
Abstract
Summary
There is a paucity of normative bone mineral density (BMD) data in healthy African women. Baseline total hip and lumbar spine BMD was measured in premenopausal women. BMD distribution was comparable to that of a reference population and was impacted by several factors including contraception and duration of lactation.
Introduction
Normative data on bone mineral density (BMD) and the cumulative impact of lactation, contraceptive use, and other factors on BMD in healthy African women have not been well studied.
Objectives
The objective of this study was to determine the factors associated with BMD in healthy premenopausal women in Uganda and Zimbabwe.
Methods
Baseline total hip (TH) and lumbar spine (LS) BMD was measured by dual x-ray absorptiometry in 518 healthy, premenopausal black women enrolling in VOICE, an HIV-1 chemoprevention trial, at sites in Uganda and Zimbabwe. Contraceptive and lactation histories, physical activity assessment, calcium intake, and serum vitamin D levels were assessed. Independent factors associated with BMD were identified using an analysis of covariance model.
Results
The study enrolled 331 women from Zimbabwe and 187 women from Uganda. Median age was 29 years (IQR 25, 32) and median body mass index (BMI) was 24.8 kg/m2 (IQR 22.2, 28.6). In univariate analyses, lower TH BMD values were associated with residence in Uganda (p < 0.001), lower BMI (p < 0.001), and any use of and duration of depot-medroxyprogresterone acetate. Use of oral contraceptives, progestin-only implants, and higher physical activity levels were protective against reduced BMD. Similarly, lower LS BMD values were associated with these same factors but also higher parity and history of breastfeeding. In a multivariable analysis, lower TH and LS BMD values were associated with enrollment in Uganda, lower BMI, and lower physical activity level; contraceptive use was associated with lower spine BMD, and breastfeeding contributed to lower total hip BMD.
Conclusions
Among healthy premenopausal women, TH and LS BMD was higher in Zimbabwe than Uganda. Additional factors independently associated with BMD included BMI, physical activity level, contraceptive use, and lactation.

Similar content being viewed by others

References
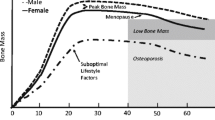
Matkovic V, Jelic T, Wardlaw GM, Ilich JZ, Goel PK, Wright JK et al (1994) Timing of peak bone mass in Caucasian females and its implication for the prevention of osteoporosis. Inference from a cross-sectional model. J Clin Invest 93(2):799–808
Berger C, Goltzman D, Langsetmo L, Joseph L, Jackson S, Kreiger N et al (2010) Peak bone mass from longitudinal data: implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J Bone Miner Res 25(9):1948–1957
IQ Solutions I. Osteoporosis: peak bone mass in women [Internet]. Available from: http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/bone_mass.asp. Accessed 28 Aug 2014
Karlsson C, Obrant KJ, Karlsson M (2001) Pregnancy and lactation confer reversible bone loss in humans. Osteoporos Int 12(10):828–834
Chantler S, Dickie K, Goedecke JH, Levitt NS, Lambert EV, Evans J et al (2012) Site-specific differences in bone mineral density in black and white premenopausal South African women. Osteoporos Int 23(2):533–542
Petitti DB, Piaggio G, Mehta S, Cravioto MC, Meirik O (2000) Steroid hormone contraception and bone mineral density: a cross-sectional study in an international population. The WHO study of hormonal contraception and bone health. Obstet Gynecol 95(5):736–744
Cundy T, Cornish J, Evans MC, Roberts H, Reid IR (1994) Recovery of bone density in women who stop using medroxyprogesterone acetate. BMJ 308(6923):247–248
Banks E, Berrington A, Casabonne D (2001) Overview of the relationship between use of progestogen-only contraceptives and bone mineral density. BJOG Int J Obstet Gynaecol 108(12):1214–1221
Kasonde M, Niska RW, Rose C, Henderson FL, Segolodi TM, Turner K, et al. (2014) Bone mineral density changes among HIV-uninfected young adults in a randomised trial of pre-exposure prophylaxis with tenofovir-emtricitabine or placebo in Botswana. PLoS ONE 13;9(3):e90111
Ettinger B, Sidney S, Cummings SR, Libanati C (first), Bikle DD, Tekawa IS, et al. Racial differences in bone density between young adult black and white subjects persist after adjustment for anthropometric, lifestyle, and biochemical differences. J Clin Endocrinol Metabol 82(2): 429–434
Scholes D et al (2005) Change in bone mineral density among adolescent women using and discontinuing depot medroxyprogesterone acetate contraception. Arch Pediatr Adolesc Med 159:139–144
Nelson DA, Pettifor JM, Barondess DA, Cody DD, Uusi-Rasi K, Beck TJ (2004) Comparison of cross-sectional geometry of the proximal femur in white and black women from Detroit and Johannesburg. J Bone Miner Res 19(4):560–565
Lloyd R, Hind K, Micklesfield A, Lisa K, Sean C, Truscott JG, Parr B et al (2010) A pilot investigation of load-carrying on the head and bone mineral density in premenopausal, black African women. J Bone Miner Metab 28:185–190
Finkelstein JS, Lee M-LT, Sowers M, Ettinger B, Neer RM, Kelsey JL et al (2002) Ethnic variation in bone density in premenopausal and early perimenopausal women: effects of anthropometric and lifestyle factors. J Clin Endocrinol Metab 87(7):3057–3067
Cleland JG, Ndugwa RP, Zulu EM (2011) Family planning in sub-Saharan Africa: progress or stagnation? Bull World Health Organ 89(2):137–143
The World Bank (2011). Unmet need for contraception [Internet]. The World Bank. Available from: http://go.worldbank.org/PCDPQW7Y70. Accessed 28 Aug 2014
Marrazzo J et al (2015). Tenofovir-Based Preexposure Prophylaxis for HIV Infection among African Women. N Engl J Med 372:509–518. doi:10.1056/NEJMoa1402269
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE et al (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35(8):1381–1395
Kanis JA, Adachi JD, Cooper C, Clark P, Cummings SR, Diaz-Curiel M et al (2013) Standardising the descriptive epidemiology of osteoporosis: recommendations from the epidemiology and quality of life working group of IOF. Osteoporos Int 24(11):2763–2764
Kaunitz A, Miller P, Rice V, Ross D, McClung M (2006) Bone mineral density in women aged 25–35 years receiving depot medroxyprogesterone acetate: recovery following discontinuation. Contraception 74(2):90–99
Rahman M, Berenson AB (2010) Predictors of higher bone mineral density loss and use of depot medroxyprogesterone acetate. Obstet Gynecol 115(1):35–40
Naessen T, Olsson SE, Gudmundson J (1995) Differential effects on bone density of progestogen-only methods for contraception in premenopausal women. Contraception 52(1):35–39
Di X, Li Y, Zhang C, Jiang J, Gu S (1999) Effects of levonorgestrel-releasing subdermal contraceptive implants on bone density and bone metabolism. Contraception 60(3):161–166
Beerthuizen R, van Beek A, Massai R, Mäkäräinen L, Hout J, Bennink HC (2000) Bone mineral density during long-term use of the progestagen contraceptive implant Implanon compared to a non-hormonal method of contraception. Hum Reprod Oxf Engl 15(1):118–122
Díaz S, Reyes MV, Zepeda A, González GB, López JM, Campino C et al (1999) Norplant((R)) implants and progesterone vaginal rings do not affect maternal bone turnover and density during lactation and after weaning. Hum Reprod Oxf Engl 14(10):2499–2505
Polatti F, Perotti F, Filippa N, Gallina D, Nappi RE (1995) Bone mass and long-term monophasic oral contraceptive treatment in young women. Contraception 51(4):221–224
Mehta S (1993) Bone loss, contraception and lactation. Acta Obstet Gynecol Scand 72(3):148–156
Holbrook TL, Barrett-Connor E (1991) Calcium intake: covariates and confounders. Am J Clin Nutr 53(3):741–744
Acknowledgments
We are grateful to the research participants for their participation in our study. We would also like to thank the Microbicide Trials Network (MTN)-003B Protocol Team, the MTN-003 (VOICE) protocol team, and the UZ-UCSF and MU-JHU research site teams for sample and data collection as well as SCHARP, our data management center. We acknowledge Karen B. Patterson for her dedication in quality control of the scans and other study data. This work would not have been possible without the support of staff of the Osteoporosis Research Center at the University of Pittsburgh.
Funding
The Microbicide Trials Network is funded by the National Institute of Allergy and Infectious Diseases (UM1AI068633, UM1AI068615, UM1AI106707), with co-funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institute of Mental Health, all components of the US National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Visit www.mtnstopshiv.org.
UZ-UCSF Clinical Trials Unit Grant Number - UM1 AI 0694361 I
MU-JHU Clinical Trials Unit Grant Number - UM1 AI069530
Conflicts of interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Sources of Funding: NIAID (5UM1AI068633), NICHD, and NIMH, all of the US National Institutes of Health.
Rights and permissions
About this article

Cite this article
Mgodi, N.M., Kelly, C., Gati, B. et al. Factors associated with bone mineral density in healthy African women. Arch Osteoporos 10, 3 (2015). https://doi.org/10.1007/s11657-015-0206-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-015-0206-7