
Abstract
Purpose
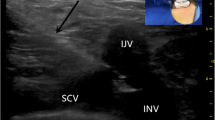
This study was undertaken to demonstrate the effectiveness of ultrasound (US)-guided placement of porta-cath (PC) through the right internal jugular vein (RIJV) by evaluating the onset of early and late complications.
Materials and methods
From 30 June 2008 to 30 June 2011, we placed 695 port-a-caths in 694 patients with a mean age of 58 years. Exclusion criteria were active infection, bleeding disorders and life expectancy <6 months. The procedures were performed in the angiography suite under local anaesthesia. After US-guided puncture of the RIJV, the subcutaneous pocket was prepared, followed by tunnelling of the vein and closure of the surgical wound. In order to evaluate pneumothorax (PNX), all patients underwent chest X-ray a few hours after the end of the procedure unless there were clinical indications. We evaluated the technical success of the procedure and the rate of complications.
Results
Technical success was achieved in all cases. The device was kept in place for an average of 168 days. There was one case of PNX (0.14%) as shown on chest X-ray and five cases of late complications (0.70%): one case of intracatheter thrombosis (0.14%), two cases of disconnection between the reservoir and catheter (0.28%) and two cases of PC infection (0.28%).
Conclusions
This procedure incurs very small number of complications compared with other positioning techniques using accesses such as the subclavian vein. Complications recorded in our study are comparable, in type and incidence, to those found by other authors, with the most frequent being device infection.
Riassunto
Obiettivo
Scopo del presente lavoro è stato dimostrare l’efficacia del posizionamento di port-a-cath (PC) attraverso la vena giugulare interna destra (VGID) sotto guida ecografica (US) valutando l’insorgenza di complicanze.
Materiali e metodi
Dal 30 giugno 2008 al 30 giugno 2011 abbiamo posizionato 695 PC in 694 pazienti con età media di 58 anni. I criteri di esclusione sono: infezione in atto, coagulopatie e aspettativa di vita inferiore ai 6 mesi. Le procedure sono state eseguite in sala angiografica previa anestesia locale. Abbiamo effettuato la puntura sottoguida US delle VGID, poi è stata preparata la tasca sottocutanea e tunnelizzazione del tramite e chiusura della ferita chirurgica. Per valutare lo pneumotorace (PNX) abbiamo eseguito un radiogramma del torace dopo qualche ora dalla procedura salvo diversa indicazione clinica. Abbiamo valutato la riuscita della procedura e il tasso di complicanze.
Risultati
La riuscita tecnica dell’impianto è stata ottenuta nella totalità dei casi. Il dispositivo è stato mantenuto in sede per una media di 168 giorni/paziente. Abbiamo registrato uno PNX (0,14%) evidenziato all’Rx di controllo e 5 casi di complicanze tardive (0,70%): 1 caso di trombosi intra-catetere (0,14%), 2 casi di deconnessioni tra il reservoir ed il catetere (0,28%) e 2 casi di infezioni del port (0,28%).
Conclusioni
Le complicanze che abbiamo osservato sono paragonabili sia in termini di incidenza che di tipologia a quelle riscontrate da altri autori; infatti anche dal nostro studio emerge che l’infezione del dispositivo risulta essere la complicanza più frequente.
Similar content being viewed by others


References/Bibliografia
Gabauer B, El-Sheik M, Vogt M, Wagner HJ (2009) Combined ultrasound and fluoroscopic guide porth catheter implantation-high succes and low complication rate. Eur J Radiol 69:517–522. DOI:10.1016/j. ejrad.2007.10.018
Niederhuber JE, Ensimnger W, Gives JW et al (1982) Totally implanted venous andarterial access system to replace external catheters in cancer treatment. Surgery 92:706–712
Sutor T, Schmidt H, Stasche N (2012) First experiences with ultrasound guided subclavian vein port placement in ENT. Laryngorhinootologie 91:28–31. DOI: 10.1055/s-0031-1291329
Plumhans C, Mahnken AH, Ocklenburg C et al (2009) Jugular versus subclavian totally implantable access ports: catheter position, complications and intrainterventional pain perception. Eur J Radiol 79:338–342. DOI:10.1016/j. ejrad.2009.12.010
Capaccioli L, Nistri M, Distante V (1998) Insertion and management of long-term central venous devices: role of radiologic imaging techniques. Radiol Med 96:369–374
Morris SL, Jacques PF, Mauro MA (1992) Radiology-assisted placement of implantable subcutaneous infusion ports for long-term venous access. Radiology 184:149–151
Centers for Disease Control (2011) Gudelines for the preventions of intravascular catheter-related infections. Centers for Disease Control, Atlanta
Hearns WC, Tiago M, Gohari A et al (2009) Chest port placement with use of the single-incision insertion technique. J Vasc Interv Radiol 20:1464–1469. DOI:10.1016/j. jvir.2009.07.035
Lorch H, Zwaan M, Kagel C et al (2001) Central venous access ports placed by interventional radiologists: experience with 125 consecutive patients. Cardiovasc Intervent Radiol 24:180–184. DOI: 10.1007/ s002700001721
Zahringer M, Hilgers J, Kruger K et al (2006) Ultrasound guided implantation of chest port systems via the lateral subclavian vein. Rofo 178:324–329. DOI: 10.1055/s-2006-926472
Wagner HJ, Teichgraber U, Gabauer B et al (2003) Transjugular implantation of venous port catheter systems. Rofo 175:1539–1544. DOI: 10.1055/s-2003-43406
Lehart M, Chegini M, Gmeiwieser J et al (1998) Radiologic implantation of central venous portal systems in the forearm. Rofo 169:189–194. DOI: 10.1055/s-2007-1015072
Lehart M, Chegini M, Gmeiwieser J et al (2010) Radiologic implantation of central venous portal systems in the forearm. Technical results and long term outcome in 391 patients. Rofo 182:20–28. DOI: 10.1055/s-0028-1109453
Biffi R, Orsi F, Pozzi S et al (2009) Best choice of central venous insertion site for the prevention of catheterrelated complications in adult patients who need cancer therapy: a randomized trial. Ann Oncol 20:935–940. DOI: 10.1093/annonc/mdn701
Park HS, Kim YI, Lee SH et al (2009) Central venous infusion port inserted via high versus low jugular venous approaches: retrospective comparison of outcome and complications. Eur J Radiol 72:494–498. DOI:10.1016/j. ejrad.2008.09.015
Ruesch S, Walder B, Martin R et al (2002) Complications of central venous catheters: internal jugular versus subclavian access a systematic review. Crit Care Med 30:454–460. DOI:10.1097/00003246-20020200000031
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Capalbo, E., Peli, M., Lovisatti, M. et al. Placement of port-a-cath through the right internal jugular vein under ultrasound guidance. Radiol med 118, 608–615 (2013). https://doi.org/10.1007/s11547-012-0894-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-012-0894-6