
Abstract
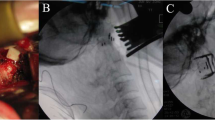
A 65-year-old woman presented with basilar invagination manifesting as neck pain, dysesthesia around the lips, and truncal ataxia. The radiological findings demonstrated invagination of the odontoid process into the medulla oblongata and vertical atlantoaxial subluxation with C1 assimilation. The clivo-axial angle was 88° and the cervicomedullary angle was 115°, indicating severe basilar invagination. We planned occipitocervical fusion with atlantoaxial distraction using a cylindrical titanium cage. C2 pedicle screws were inserted, and the atlantoaxial joint was opened to translocate the odontoid process downward. A cylindrical titanium cage packed with local bone graft was inserted into the opened facet joint space. Occipital-C2 fusion was completed by fastening the occipital bone plates with pedicle screws using titanium rods. Postoperatively, the apex of the odontoid process descended by 7 mm, and the clivo-axial and cervicomedullary angles opened to 112° and 125°, respectively. Invagination of the odontoid process into the medulla oblongata was relieved. The preoperative symptoms improved, and she remained symptom-free without requiring anterior decompression over 2 years. Bone fusion of the atlantoaxial joints was completed with sustained facet distraction 12 months after the surgery, and adequate relief of the basilar invagination was maintained. The atlantoaxial distraction method using a cylindrical titanium cage can be a useful option in posterior fusion surgery for basilar invagination.




Similar content being viewed by others


References
Abumi K, Takada T, Shono Y, Kaneda K, Fujiya M (1999) Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine (Phila Pa 1976) 24:1425–1434
Bundschuh C, Modic MT, Kearney F, Morris R, Deal C (1988) Rheumatoid arthritis of the cervical spine: surface-coil MR imaging. AJR Am J Roentgenol 151:181–187
Dickman CA, Locantro J, Fessler RG (1992) The influence of transoral odontoid resection on stability of the craniovertebral junction. J Neurosurg 77:525–530
Elliott RE, Tanweer O, Smith ML, Frempong-Boadu A (2014) Impact of starting point and bicortical purchase of C1 lateral mass screws on atlantoaxial fusion: meta-analysis and review of the literature. J Spinal Disord Tech. doi:10.1097/BSD.0b013e31828ffc97
Fukui K, Kataoka O, Sho T, Sumi M (1990) Pathomechanism, pathogenesis, and results of treatment in cervical spondylotic myelopathy caused by dynamic canal stenosis. Spine (Phila Pa 1976) 15:1148–1152
Goel A, Laheri V (1994) Plate and screw fixation for atlanto-axial subluxation. Acta Neurochir (Wien) 129:47–53
Goel A, Bhatjiwale M, Desai K (1998) Basilar invagination: a study based on 190 surgically treated patients. J Neurosurg 88:962–968
Goel A (2004) Treatment of basilar invagination by atlantoaxial joint distraction and direct lateral mass fixation. J Neurosurg Spine 1:281–286
Goel A, Shah A (2008) Atlantoaxial joint distraction as a treatment for basilar invagination: a report of an experience with 11 cases. Neurol India 56:144–150
Goel A, Shah A (2009) Reversal of longstanding musculoskeletal changes in basilar invagination after surgical decompression and stabilization. J Neurosurg Spine 10:220–227
Grob D, Dvorak J, Panjabi MM, Antinnes JA (1994) The role of plate and screw fixation in occipitocervical fusion in rheumatoid arthritis. Spine (Phila Pa 1976) 19:2545–2551
Grob D, Schutz U, Plotz G (1999) Occipitocervical fusion in patients with rheumatoid arthritis. Clin Orthop Relat Res 366:46–53
Hacker RJ, Cauthen JC, Gilbert TJ, Griffith SL (2000) A prospective randomized multicenter clinical evaluation of an anterior cervical fusion cage. Spine (Phila Pa 1976) Spine (Phila Pa 1976) 25:2646–2654, discussion 2655
Harms J, Melcher RP (2001) Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976) 26:2467–2471
Hida K, Iwasaki Y, Yano S, Akino M, Seki T (2008) Long-term follow-up results in patients with cervical disk disease treated by cervical anterior fusion using titanium cage implants. Neurol Med Chir (Tokyo) 48:440–446, discussion 446
Jian FZ, Chen Z, Wrede KH, Samii M, Ling F (2010) Direct posterior reduction and fixation for the treatment of basilar invagination with atlantoaxial dislocation. Neurosurgery 66:678–687, discussion 687
Kadoya S (1992) Grading and scoring system for neurological function in degenerative cervical spine disease—Neurosurgical Cervical Spine Scale. Neurol Med Chir (Tokyo) 32:40–41
Menezes AH, VanGilder JC (1988) Transoral-transpharyngeal approach to the anterior craniocervical junction. Ten-year experience with 72 patients. J Neurosurg 69:895–903
Nagashima C, Kubota S (1983) Craniocervical abnormalities. Modern diagnosis and a comprehensive surgical approach. Neurosurg Rev 6:187–197
Nishikawa M, Ohata K, Baba M, Terakawa Y, Hara M (2004) Chiari I malformation associated with ventral compression and instability: one-stage posterior decompression and fusion with a new instrumentation technique. Neurosurgery 54:1430–1434, discussion 1434–1435
Nockels RP, Shaffrey CI, Kanter AS, Azeem S, York JE (2007) Occipitocervical fusion with rigid internal fixation: long-term follow-up data in 69 patients. J Neurosurg Spine 7:117–123
Patel AJ, Boatey J, Muns J, Bollo RJ, Whitehead WE, Giannoni CM, Jea A (2012) Endoscopic endonasal odontoidectomy in a child with chronic type 3 atlantoaxial rotatory fixation: case report and literature review. Childs Nerv Syst 28:1971–1975
Sandhu FA, Pait TG, Benzel E, Henderson FC (2003) Occipitocervical fusion for rheumatoid arthritis using the inside-outside stabilization technique. Spine (Phila Pa 1976) 28: 414–419
Vale FL, Oliver M, Cahill DW (1999) Rigid occipitocervical fusion. J Neurosurg 91(2 Suppl):144–150
Zileli M, Cagli S (2002) Combined anterior and posterior approach for managing basilar invagination associated with type I Chiari malformation. J Spinal Disord Tech 15:284–289
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Atul Goel, Mumbai, India
Basilar invagination is a manifestation of ‘vertical’ atlantoaxial instability [12]. Incompetence of the muscles of the nape of the neck secondary to trauma or poor muscle nutrition may be the pathogenetic cause. Listhesis of the facet of atlas over the facet of axis results in superior and posterior migration of the odontoid process in relationship to the arch of atlas resulting in basilar invagination and atlantoxial dislocation [14]. The atlantoaxial dislocation in such cases is not freely mobile and reducible and was earlier referred to as ‘fixed’ atlantoaxial dislocation [7]. The most defining feature that probably revolutionised the treatment of ‘basilar invagination’ was the identification of the fact that atlantoaxial joints in such cases are not fixed but are functional and mobile and, more importantly, are reducible [1, 5, 9]. Instability of the atlantoaxial joint and microtrauma inflicted to critical neural structures by repeated abnormal movements of the odontoid process are the cause of neurological deficits and are more important than structural malformation or deformation that it results [9]. The subtleness and long-standing nature of process of listhesis result in remarkable natural readjustments that lead to a host of musculoskeletal and neural alterations, all aimed at reducing the impact of instability and in reducing the neural compromise. Torticollis, short neck, platybasia, bone fusions and several similar morphological alterations that are frequently observed in cases with basilar invagination are all potentially reversible following surgical procedure that stabilizes the atlantoaxial joint [9].
Opening of the atlantoaxial joint, denuding of the articular cartilage, stuffing of bone graft within the confines of the atlantoaxial joint and subsequent plate/rod and screw fixation of C1 and C2 pars/pedicle/facets form the basis of our fixation technique [6, 8]. The description of feasibility and safety of sectioning of the C2 ganglion, whenever necessary, to obtain wide exposure of the region to complete all the steps of the fixation technique is another crucial step in the advancement of surgery in the craniovertebral region [4]. The exposure of the atlantoaxial joint in cases with basilar invagination is significantly more difficult when compared to normally located joints. The joints are rostrally located and dissection in the region amidst large venous complexes can be tedious. Sectioning of C2 ganglion, particularly in such cases, can assist in providing a panoramic view to the joint and facets so that the entire surgical procedure can be done under direct surgical vision.
Distraction of facets of the spine by employing metal spacers is emerging to be a robust technique for provision of stability and realignment [10, 11]. Impaction of metal spacer within the atlantoaxial joint provides significant stability to the region [2]. Distraction of the facets by the spacers, at the site of fulcrum of craniovertebral movements, results in reduction of basilar invagination and restoration of craniovertebral and spinal alignment [4, 13]. However, as our experience in the treatment of basilar invagination in increasing, we have realised that it is more important to obtain stability of the atlantoaxial region than to aim at morphological reduction in basilar invagination. With that aim in mind, introduction of bone graft within the confines of the joint and in the appropriately prepared suboccipital region is crucially important.
The authors in the present manuscript have resorted to inclusion of the occipital bone in the fusion construct. The use of short plates/rods and segmental fixation at the point of fulcrum of movements as is done for atlantoaxial fixation is biomechanically far superior when compared to the use of long plates/rods necessary for occipitocervical fixation. The use of long length screws as is possible in the strong and largely cortical bone facets of atlas and axis is much more robust when compared to the use of multiple short screws in the suboccipital squama. Inclusion of the occipital bone and sub-axial spinal segment not only is unnecessary, but can significantly reduce the strength of the implant and adversely affect the neck movements and neck growth [3]. Manipulation of the facets that is the point of pathogenesis of basilar invagination is far more effective than remote manipulation of the occipital bone. Although the technique of exposure of the atlantoaxial joint is relatively difficult and tedious, if learnt appropriately and performed adequately, it can lead to gratifying surgical results in this relatively complex and daunting clinical situation.
References
1. Goel A (2004) Treatment of basilar invagination by atlantoaxial joint distraction and direct lateral mass fixation. J Neurosurg Spine.1(3):281–6.
2. Goel A (2007) Atlantoaxial joint jamming as a treatment for atlantoaxial dislocation: a preliminary report. Technical note. J Neurosurg Spine.7(1):90–4.
3. Goel A (2010) Occipitocervical fixation—is it necessary? Editorial, J Neurosurg Spine. 13(1):1–2.
4. Goel A (2012) Cervical ganglion 2 (CG2) neurectomy: a window to the atlantoaxial joint. World Neurosurg.78(1–2):78–9
5. Goel A, Bhatjiwale M, Desai K (1988) Basilar invagination: a study based on 190 surgically treated cases. J Neurosurg 88:962–968.
6. Goel A, Desai K, Muzumdar D (2002) Atlantoaxial fixation using plate and screw method: a report of 160 treated patients. Neurosurgery 51; 1351–1357.
7. Goel A, Kulkarni AG, Sharma P (2005) Reduction of fixed atlantoaxial dislocation in 24 cases: technical note. J Neurosurg Spine 2(4):505–9.
8. Goel A, Laheri VK (1994) Plate and screw fixation for atlanto-axial dislocation. (technical report). Acta Neurochir (Wien) 129:47–53.
9. Goel A, Shah A (2009) Reversal of longstanding musculoskeletal changes in basilar invagination after surgical decompression and stabilization. J Neurosurg Spine.10(3):220–7.
10. Goel A, Shah A (2011) Facetal distraction as treatment for single- and multilevel cervical spondylotic radiculopathy and myelopathy: a preliminary report. J Neurosurg Spine 14(6):689–96.
11. Goel A, Shah A, Jadhav M, Nama S (2013) Distraction of facets with intraarticular spacers as treatment for lumbar canal stenosis: report on a preliminary experience with 21 cases. J Neurosurg Spine 19(6):672–7.
12. Goel A, Shah A, Rajan S (2009) Vertical mobile and reducible atlantoaxial dislocation. Clinical article. J Neurosurg Spine 11(1):9–14.
13. Goel A, Sharma P. (2005) Craniovertebral junction realignment for the treatment of basilar invagination with syringomyelia: preliminary report of 12 cases. Neurol Med Chir (Tokyo) 45(10):512–8.
14. Kothari M, Goel A (2007) Transatlantic odonto-occipital listhesis: the so-called basilar invagination. Neurol India 55(1):6–7.
Rights and permissions
About this article
Cite this article
Yoshizumi, T., Murata, H., Ikenishi, Y. et al. Occipitocervical fusion with relief of odontoid invagination: atlantoaxial distraction method using cylindrical titanium cage for basilar invagination—case report. Neurosurg Rev 37, 519–525 (2014). https://doi.org/10.1007/s10143-014-0531-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-014-0531-0