay of a cardiac marker using a microfluidic device combined with a portable surface plasmon resonance system. Anal Chem 78:5525–5531
Tweedie M et al (2006) Fabrication of impedimetric sensors for label-free Point-of-Care immunoassay cardiac marker systems, with passive microfluidic delivery. IEEE 1:4610–4614
Christenson RH, Azzazy HME (2009) Cardiac point of care testing: a focused review of current National Academy of Clinical Biochemistry guidelines and measurement platforms. Clin Biochem 42:150–157
Billah M, Hays HCW, Millner PA (2008) Development of a myoglobin impedimetric immunosensor based on mixed self-assembled monolayer onto gold. Microchimica Acta 160:447–454
Zhou F et al (2010) Electrochemical Immunosensor for Simultaneous Detection of Dual Cardiac Markers Based on a Poly (Dimethylsiloxane)-Gold Nanoparticles Composite Microfluidic Chip: A Proof of Principle. Clin Chem 56:1701–1707
Chen X et al (2008) Electrochemical impedance immunosensor based on three-dimensionally ordered macroporous gold film. Anal Chem 80:2133–2140
Mitsakakis K, Gizeli E (2011) Detection of multiple cardiac markers with an integrated acoustic platform for cardiovascular risk assessment. Anal Chim Acta 699(1):1–5
Hong J, Edel JB, deMello AJ (2009) Micro-and nanofluidic systems for high-throughput biological screening. Drug Discov Today 14:134–146
Liu J et al (2009) In Situ Microarray Fabrication and Analysis Using a Microfluidic Flow Cell Array Integrated with Surface Plasmon Resonance Microscopy. Anal Chem 81:4296–4301
Caliper LifeSciences-Target ID/Validation Applications. http://www.perkinelmer.com/industries/lifesciencesresearch/default.xhtml. Accessed 26 May 2011
The FilmArray Respiratory Panel. http://www.biofiredx.com/FilmArray/RespiratoryTest.html Accessed 12 Nov 2012.
(2011) search issued patents for “microfluidic” in title or abstract, United States Patent and Trademark office.
Mark D et al (2010) Microfluidic lab-on-a-chip platforms: requirements, characteristics and applications. Chem Soc Rev 39:1153–1182
Becker H (2009) It’s the economy. Lab Chip 9:2759–2762
Kim L (2011) FluidicMEMS.com’s list of microfluidics/lab-on-a-chip companies. http://fluidicmems.com/list-of-microfluidics-lab-on-a-chip-and-biomems-companies.Accessed 12 Nov 2012
Acknowledgments
The authors thank Keng-Min Lin for the schematic diagram in Fig. 1. The authors would like to thank the Nano Institute of Utah for funding this work through a nanotechnology training fellowship.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media,LLC
About this protocol
Cite this protocol
Jayamohan, H., Sant, H.J., Gale, B.K. (2013). Applications of Microfluidics for Molecular Diagnostics. In: Jenkins, G., Mansfield, C. (eds) Microfluidic Diagnostics. Methods in Molecular Biology, vol 949. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-134-9_20
Download citation
DOI: https://doi.org/10.1007/978-1-62703-134-9_20
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-133-2
Online ISBN: 978-1-62703-134-9
eBook Packages: Springer Protocols