
Abstract
Purpose
To report the radiological predictors of kyphotic deformity in osteoporotic vertebral compression fractures (OVCF).
Methods
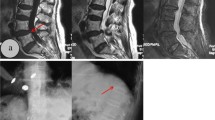
This is a retrospective study of 64 consecutive patients with OVCF. We studied the radiographic features in the immediate post-injury image of patients, who developed significant (more than 30°) segmental kyphotic deformity at final follow-up and compared them with those patients who did not.
Results
Thirty-three (82.5 %) out of 40 patients with fracture at thoracolumbar (TL) junction, 5 (33.3 %) patients out of 15 with fracture at lumbar (L) spine and 7 (77.7 %) patients out of 9 with fracture at thoracic (T) spine developed significant segmental kyphotic deformity. Forty-one (75.9 %) [TL-33 (80.5 %), L-4 (33.33 %) and T-4 (80 %)] out of 54 [TL-37 (68.51 %), L-12 (22.23 %) and T-5 (9.26 %)] patients with superior endplate fracture developed significant segmental kyphotic deformity. Forty patients (86.9 %) [TL-28 (70 %), L-6 (15 %) and T-6 (15 %)] out of 46 [TL-32 (69.56 %), L-8 (17.4 %) and T-6 (13.04 %)] with anterior cortical wall fracture developed significant segmental kyphotic deformity. Five patients (71.42 %) [TL-2 (40 %) and T-3 (60 %)] out of 7 [TL-02 (28.58 %), L-01 (14.28 %), T-04 (57.14 %)] with adjacent level fracture developed significant segmental kyphotic deformity. The average immediate post-injury kyphosis of 11° (5°–25°) increased to 29° (15°–50°) at final follow-up.
Conclusion
Progressive segmental kyphotic collapse following an OVCF seems unavoidable. Patients with TL junction and superior endplate fracture are probably at the highest risk for significant segmental kyphotic deformity.






Similar content being viewed by others


References
Chang Kao-Wha, Chen Ying-Yu, Lin Chien-Chung, Hsu Hsiang-Lan, Pai Ke-Chun (2005) Apical lordosating osteotomy and minimal segment fixation for the treatment of thoracic or thoracolumbar osteoporotic kyphosis. Spine 30:1674–1681
Brian K Alldredge, Koda-Kimble, Anne Mary, Young, Y Lloyd, Wayne A Kradjan, Joseph Guglielmo B (2009) Applied therapeutics: the clinical use of drugs. Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia, pp 101–103
WHO (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 843:1–129
Tsujio T, Nakamura H, Terai H, Hoshino M, Namikawa T, Matsumura A, Kato M, Suzuki A, Takayama K, Fukushima W, Kondo K, Hirota Y, Takaoka K (2011) Characteristic radiographic or magnetic resonance images of fresh osteoporotic vertebral fractures predicting potential risk for nonunion a prospective multicenter study. Spine 36:1229–1235
Belmont PJ Jr, Polly DW Jr, Cunningham BW et al (2001) The effects of hook pattern and kyphotic angulation on mechanical strength and apical rod strain in a long-segment posterior construct using a synthetic model. Spine 26:627–635
White AA, Panjabi MM, Thomas CL (1977) The clinical biomechanics of kyphotic deformities. Clin Orthop Relat Res 128:8–17
Heggeness MH (1993) Spine fracture with neurological deficit in osteoporosis. Osteoporos Int 3:215–221
Salomon C, Chopin D, Benoist M (1988) Spinal cord compression: an exceptional complication of spinal osteoporosis. Spine 13:222–224
Roush RN, Karen MSN, FNP BC (2011) Prevention and treatment of osteoporosis in postmenopausal women: a review. Am J Nurs 111:26–35
Adams MA, Freeman BJ, Morrison HP, Nelson IW, Dolan P (2000) Mechanical initiation of intervertebral disc degeneration. Spine 25:1625–1636
Pollintine P, Przybyla AS, Dolan P, Adams MA (2004) Neural arch load-bearing in old and degenerated spines. J Biomech 37:197–204
Edwards WT, Zheng Y, Ferrara LA, Yuan HA (2001) Structural features and thickness of the vertebral cortex in the thoracolumbar spine. Spine 26:218–225
Ortiz AO, Bordia R (2011) Bordia Injury to the vertebral endplate-disk complex associated with osteoporotic vertebral compression fractures. AJNR 32:115–120
Trout AT, Kallmes DF, Layton KF, Thielen KR, Hentz JG (2006) Vertebral endplate fractures: an indicator of the abnormal forces generated in the spine after vertebroplasty. J Bone Miner Res 21:1797–1802
Zhao F-D, Pollintinec P, Hole BD, Adams MA, Dolan P (2009) Vertebral fractures usually affect the cranial endplate because it is thinner and supported by less-dense trabecular bone. Bone 44:372–379
Brinckmann P, Biggemann M, Hilweg D (1988) Fatigue fracture of human lumbar vertebrae. Clin Biomech 3(Suppl 1):1–23
Pal GP, Cosio L, Routal RV (1988) Trajectory architecture of the trabecular bone between the body and the neural arch in human vertebrae. Anat Rec 222:418–425
Yuan HA, Brown CW, Phillips FM (2004) Osteoporotic spinal deformity: a biomechanical rationale for the clinical consequences and treatment of vertebral body compression fractures. J Spinal Disod Tech 17:236–242
Ryu CW, Han H, Lee YM, Lim MK (2009) The intravertebral cleft in benign vertebral compression fracture: the diagnostic performance of non-enhanced MRI and fat-suppressed contrast-enhanced MRI. Br J Radiol 82:976–981
Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ 3rd (1992) Incidence of clinically diagnosed vertebral fractures. A population based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 7:221–227
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Patil, S., Nene, A.M. Predictors of kyphotic deformity in osteoporotic vertebral compression fractures: a radiological study. Eur Spine J 23, 2737–2742 (2014). https://doi.org/10.1007/s00586-014-3457-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3457-x