
Abstract
Summary
There is a wide variation in fracture probabilities estimated by Asian FRAX models, although the outputs of South Asian models are concordant. Clinicians can choose either fixed or age-specific intervention thresholds when making treatment decisions in postmenopausal women. Cost-effectiveness of such approach, however, needs to be addressed.
Purpose
This study examined suitable fracture probability intervention thresholds (ITs) for Sri Lanka, based on the Sri Lankan FRAX model.
Methods
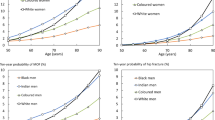
Fracture probabilities were estimated using all Asian FRAX models for a postmenopausal woman of BMI 25 kg/m2 and has no clinical risk factors apart from a fragility fracture, and they were compared. Age-specific ITs were estimated based on the Sri Lankan FRAX model using the method followed by the National Osteoporosis Guideline Group in the UK. Using the age-specific ITs as the reference standard, suitable fixed ITs were also estimated.
Results
Fracture probabilities estimated by different Asian FRAX models varied widely. Japanese and Taiwan models showed higher fracture probabilities while Chinese, Philippine, and Indonesian models gave lower fracture probabilities. Output of remaining FRAX models were generally similar. Age-specific ITs of major osteoporotic fracture probabilities (MOFP) based on the Sri Lankan FRAX model varied from 2.6 to 18 % between 50 and 90 years. ITs of hip fracture probabilities (HFP) varied from 0.4 to 6.5 % between 50 and 90 years. In finding fixed ITs, MOFP of 11 % and HFP of 3.5 % gave the lowest misclassification and highest agreement.
Conclusion
Sri Lankan FRAX model behaves similar to other Asian FRAX models such as Indian, Singapore-Indian, Thai, and South Korean. Clinicians may use either the fixed or age-specific ITs in making therapeutic decisions in postmenopausal women. The economical aspects of such decisions, however, need to be considered.



Similar content being viewed by others


References
Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 15(11):897–902
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM, Melton LJ, Cummings SR, Kanis JA (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22(5):1277–1288
Mithal A, Dhingra V, Lau E, Stenmark J, Nauroy L (2009) The Asian Audit: epidemiology, costs and burden of osteoporosis in Asia 2009. International Osteoporosis Foundation. www.iofbonehealth.org/asian audit. Accessed 1 June 2013
www.shef.ac.uk/FRAX/pdfs/FRAX_Release_Notes.pdf. Accessed 1 June 2013
National Osteoporosis Guideline Group (2008) Case finding for the management of osteoporosis with FRAX—assessment and intervention thresholds for the UK. Osteoporos Int 19(10):1395–1408
National Osteoporosis Foundation (2013) Clinician’s guide to prevention and treatment of osteoporosis. National Osteoporosis Foundation, Washington, DC
Lee DY, Lim SJ, Moon YW, Min YK (2010) Determination of an applicable FRAX model in Korean women. J Korean Med Sci 25(11):1657–1660
Korthoewer D, Chandran M (2012) Osteoporosis management and the utilization of FRAX: a survey amongst health care professionals of the Asia-Pacific. Arch Osteoporos 7(1–2):193–200
Fujiwara S, Nakamura T, Orimo H, Hosoi T, Gorai I, Oden A, Johansson H, Kanis JA (2008) Development and application of a Japanese model of the WHO fracture risk assessment tool (FRAX). Osteoporos Int 19(4):429–435
Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A (2008) Case finding for the management of osteoporosis with FRAX—assessment and intervention thresholds for the UK. Osteoporos Int 19(10):1395–1408
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lekamwasam, S. Sri Lankan FRAX model and country-specific intervention thresholds. Arch Osteoporos 8, 148 (2013). https://doi.org/10.1007/s11657-013-0148-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-013-0148-x