
Abstract
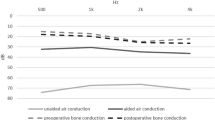
Previous researches focusing on BC hearing mechanisms proved that the two routes, (1) EAC sound radiation and (2) inertial of ossicular chain, partially contribute to normal BC hearing. Therefore, the BC hearing for those patients with congenital aural atresia should partially decrease theoretically due to their abnormal anatomy. However, there are not many studies which mention these patients’ BC hearing up till now. The objective of this study is to investigate congenital aural atresia patient’s BC hearing by analysis of pre-surgical audiogram and to study their potential BC hearing mechanisms using animal modeling and their ABR measurements. The study methoed involves analyzing 75 patients’ pre-operative audiogram. Then we produced an animal model by surgery to measure their BC hearing threshold changes. Clinical data showed that those patients had some BC hearing loss; and there were 25 cases (25/75, 33.3 %) which present with typical Carhart’s Notch. The animal experiments proved that inertia of ossicular chain contribute to partial BC hearing, which demonstrated that the inertia produced more affects on high frequencies by comparing with low frequencies. The patients with congenital aural atresia present BC hearing loss, which could be mainly ascribed to the absence of inertia of ossicular chain.



Similar content being viewed by others
References
Declau F, Cremers C, Van de Heyning P (1999) Diagnosis and management strategies in congenital atresia of the external auditory canal. Br J Audiol 33:313–327
EI-Begermy MA, Mansour OI, EI-Makhzangy AM, EI-Gindy TS (2009) Congenital auditory meatal atresia: a numerical review. Eur Arch Otorhinolaryngol 266(4):501–506
Schuknecht HF (1989) Congenital aural atresia. Laryngoscope 99:908–917
Stenfelt S, Goode RL (2005) Bone-conducted sound: physiological and clinical aspects. Otol Neurotol 26(6):1245–1261
Zhang JP, Liang XF, Qu YK, Chen HJ, Xu YD, Zhang ZG, Zhen YQ, Chen L (2006) Audiological assessment of patients with congenital external and middle ear malformation. J Audiol Speech Pathol 14(3):187–189
He LR, Zhuang HX (2007) Long-term investigation of hearing reconstruction in congenital microtia syndrome patients. Chin J Otorhinolaryngol Head Neck Surg 42(8):619–620
Nelissen RC, Mylanus EA, Cremers CW, Hol MK, Snik AF (2015) Long-term compliance and satisfaction with percutaneous bone conduction devices in patients with congenital unilateral conductive hearing loss. Otol Neurotol 36(5):826–833
Agterberg MJ, Frenzel H, Wollenberg B, Somers T, Cremers CW, Snik AF (2014) Amplification options in unilateral aural atresia: an active middle ear implant or a bone conduction device? Otol Neurotol 35(1):129–135
Carhart R (1950) Clinical application of bone conduction audiometry. Arch Otolaryngol 51(6):798–808
Kashio A, Ito K, Kakigi A, Karino S, Iwasaki S, Sakamoto T, Yasui T, Suzuki M, Yamasoba T (2011) Carhart notch 2-kHz bone conduction threshold dip: a nondefinitive predictor of stapes fixation in conductive hearing loss with normal tympanic membrane. Arch Otolaryngol Head Neck Surg 137(3):236–240
Khanna SM, Tonndorf J, Queller J (1976) Mechanical parameters of hearing by bone conduction. J Acoust Soc Am 60:139–154
Tonndorf J (1966) Bone conduction. Studies in experimental animals. Acta Oto-Laryngol 213(Suppl):1–132
Barany E (1938) A contribution to the physiology of bone conduction. Acta Oto-Layngol 26(Suppl):1–129
Huizing EH (1960) Bone conduction-the influence of the middle ear. Acta Oto-Laryngol 155(Suppl):1–99
Khanna SM, Tonndorf J, Queller J (1976) Mechanical parameters of hearing by bone conduction. J Acoust Soc Am 60:139–154
Tonndorf J, Greenfield EC, Kaufman RS (1964) Occlusion effect of the external-ear canal and its effect upon bone conduction. J Acoust Soc Am 36(5):1049
Dean MS, Martin FN (2000) Insert earphone depth and the occlusion effect. Am J Audiol 9(2):131–134
Stenfelt S, Wild T, Hato N, Goode RL (2003) Factors contributing to bone conduction: the outer ear. J Acoust Sco Am 113(2):902–913
Tsai V, Ostroff J, Korman M, Chen JM (2005) Bone-conduction hearing and the occlusion effect in otosclerosis and normal controls. Otol Neurotol 26:1138–1142
Elpern BS, Naunton RF (1963) The stability of the occlusion effect. Arch Otolaryngol 77:376–382
Kelley N, Reger S (1937) Effect of binaural occlusion of the external auditory meati on the sensitivity of the normal ear for bone conducted sound:1. Exp psycho 21:211–217
Kirikae I (1959) An experimental study on the fundamental mechanism of bone conduction. Acta Otolaryngol 145:1–111
Stenfelt S, Naohito Hato, Goode RL (2002) Factors contributing to bone conduction: The middle ear. J Acoust Soc Am 111(2):947–959
Stenfelt S (2006) Middle ear ossicles motion at hearing thresholds with air conduction and bone conduction stimulation. J Acoust Soc Am 119(5 Pt 1):2848–2858
Heffner RS (2004) Primate hearing from a mammalian perspective. Anat Rec Part A 281A:1111–1122
Romo T 3rd, Morris LG, Reitzen SD, Ghossaini SN, Wazen JJ, Kohan D (2009) Reconstruction of congenital microtia-atresia: outcomes with the MedPor/bone-anchored hearing aid-approach. Ann Plast Surg 62(4):384–389
Koontakis SE, Helidonis E, Jahrsdoerfer RA (1995) Microtia grade as an indicator of middle ear development in aural atrasia. Arch Otolaryngol Head Neck Surg 121:885–886
Acknowledgments
The authors thank The Newly Hundred Promising Talents Training Program from Shanghai Municipal Health Bureau (No. XBR2011068) and The Scholarship Award for Promising Scientists from China Ministry of Education in 2011 providing finial support for this research. In addition, the authors want to express their appreciations to Professor Geoffrey A. Manley for his help in revising language for this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We declare that we have no conflict of interest.
Additional information
L. Zhang and N. Gao contributed equally for this study.
Rights and permissions
About this article

Cite this article
Zhang, L., Gao, N., Yin, Y. et al. Bone conduction hearing in congenital aural atresia. Eur Arch Otorhinolaryngol 273, 1697–1703 (2016). https://doi.org/10.1007/s00405-015-3727-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-015-3727-1