
Abstract
Background
Necropsy studies have shown that nonbacterial thrombotic endocarditis (NBTE) may be associated with cerebral infarctions and antemortem diagnosis is now possible. However, the best treatment for patients with NBTE presenting with stroke is not known.
Summary of report
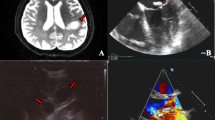
We describe three patients presenting with an acute embolic stroke secondary to large,mobile vegetations detected by transthoracic (one case) or transesophageal echocardiography (two cases). All patients underwent surgery for removal of the vegetations to prevent recurrent embolic events; valve replacement was necessary in two cases. The sterile nature of the vegetations was confirmed by pathological examination and negative stains and cultures of the surgical samples. A previously unrecognized hypercoagulable condition was diagnosed in all patients (antiphospholipid antibody syndrome in two cases and disseminated adenocarcinoma in one case).
Conclusion
NBTE should be considered among the possible causes of embolic stroke even in the absence of history of cancer, hypercoagulability, or previous embolic manifestations. If NBTE is diagnosed, the possibility of underlying thrombophilia should be thoroughly investigated. Valvular surgery represents a valuable therapeutic alternative in patients with large mobile vegetations, valvular dysfunction or recurrent embolic events despite anticoagulation.
Similar content being viewed by others


References
Biller J, Challa VR, Toole JF, Howard VJ (1982) Nonbacterial thrombotic endocarditis. A neurologic perspective of clinicopathologic correlations of 99 patients. Arch Neurol 39:95–98
Blanchard DG, Ross RS, Dittrich HC (1992) Nonbacterial thrombotic endocarditis. Assessment by transesophageal echocardiography. Chest 102:954–956
Brenner B, Blumenfeld Z, Markiewicz W, Reisner SA (1991) Cardiac involvement in patients with primary antiphospholipid syndrome. J Am Coll Cardiol 18:931–936
Cervera R, Khamashta MA, Font J, Reyes PA, Vianna JL, Lopez–Soto A, Amigo MC, Asherson RA, Azqueta M, Pare C (1991) High prevalence of significant heart valve lesions in patients with the ‘primary’ antiphospholipid syndrome. Lupus 1:43–47
Eiken PW, Edwards WD, Tazelaar HD, McBane RD, Zehr KJ (2001) Surgical pathology of nonbacterial thrombotic endocarditis in 30 patients, 1985–2000. Mayo Clin Proc 76:1204–1212
Fulham MJ, Gatenby P, Tuck RR (1994) Focal cerebral ischemia and antiphospholipid antibodies: a case for cardiac embolism.Acta Neurol Scand 90:417–423
Joffe II, Jacobs LE, Owen AN, Ioli A, Kotler MN (1996) Noninfective valvular masses: review of the literature with emphasis on imaging techniques and management. Am Heart J 131:1175–1183
Lopez JA, Ross RS, Fishbein MC, Siegel RJ (1987) Nonbacterial thrombotic endocarditis: a review. Am Heart J 113:773–784
Nihoyannopoulos P, Gomez PM, Joshi J, Loizou S, Walport MJ, Oakley CM (1990) Cardiac abnormalities in systemic lupus erythematosus. Association with raised anticardiolipin antibodies. Circulation 82:369–375
Rogers LR, Cho ES, Kempin S, Posner JB (1987) Cerebral infarction from non-bacterial thrombotic endocarditis. Clinical and pathological study including the effects of anticoagulation. Am J Med 83:746–756
Singhal B, Topcuoglu MA, Buonanno FS (2002) Acute ischemic stroke patterns infective and nonbacterial thrombotic endocarditis: a diffusionweighted magnetic resonance imaging study. Stroke 33:1267–1273
Skyrme–Jones RA, Wardrop CA, Wiles CM, Fraser AG (1995) Transesophageal echocardiographic demonstration of resolution of mitral vegetations after warfarin in a patient with the primary antiphospholipid syndrome. J Am Soc Echocardiogr 8:251–256
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rabinstein, A.A., Giovanelli, C., Romano, J.G. et al. Surgical treatment of nonbacterial thrombotic endocarditis presenting with stroke. J Neurol 252, 352–355 (2005). https://doi.org/10.1007/s00415-005-0660-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-005-0660-z