
Abstract
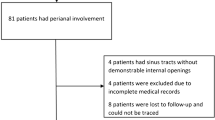
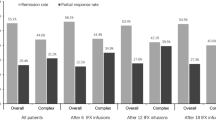
Perianal fistulizing Crohn’s disease (PFCD) treatment is based on fistula drainage, antibiotics, immunosuppressant (IS) drugs, and infliximab. Our aim was to study the effectiveness of combination therapy on PFCD and to search for clinical or imaging features associated with the initial complete clinical response and its stability overtime. Patients and methods All patients with PFCD treated in our tertiary center between 2000 and 2005 by infliximab in combination with seton placement and/or IS and evaluated by MRI before treatment were included in the study. Basal clinical and MRI characteristics were recorded. Response to treatment was evaluated after the infliximab induction regiment and at the end of the follow-up. Results Twenty-six patients were included and followed-up for an average 4.9 years. A complex fistula was present in 69% (18/26 patients) of cases and eight (8/26 patients) had an ano-vaginal fistula. After infliximab induction therapy, 13 patients (50%) achieved a complete clinical response. The initial clinical response was significantly associated with the absence of both, active intestinal disease (54% vs. 8%, P = 0.03) and active proctitis (77% vs. 23%, P = 0.01). No initial MRI characteristics were linked to the initial response. In multivariate analysis, only the presence of active proctitis was associated with the lack of response (P = 0.047). At the end of the follow-up, 42% of the patients remained in clinical remission. No clinical characteristics were associated to sustained response when among long-standing responders two exhibited a normal post-treatment MRI. Conclusion An initial complete response of PFCD was observed in half of the patients after combined therapy including infliximab that decreased to 42% later on. Complete healing of fistulas on MRI was possible but unusual. The initial response seemed related to the absence of active intestinal disease, especially in the rectum, when the long-term response could not be predicted by the basal characteristics of patients.
Similar content being viewed by others

References
Beaugerie L, Seksik P, Nion-Larmurier I, Gendre JP, Cosnes J. Predictors of Crohn’s disease. Gastroenterology. 2006;130:650–656. doi:10.1053/j.gastro.2005.12.019.
Gower-Rousseau C, Salomez JL, Dupas JL, et al. Incidence of inflammatory bowel disease in northern France (1988–1990). Gut. 1994;35:1433–1438. doi:10.1136/gut.35.10.1433.
Molinie F, Gower-Rousseau C, Yzet T, et al. Opposite evolution in incidence of Crohn’s disease and ulcerative colitis in Northern France (1988–1999). Gut. 2004;53:843–848. doi:10.1136/gut.2003.025346.
Singh B, Mc C, Mortensen NJ, Jewell DP, George B. Perianal Crohn’s disease. Br J Surg. 2004;91:801–814. doi:10.1002/bjs.4613.
Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med. 1999;340:1398–1405. doi:10.1056/NEJM199905063401804.
Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350:876–885. doi:10.1056/NEJMoa030815.
Ouraghi A, Nieuviarts S, Mougenel JL, et al. Infliximab therapy for Crohn’s disease anoperineal lesions. Gastroenterol Clin Biol. 2001;25:949–956.
Lichtenstein G, Yan S, Bala M, Blank M, Sands BE. Infliximab maintenance treatment reduces hospitalizations, surgeries, and procedures in fistulizing Crohn’s disease. Gastroenterology. 2005;128:862–869. doi:10.1053/j.gastro.2005.01.048.
West RL, van der Woude CJ, Hansen BE, et al. Clinical and endosonographic effect of ciprofloxacin on the treatment of perianal fistulae in Crohn’s disease with infliximab: a double-blind placebo-controlled study. Aliment Pharmacol Ther. 2004;20:1329–1336. doi:10.1111/j.1365-2036.2004.02247.x.
Hyder SA, Travis S, Jewell D, Mortensen N, George B. Fistulating anal Crohn’s disease: results of combined surgical and infliximab treatment. Dis Colon Rectum. 2006;49:1837–1841. doi:10.1007/s10350-006-0656-5.
Schwartz DA, Herdman CR. Review article: the medical treatment of Crohn’s perianal fistulas. Aliment Pharmacol Ther. 2004;19:953–967. doi:10.1111/j.1365-2036.2004.01917.x.
Ochsenkuhn T, Goke B, Sackmann M. Combining infliximab with 6-mercaptopurine/azathioprine for fistula therapy in Crohn’s disease. Am J Gastroenterol. 2002;97:2022–2025.
Schroder O, Blumenstein A, Schulte-Bockholt A, Stein J. Combining infliximab and methotrexate in fistulizing Crohn’s disease resistant or intolerant to azathioprine. Aliment Pharmacol Ther. 2004;19:295–301. doi:10.1111/j.1365-2036.2004.01850.x.
Markowitz J, Rosa J, Grancher K, Aiges H, Daum F. Long-term 6-mercaptopurine treatment in adolescents with Crohn’s disease. Gastroenterology. 1990;90:1347–1351.
Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn's disease. A meta-analysis. Ann Intern Med. 1995;123:132–142.
Topstad DR, Panaccione R, Heine JA, Johnson DRE, MacLean AR, Buie WD. Combined seton placement, infliximab infusion, and maintenance immunosuppressives improve healing rate in fistulizing anorectal Crohn’s disease. A single center experience. Dis Colon Rectum. 2003;46:577–583. doi:10.1007/s10350-004-6611-4.
Williams JG, Rothenberger DA, Nemer FD, Goldberg SM. Fistula-in ano in Crohn’s disease. Results of aggressive surgical treatment. Dis Colon Rectum. 1991;34:378–384. doi:10.1007/BF02053687.
Ardizzone S, Maconi G, Colombo E, Bollani Sand MG, Bianchi Porro G. Perianal fistulae following infliximab treatment. Clinical and endosonographic outcome. Inflamm Bowel Dis. 2004;10:91–96. doi:10.1097/00054725-200403000-00005.
Van Assche G, Vanbeckevoort D, Bielen D, et al. Magnetic resonance imaging of the effects of infliximab on perianal fistulizing Crohn’s disease. Am J Gastroenterol. 2003;98:332–339.
Loftus EV. Editorial imaging and therapy for perianal Crohn’s disease: on the right track? Am J Gastroenterol. 2004;99:89–90. doi:10.1111/j.1572-0241.2004.04016.x.
Parsi MA, Achkar JP, Richardson S, et al. Predictors of response to infliximab in patients with Crohn’s disease. Gastroenterology. 2002;123:707–713. doi:10.1053/gast.2002.35390.
Parsi MA, Lashner BA, Achkar JP, Connor JT, Brzezinski A. Type of fistula determines responses to infliximab in patients with fistulous Crohn’s disease. Am J Gastroenterol. 2004;99:445–449. doi:10.1111/j.1572-0241.2004.04083.x.
Vermeire S, Louis E, Carbonez A, et al. Demographic and clinical parameters influencing the short-term outcome of anti-TNF necrosis factor (infliximab) treatment on Crohn’s disease. Am J Gastroenterol. 2002;97:2357–2363. doi:10.1111/j.1572-0241.2002.05991.x.
Regueiro M, Mardini H. Treatment of perianal fistulizing Crohn’s disease with infliximab alone or as an adjunct to examine under anaesthesia with seton placement. Inflamm Bowel Dis. 2003;9:98–103. doi:10.1097/00054725-200303000-00003.
Rasul I, Wilson SR, MacRae H, Irwin S, Greenberg GR. Clinical and radiological responses after infliximab treatment for perianal fistulising Crohn’s disease. Am J Gastroenterol. 2004;99:82–88. doi:10.1046/j.1572-0241.2003.04009.x.
Bell SJ, Halligan AC, Windsor ACJ, Williams AB, Wiesel P, Kamm MA. Response of fistulating Crohn’s disease to infliximab treatment assessed by magnetic resonance. Aliment Pharmacol Ther. 2003;17:387–393. doi:10.1046/j.1365-2036.2003.01427.x.
Schwartz DA, White CM, Wise PE, Herline AJ. Use of endoscopic ultrasound to guide combination medical and surgical therapy for patients with Crohn’s perianal fistulas. Inflamm Bowel Dis. 2005;11:727–732. doi:10.1097/01.MIB.0000172811.57242.18.
Rutgeerts P, Diamonds RH, Bala M, et al. Scheduled maintenance treatment with infliximab is superior to episodic treatment for the healing of mucosal ulceration associated with Crohn’s disease. Gastrointest Endosc. 2006;63:433–442. doi:10.1016/j.gie.2005.08.011.
Rutgeerts P, Vermeire S, Van Assche G. Mucosal healing in inflammatory bowel disease: impossible ideal or therapeutic target? Gut. 2007;56:453–455. doi:10.1136/gut.2005.088732.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tougeron, D., Savoye, G., Savoye-Collet, C. et al. Predicting Factors of Fistula Healing and Clinical Remission After Infliximab-Based Combined Therapy for Perianal Fistulizing Crohn’s Disease. Dig Dis Sci 54, 1746–1752 (2009). https://doi.org/10.1007/s10620-008-0545-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-008-0545-y