
Abstract
Purpose
Optimal antimicrobial treatment duration for Gram-negative bloodstream infection (BSI) remains unclear. This retrospective cohort study examined effectiveness of short (7–10 days) and long (>10 days) courses of antimicrobial therapy for uncomplicated Gram-negative BSI.
Methods
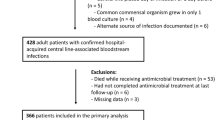
Hospitalized adults with uncomplicated Gram-negative BSI at Palmetto Health hospitals in Columbia SC, USA from January 1, 2010 to December 31, 2013 were identified. Multivariate Cox proportional hazards regression with propensity score adjustment was used to examine risk of treatment failure in the two groups.
Results
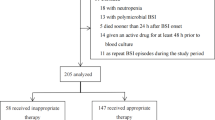
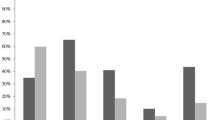
During the study period, 117 and 294 patients received short and long courses of antimicrobial therapy for uncomplicated Gram-negative BSI, respectively. Overall, the median age was 67 years, 258 (63%) were women, 282 (69%) had urinary source of infection, and 271 (66%) had BSI due to Escherichia coli. The median duration of antimicrobial therapy was 8.5 and 13.3 days in the short and long treatment groups, respectively. After adjustment for the propensity to use a short course of therapy, risk of treatment failure was higher in patients receiving short compared to long courses of antimicrobial agents (HR 2.60, 95% CI: 1.20–5.53, p = 0.02). Other risk factors for treatment failure included liver cirrhosis (HR 5.83, 95% CI: 1.89–15.02, p = 0.004) and immune compromised status (HR 4.30, 95% CI: 1.57–10.80, p = 0.006). Definitive antimicrobial therapy with intravenous or highly bioavailable oral agents was associated with reduced risk of treatment failure (HR 0.33, 95% CI: 0.14–0.73, p = 0.006).
Conclusions
The current results support common clinical practice of 2 weeks of antimicrobial therapy for uncomplicated Gram-negative BSI.

Similar content being viewed by others
References
Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19:501–9.
Uslan DZ, Crane SJ, Steckelberg JM, Cockerill FR 3rd, St Sauver JL, Wilson WR, Baddour LM. Age-and sex-associated trends in bloodstream infection. Arch Intern Med. 2007;167:834–9.
Bryan CS, Reynolds KL, Brenner ER. Analysis of 1186 episodes of Gram-negative bacteremia in non-university hospital: the effects of anti-microbial therapy. Rev Infect Dis. 1983;5:629–38.
Retamar P, Portillo MM, López-Prieto MD, Rodríguez-López F, de Cueto M, García MV, Gómez MJ, Del Arco A, Muñoz A, Sánchez-Porto A, Torres-Tortosa M, Martín-Aspas A, Arroyo A, García-Figueras C, Acosta F, Corzo JE, León-Ruiz L, Escobar-Lara T, Rodríguez-Baño J. SAEI/SAMPAC Bacteremia Group. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother. 2012;56:472–8.
Cain SE, Kohn J, Bookstaver PB, Albrecht H, Al-Hasan MN. Stratification of the impact of inappropriate empirical antimicrobial therapy for gram-negative bloodstream infections by predicted prognosis. Antimicrob Agents Chemother. 2015;59:245–50.
Shorr AF, Micek ST, Welch EC, Doherty JA, Reichley RM, Kollef MH. Inappropriate antibiotic therapy in Gram-negative sepsis increases hospital length of stay. Crit Car Med. 2011;39:46–51.
Battle SE, Bookstaver PB, Justo JA, Kohn J, Albrecht H, Al-Hasan MN. Association between inappropriate empirical antimicrobial therapy and hospital length of stay in gram-negative bloodstream infections: stratification by prognosis. J Antimicrob Chemother. 2017;72:299–304.
Wendt C, Messer SA, Hollis RJ, Pfaller MA, Wenzel RP, Herwaldt LA. Recurrent gram-negative bacteremia: incidence and clinical patterns. Clin Infect Dis. 1999;28:611–7.
Al-Hasan MN, Eckel-Passow JE, Baddour LM. Recurrent gram-negative bloodstream infection: a 10-year population-based cohort study. J Infect. 2010;61:28–33.
Nielsen SL, Lassen AT, Gradel KO, Jensen TG, Kolmos HJ, Hallas J, Pedersen C. Bacteremia is associated with excess long-term mortality: a 12-year population-based cohort study. J Infect. 2015;70:111–26.
Al-Hasan MN, Juhn YJ, Bang DW, Yang HJ, Baddour LM. External validation of Gram-negative bloodstream infection mortality risk score in a population-based cohort. Clin Microbiol Infect. 2014;20:886–91.
Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP, Raad II, Rijnders BJ, Sherertz RJ, Warren DK. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Disease Society of America. Clin Infect Dis. 2009;49:1–45.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–32.
Friedman ND, Kaye KS, Stout JE, McGarry SA, Trivette SL, Briggs JP, Lamm W, Clark C, MacFarquhar J, Walton AL, Reller LB, Sexton DJ. Health-care associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791–7.
Grayson ML, Crowe SM, McCarthy S, Mills J, Mouton JW, Norrby SR, Paterson DL, Pfaller MA. Kucers’: the use of antibiotics. 6th ed. London: CRC Press; 2010.
Kutob LF, Justo JA, Bookstaver PB, Kohn J, Albrecht H, Al-Hasan MN. Effectiveness of oral antibiotics for definitive therapy of Gram-negative bloodstream infections. Int J Antimicrob Agents. 2016;48:498–503.
Holland TL, Arnold C, Fowler VG. Clinical management of Staphylococcus aureus bacteremia: a review. JAMA. 2014;312:1330–41.
Chong YP, Moon SM, Bang KM, Park HJ, Park SY, Kim MN, Park KH, Kim SH, Lee SO, Choi SH, Jeong JY, Woo JH, Kim YS. Treatment duration for uncomplicated Staphylococcus aureus bacteremia to prevent relapse. Antimicrob Agents Chemother. 2013;57:1150–6.
López-Cortés LE, Del Toro MD, Gálvez-Acebal J, Bereciartua-Bastarrica E, Fariñas MC, Sanz-Franco M, Natera C, Corzo JE, Lomas JM, Pasquau J, Del Arco A, Martínez MP, Romero A, Muniain MA, de Cueto M, Pascual A, Rodríguez-Baño J. REIPI/SAB group. Impact of an evidence-based bundle intervention in the quality-of-care management and outcome of Staphylococcus aureus bacteremia. Clin Infect Dis. 2013;57:1225–33.
Havey TC, Fowler RA, Daneman N. Duration of antibiotic therapy for bacteremia: a systematic review and meta-analysis. Crit Care. 2011;15:R267.
Chowdhary G, Dutta S, Narang A. Randomized controlled trial of 7-day vs. 14-day antibiotics for neonatal sepsis. J Trop Pediatr. 2006;52:427–32.
Park SH, Milstone AM, Diener-West M, Nussenblatt V, Cosgrove SE, Tamma PD. Short versus prolonged courses of antibiotic therapy for children with uncomplicated Gram-negative bacteraemia. J Antimicrob Chemother. 2013;69:779–85.
Daneman N, Rishu AH, Xiong W, Bagshaw SM, Dodek P, Hall R, Kumar A, Lamontagne F, Lauzier F, Marshall J, Martin CM, McIntyre L, Muscedere J, Reynolds S, Stelfox HT, Cook DJ, Fowler RA, Canadian Critical Care Trials Group. Duration of antimicrobial treatment for bacteremia in canadian critically Ill patients. Crit Care Med. 2016;44:256–64.
Cheng CH, Tsau YK, Lin TY. Effective duration of antimicrobial therapy for the treatment of acute lobar nephronia. Pediatrics. 2006;117:e84–9.
Sandberg T, Skoog G, Hermansson AB, Kahlmeter G, Kuylenstierna N, Lannergård A, Otto G, Settergren B, Ekman GS. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: a randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Lancet. 2012;380:484–90.
Eliakim-Raz N, Yahav D, Paul M, Leibovici L. Duration of antibiotic treatment for acute pyelonephritis and septic urinary tract infection- 7 days or less versus longer treatment: systematic review and meta-analysis of randomized controlled trials. J Antimicrob Chemother. 2013;68:2183–91.
Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, Moran GJ, Nicolle LE, Raz R, Schaeffer AJ, Soper DE. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52:e103–20.
Acknowledgements
The authors thank the Palmetto Health Antimicrobial Stewardship and Support Team in South Carolina, USA for their help in facilitating the conduction of this study. The preliminary results of this study were presented in part at IDWeek annual meeting in October 26-30, 2016; New Orleans, LA, USA (Abstract # 59811). ANN and MNA have full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the analysis.
Funding
ANN received funding from the Medical Scholars Program 2016 of the Infectious Disease Society of America Education and Research Foundation. Funding source had no role in study design. The study had no other sources of funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
ANN, JAJ, JK and HA: No conflicts. PBB and MNA: Continuous medical education steering committee for Rockpointe Corporation, Columbia, MD, USA.
Rights and permissions
About this article

Cite this article
Nelson, A.N., Justo, J.A., Bookstaver, P.B. et al. Optimal duration of antimicrobial therapy for uncomplicated Gram-negative bloodstream infections. Infection 45, 613–620 (2017). https://doi.org/10.1007/s15010-017-1020-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-017-1020-5