
Abstract
Background
Remission of type 2 diabetes (T2D) is a desired outcome after bariatric surgery (BS). Even if this goal is not achieved, individuals who do not strictly fulfill remission criteria experience an overall improvement. The aim of this study was to evaluate the metabolic control status in patients considered as diabetes “non-remitters.”
Methods
A retrospective study of 125 patients (59.2 % women) with preoperative diagnosis of T2D who underwent BS in a single center (2006–2011) was conducted. We collected anthropometric and metabolic parameters before surgery and at 1-year follow-up. T2D remission was defined according to the 2009 consensus statement: glycosylated hemoglobin (HbA1c) <6 %, fasting glucose (FG) <100 mg/dLs, and absence of pharmacologic treatment. We evaluated metabolic status of non-remitters, according to the American Diabetes Association's (ADA) target recommendations: HbA1c <7 %, LDL-c <100 mg/dL, triglycerides <150 mg/dL, and HDL-c >40 (male) or >50 mg/dL (female). Statistics: analysis of variance.
Results
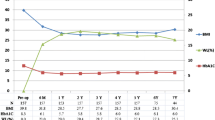
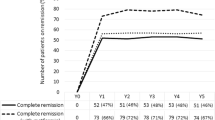
Baseline characteristics (mean ± SD): age 53.5 ± 9.7 years, BMI 43.5 ± 5.6 kg/m2, time since diagnosis of T2D 7.7 ± 7.9 years, FG 162.0 ± 56.3 mg/dL, HbA1c 7.7 ± 1.6 %. ADA's target recommendations were present in 12 patients (9.6 %) preoperatively, and in 45 (36.0 %) at 1-year follow-up (p <0.001). Sixty-two (49.6 %) patients did not achieve diabetes remission; 26 (41.9 %) had now diet treatment, 30 (48.4 %) oral medications, and 6 (9.7 %) required insulin. Of the non-remitters, 57 (91.9 %) had HbA1c <7 % and 18 (40.0 %) achieved ADA's target recommendations. There were no differences between remitters and non-remitters in the number of individuals reaching ADA's combined metabolic control.
Conclusions
Although almost 50 % of the patients may not be classified as diabetes remitters, their significant improvement in metabolic control should be regarded as a success, according to most scientific societies' target recommendations.

Similar content being viewed by others

References
Dixon JB, O'Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–23.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:248–56.
Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–85.
Schauer P, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Eng J Med. 2012;366:1567–76.
Blackstone R, Bunt JC, Cortés MC, et al. Type 2 diabetes after gastric bypass: remission in five models using HbA1c, fasting blood glucose, and medication status. Surg Obes Relat Dis. 2012;8:548–55.
Ramos-Levi AM, Cabrerizo L, Matía P, et al. Which criteria should be used to define type 2 diabetes remission after bariatric surgery? BMC Surg. 2013;13:8.
Buse JB, Caprio S, Cefalu WT, et al. How do we define cure of diabetes? Diabetes Care. 2009;32:2133–5.
Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93.
Keogh JB, Turner KM, McDonald F, et al. Remission of diabetes in patients with long-standing type 2 diabetes following placement of adjustable gastric band: a retrospective case control study. Diabetes Obes Metab. 2012. doi:10.1111/dom.12034.
Dorman RB, Serrot FJ, Miller CJ, et al. Case-matched outcomes in bariatric surgery for treatment of type 2 diabetes in the morbidly obese patient. Ann Surg. 2012;255:287–93.
Kashyap SR, Schauer P. Clinical considerations for the management of residual diabetes following bariatric surgery. Diabetes Obes Metab. 2012;14:733–79.
Chikunguwo SM, Wolfe LG, Dodson P, et al. Analysis of factors associated with durable diabetes remission of diabetes after Roux –en-Y gastric bypass. Surg Obes Relat Dis. 2010;6:254–9.
American Diabetes Association. Position Statement. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36 suppl 1:S67–74.
Deitel M, Greenstein RJ. Recommendations for reporting weight loss. Obes Surg. 2003;13:159–60.
Hess DS, Hess DW. Biliopancreatic diversion with a duodenal switch. Obes Surg. 1998;8:267–82.
Sánchez-Pernaute A, Rubio Herrera MA, Pérez-Aguirre E, et al. Proximal duodenal-ileal end-to-side bypass with sleeve gastrectomy: proposed technique. Obes Surg. 2007;17:1614–8.
American Diabetes Association. Standards of medical care in diabetes 2013 (position statement). Diabetes Care. 2013;36 suppl 1:S11–66.
Pournaras DJ, Aasheim ET, Søvik TT, et al. Effect of the definition of type II diabetes remission in the evaluation of bariatric surgery for metabolic disorders. Br J Surg. 2012;99:100–3.
Ramos-Levi AM, Sánchez-Pernaute A, Matía P, et al. Rubio MA. Obes Surg: Diagnosis of diabetes remission after bariatric surgery may be jeopardized by remission criteria and previous hypoglycemic treatment; 2013. doi:10.1007/s11695-013-0995-y.
Schauer PR, Burguera B, Ikramuddin S, et al. Effect of laparoscopic Roux-en-Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003;238:467–85.
Dixon JB, Chuang LM, Chong K, et al. Predicting the glycemic response to gastric bypass surgery in patients with type 2 diabetes. Diabetes Care. 2013;36:20–6.
Hall TC, Pellen MG, Sedman PC, et al. Preoperative factors predicting remission of type 2 diabetes mellitus after Roux-en-Y gastric bypass surgery for obesity. Obes Surg. 2010;20:1245–50.
Pories WJ, Swanson MS, MacDonald KG, et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995;222:339–50. discussion 350–2.
Rubino F, Schauer PR, Kaplan LM, et al. Metabolic surgery to treat type 2 diabetes: clinical outcomes and mechanisms of action. Annu Rev Med. 2010;61:393–411.
Lecube A, Burgera B, Rubio MA. Breaking therapeutic inertia: should metabolic surgery be considered one more option for the treatment of type 2 diabetes mellitus? Endocrinol Nutr. 2012;59:281–3.
Zimmet P, Alberti KG, Rubino F, et al. IDF's view of bariatric surgery in type 2 diabetes. Lance. 2011;378:108–10.
Dixon JB, Zimmet P, Alberti KG, et al. Bariatric surgery: an IDF statement for obese type 2 diabetes. Diabet Med. 2011;28:628–42.
Deitel M. Update: why diabetes does not resolve in some patients after bariatric surgery. Obes Surg. 2011;21:794–6.
Acknowledgments
The authors would like to acknowledge grant support from the Fundación Mutua Madrileña de Investigación Biomédica AP 89592011.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ramos-Levi, A.M., Sanchez-Pernaute, A., Cabrerizo, L. et al. Remission of Type 2 Diabetes Mellitus Should Not Be the Foremost Goal after Bariatric Surgery. OBES SURG 23, 2020–2025 (2013). https://doi.org/10.1007/s11695-013-1032-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-013-1032-x