
Abstract
Background
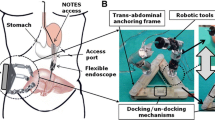
The lack of triangulation of standard endoscopic devices limits the degree of freedom for surgical maneuvers during natural orifice transluminal endoscopic surgery (NOTES). This study explored the feasibility of adapting an intuitively controlled master and slave transluminal endoscopic robot (MASTER) the authors developed to facilitate wedge hepatic resection in NOTES.
Methods
The MASTER consists of a master controller, a telesurgical workstation, and a slave manipulator that holds two end-effectors: a grasper, and a monopolar electrocautery hook. The master controller is attached to the wrist and fingers of the operator and connected to the manipulator by electrical and wire cables. Movements of the operator are detected and converted into control signals driving the slave manipulator via a tendon-sheath power transmission mechanism allowing nine degrees of freedom. Using this system, wedge hepatic resection was performed through the transgastric route on two female pigs under general anesthesia. Entry into the peritoneal cavity was via a 10-mm incision made on the anterior wall of the stomach by the electrocautery hook. Wedge hepatic resection was performed using the robotic grasper and hook. Hemostasis was achieved with the electrocautery hook. After the procedure, the resected liver tissue was retrieved through the mouth using the grasper.
Results
Using the MASTER, transgastric wedge hepatic resection was successfully performed on two pigs with no laparoscopic assistance. The entire procedure took 9.4 min (range, 8.5–10.2 min), with 7.1 min (range, 6–8.2 min) spent on excision of the liver tissue. The robotics-controlled device was able to grasp, retract, and excise the liver specimen successfully in the desired plane.
Conclusion
This study demonstrated for the first time that the MASTER could effectively mitigate the technical constraints normally encountered in NOTES procedures. With it, the triangulation of surgical tools and the manipulation of tissue became easy, and wedge hepatic resection could be accomplished successfully without the need for assistance using laparoscopic instruments.






Similar content being viewed by others


References
Lomanto D, Dhir U, So JB, Cheah WK, Moe MA, Ho KY (2009) Total transvaginal endoscopic abdominal wall hernia repair: a NOTES survival study. Hernia 13(4):415–419
Raman JD, Bergs RA, Fernandez R, Bagrodia A, Scott DJ, Tang SJ, Pearle MS, Cadeddu JA (2009) Complete transvaginal NOTES nephrectomy using magnetically anchored instrumentation. J Endourol 23:367–371
Perretta S, Dallemagne B, Coumaros D, Marescaux J (2008) Natural orifice transluminal endoscopic surgery: transgastric cholecystectomy in a survival porcine model. Surg Endosc 22:1126–1130
Leroy J, Cahill RA, Perretta S, Forgione A, Dallemagne B, Marescaux J (2009) Natural orifice translumenal endoscopic surgery (NOTES) applied totally to sigmoidectomy: an original technique with survival in a porcine model. Surg Endosc 23:24–30
Kalloo AN, Singh VK, Jagannath SB, Niiyama H, Hill SL, Vaughn CA, Magee CA, Kantsevoy SV (2004) Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc 60:114–117
Gettman MT, Blute ML (2007) Transvesical peritoneoscopy: initial clinical evaluation of the bladder as a portal for natural orifice translumenal endoscopic surgery. Mayo Clin Proc 82:843–845
Jagannath SB, Kantsevoy SV, Vaughn CA, Chung SSC, Cotton PB, Gostout CJ, Hawes RH, Pasricha PJ, Scorpio DG, Magee CA, Pipitone LJ, Kalloo AN (2005) Peroral transgastric endoscopic ligation of fallopian tubes with long-term survival in a porcine model. Gastrointest Endosc 61:449–453
Merrifield BF, Wagh MS, Thompson CC (2006) Peroral transgastric organ resection: a feasibility study in pigs. Gastrointest Endosc 63:693–697
Swain P (2008) Nephrectomy and natural orifice translumenal endoscopy (NOTES): transvaginal, transgastric, transrectal, and transvesical approaches. J Endourol 22:811–818
Whiteford MH, Denk PM, Swanström LL (2007) Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 21:1870–1874
ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery (2006) White paper October 2005. Gastrointest Endosc 63:199–203
Chiu PW, Lau JY, Ng EK, Lam CC, Hui M, To KF, Sung JJ, Chung SS (2008) Closure of a gastrotomy after transgastric tubal ligation by using the Eagle Claw VII: a survival experiment in a porcine model (with video). Gastrointest Endosc 68:554–559
Mellinger JD, MacFadyen BV, Kozarek RA, Soper ND, Birkett DH, Swanstrom LL (2007) Initial experience with a novel endoscopic device allowing intragastric manipulation and plication. Surg Endosc. 21:1002–1005
Seaman DL, Gostout CJ, de la Mora Levy JG, Knipschield MA (2006) Tissue anchors for transmural gut-wall apposition. Gastrointest Endosc 64:577–581
Ho KY, Phee SJ, So BYJ, Chung SCS (2007) Robotic manipulator for natural orifice transluminal endoscopic surgery. Gastrointest Endosc 65:AB110
Phee SJ, Low SC, Sun ZL, Ho KY, Huang WM, Thant ZM (2008) Robotic system for no-scar gastrointestinal surgery. Int J Med Robot 4:15–22
Low SC, Tang SW, Thant ZM, Phee L, Ho KY, Chung SC (2006) Master-slave robotic system for therapeutic gastrointestinal endoscopic procedures. Conf Proc IEEE Eng Med Biol Soc 1:3850–3853
Bardaro SJ, Swanström L (2006) Development of advanced endoscopes for natural orifice transluminal endoscopic surgery (NOTES). Minim Invasive Ther Allied Technol 15:378–383
Oleynikov D (2008) Robotic surgery. Surg Clin North Am 88:1121–1130
Acknowledgment
We thank Dr. Jennie Wong for her editorial assistance.
Disclosures
S. J. Phee, K. Y. Ho, D. Lomanto, S. C. Low, V. A. Huynh, A. P. Kencana, K. Yang, Z. L. Su, and S. C. Sydney Chung have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Phee, S.J., Ho, K.Y., Lomanto, D. et al. Natural orifice transgastric endoscopic wedge hepatic resection in an experimental model using an intuitively controlled master and slave transluminal endoscopic robot (MASTER). Surg Endosc 24, 2293–2298 (2010). https://doi.org/10.1007/s00464-010-0955-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-0955-8