
Abstract
Introduction and hypothesis
Puborectalis avulsion is a likely etiological factor for female pelvic organ prolapse (FPOP). We performed a study to establish minimal sonographic criteria for the diagnosis of avulsion.
Methods
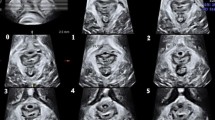
We analysed datasets of 764 women seen at a urogynecological service. Offline analysis of ultrasound datasets was performed blinded to patient data. Tomographic ultrasound imaging (TUI) was used to diagnose avulsion of the puborectalis muscle.
Results
Logistic regression modelling of TUI data showed that complete avulsion is best diagnosed by requiring the three central tomographic slices to be abnormal. This finding was obtained in 30% of patients and was associated with symptoms and signs of FPOP (P < 0.001). Lesser degrees of trauma (‘partial avulsion’) were not associated with symptoms or signs of pelvic floor dysfunction.
Conclusions
Complete avulsion of the puborectalis muscle is best diagnosed on TUI by requiring all three central slices to be abnormal. Partial trauma seems of limited clinical relevance.


Similar content being viewed by others


Abbreviations
- 3-D:
-
Three-dimensional
- ICS POP-Q:
-
International Continence Society Prolapse Quantification
- PFMC:
-
Pelvic floor muscle contraction
- ROI:
-
Region of Interest
- TUI:
-
Tomographic ultrasound imaging
References
Dietz H, Simpson J (2008) Levator trauma is associated with pelvic organ prolapse. Br J Obstet Gynaecol 115:979–984
DeLancey J, Morgan D, Fenner D, Kearney R, Guire K, Miller J et al (2007) Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol 109:295–302
Dietz H, Lanzarone V (2005) Levator trauma after vaginal delivery. Obstet Gynecol 106:707–712
Dietz H, Gillespie A, Phadke P (2007) Avulsion of the pubovisceral muscle associated with large vaginal tear after normal vaginal delivery at term. Aust NZ J Obstet Gynaecol 47:341–344
Shek K, Dietz H (2009) The effect of childbirth on hiatal dimensions: a prospective observational study. Obstet Gynecol 113:1272–1278
Valsky DV, Lipschuetz M, Bord A, Eldar I, Messing B, Hochner-Celnikier D et al (2009) Fetal head circumference and length of second stage of labor are risk factors for levator ani muscle injury, diagnosed by 3-dimensional transperineal ultrasound in primiparous women. Am J Obstet Gynecol 201:91.e91–91.e97
Abdool Z, Shek K, Dietz H (2009) The effect of levator avulsion on hiatal dimensions and function. Am J Obstet Gynecol 201:89.e81–89.e85
Dietz HP, Shek C (2008) Levator avulsion and grading of pelvic floor muscle strength. Int Urogynecol J 19:633–636
Dietz HP, Steensma AB (2006) The prevalence of major abnormalities of the levator ani in urogynaecological patients. Br J Obstet Gynaecol 113:225–230
DeLancey JO, Speights SE, Tunn R, Howard D, Ashton Miller JA (1999) Localized levator ani muscle abnormalities seen in MR images: site, size and side of occurrence. Int Urogynecol J 10:S20–S21
Dietz H (2004) Ultrasound imaging of the pelvic floor: 3D aspects. Ultrasound Obstet Gynecol 23:615–625
Shobeiri S, Chimpiri A, Allen AC, Nihira M, Quiroz LH (2009) Surgical reconstitution of a unilaterally avulsed symptomatic puborectalis muscle using autologous fascia lata. Obstet Gynecol 114:480–482
Wallner C, Wallace C, Maas C, Lange M, Lahaye M, Moayeri N et al (2009) A high resolution 3D study of the female pelvis reveals important anatomical and pathological details of the pelvic floor. Neurourol Urodyn 28:668–670
Dietz HP, Chantarasorn V, Shek KL (2010) Levator avulsion is a risk factor for cystocele recurrence. Ultrasound Obstet Gynecol 36:76–80
Model A, Shek KL, Dietz HP (2010) Levator defects are associated with prolapse after pelvic floor surgery. Eur J Obstet Gynecol Reprod Biol. doi:10.1016/j.ejogrb.2010.07.046
Dietz HP, Shek KL (2008) Validity and reproducibility of the digital detection of levator trauma. Int Urogynecol J 19:1097–1101
Kearney R, Miller JM, Delancey JO (2006) Interrater reliability and physical examination of the pubovisceral portion of the levator ani muscle, validity comparisons using MR imaging. Neurourol Urodyn 25:50–54
Weinstein MM, Pretorius D, Nager CW, Mittal R (2007) Inter-rater reliability of pelvic floor muscle imaging abnormalities with 3D ultrasound. Ultrasound Obstet Gynecol 30:538
Dietz H (2007) Quantification of major morphological abnormalities of the levator ani. Ultrasound Obstet Gynecol 29:329–334
Dietz HP, Shek K (2009) Tomographic ultrasound of the pelvic flooor: which levels matter most? Ultrasound Obstet Gynecol 33:698–703
Dietz H, Abbu A, Shek K (2008) The levator urethral gap measurement: a more objective means of determining levator avulsion? Ultrasound Obstet Gynecol 32:941–945
Singh K, Jakab M, Reid W, Berger LA, Hoyte L (2003) Three-dimensional magnetic resonance imaging assessment of levator ani morphologic features in different grades of prolapse. Am J Obstet Gynecol 188:910–915
Moegni F, Shek K, Dietz H (2010) Diagnosis of levator avulsion injury: a comparison of three methods. Int Urogynecol J 21:S215–S216
Conflicts of interest
Dr. Dietz has acted as a consultant for American Medical Systems (Minnetonka, MN), Continence Control Systems (Sydney) and Materna Inc. (San Francisco, CA), accepted speaker’s fees from General Electric Medical Ultrasound (Sydney, Australia), American Medical Systems, and Astellas (Tokyo, Japan), and has benefitted from equipment loans provided by General Electric, Bruel and Kjaer (Gentofte, Denmark), and Toshiba (North Ryde, Australia). Drs. Ka Lai Shek, Maria Jose Bernardo and Adrienne Kirby have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dietz, H.P., Bernardo, M.J., Kirby, A. et al. Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound. Int Urogynecol J 22, 699–704 (2011). https://doi.org/10.1007/s00192-010-1329-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-010-1329-4