
Abstract
Background
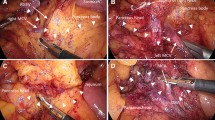
When we perform laparoscopic lymph node dissection around the inferior mesenteric artery (IMA), we preserve the left colic artery (LCA) to maintain the blood supply to the proximal sigmoid colon. In this study, we present our laparoscopic D2 and D3 lymph node (LN) dissection technique and evaluate its applicability and safety.
Methods
We performed LN dissection on 23 rectal and lower sigmoid colon cancer cases from April 2002 to December 2004. For D3 LN dissection, the incision to the mesosigmoid extends to just before the root of the IMA, which is exposed with an ultrasonic cutting and coagulating surgical device to avoid bleeding. Then, the arterial wall is exposed with a dissecting electrocautery spatula down to the LCA, at least 2 cm of which is exposed. Adipose tissue surrounding the IMA and inferior mesenteric vein is dissected. For D2 LN dissection, we partially expose the IMA to confirm the location of the LCA.
Results
The mean times taken for D2 and D3 LN dissections were 36.2 and 68.2 min, respectively. Both procedures took longer in male patients. There was a trend for the procedure overall to take less time in female patients. However, D2 dissection took significantly longer in male than female patients (p < 0.05). In women, D3 dissection took significantly longer than D2 (p < 0.05), but this trend was not seen in men. Increased experience among surgeons with this procedure was associated with significantly faster LN dissections in men (p < 0.05), but not in women (p = 0.493). Pearson product moment analysis identified a relationship between body mass index (BMI) and the time taken for D2 LN dissection (r = 0.765), but not D3 LN dissection (r = 0.158).
There was no treatment-related morbidity with this technique.
Conclusions
This method was safe and feasible for all patients in this series, but takes longer to perform in male patients.




Similar content being viewed by others

References
Baixauli J, Kiran RP, Delaney CP (2003) Investigation and management of ischemic colitis. Cleveland Clin J Med 70: 920–934
Griffiths JD (1956) Surgical anatomy of the blood supply of the distal colon. Ann R Coll Surg Engl 19: 241–256
Horton KM, Fishman EK (2000) 3D CT angiography of the celiac and superior mesenteric arteries with multidetector CT data sets: preliminary observations. Abdom Imaging 25: 523–525
Kornblith PL, Boley SJ, Whitehouse BS (1992) Anatomy of the splanchnic circulation. Surg Clin North Am 72: 1–30
Milsom JW, Böhm B (1996) Laparoscopic colorectal surgery. Springer-Verlag, New York, pp 117–194
Milsom JW, Böhm B, Decanini C, Fazio VW (1994) Laparoscopic oncologic proctosigmoidectomy with low colorectal anastomosis in a cadaver model. Surg Endosc 8: 1117–1123
Rosenblum JD, Boyle CM, Schwartz LB (1997) The mesenteric circulation: anatomy and physiology. Surg Clin North Am 77: 289–306
Acknowledgment
This study was supported by Kobayashi Magobe Memorial Medical Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) meeting, Fort Lauderdale, FL, USA, 13–16 April 2005
Rights and permissions
About this article
Cite this article
Kobayashi, M., Okamoto, K., Namikawa, T. et al. Laparoscopic lymph node dissection around the inferior mesenteric artery for cancer in the lower sigmoid colon and rectum. Surg Endosc 20, 563–569 (2006). https://doi.org/10.1007/s00464-005-0160-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0160-3