
Abstract
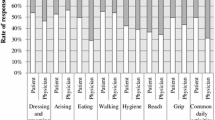
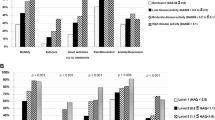
Some health problems are considered by many individuals as a ‘normal’ part of ageing. Our aim was to investigate whether patients with rheumatoid arthritis (RA) consider different types and levels of health losses as acceptable beyond a certain age. A multicenter cross-sectional survey was performed involving RA patients at the initiation of the first biological therapy. The EQ-5D and the Health Assessment Questionnaire Disability Index (HAQ-DI) questionnaires were used to describe domain-specific health states. Patients were asked to indicate for each domain from what age and onward (between ages 30 and 80 years in 10 year intervals) they considered moderate and severe problems acceptable or alternatively never acceptable. Seventy-seven RA patients (females 86 %, mean age 50.3, disease duration 9.1 years) completed the questionnaire. Disease activity (DAS28), EQ-5D and HAQ-DI scores were mean 6.00 (SD 0.85), 0.35 (SD 0.36), 1.48 (SD 0.66), respectively. The majority of the patients considered age 70 and beyond as acceptable to have some health problems (EQ-5D: self-care 42 %, pain/discomfort 34 %, mobility 33 %, usual activities 33 %, anxiety/depression 27 %), whilst at ages 30 and 40 as not acceptable. Severe health problems were mostly (57–69 %) considered never acceptable, except the ‘Usual activities’ domain (acceptable from age 80 by 50.6 %). The great majority of the patients (77–96 %) were younger than what they indicated as the acceptability age limit. Similar results were found for the HAQ-DI. This small experimental study suggests that RA patients consider some health problems acceptable. This acceptability is age related and varies by health areas. Further larger studies are needed to explore explanatory variables and to compare with other diseases. Owing to the impact acceptability might have on RA patients’ self-evaluation of current health state and decision-making, the topic deserves methodological improvement and further investigation.



Similar content being viewed by others

References
WHO: Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June, 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948 (1948)
Renehan, E., Dow, B., Lin, X., Blackberry, I., Haapala, I., Gaffy, E., Cyarto, E., Brasher, K., Hendy, S.: Healthy ageing literature review. Victorian Government. http://www.health.vic.gov.au/agedcare/maintaining/downloads/healthy_litreview.pdf (2012). Accessed 28 Feb 2014
Hung, L.-W., Kempen, G.I.J.M., De Vries, N.K.: Cross-cultural comparison between academic and lay views of healthy ageing: a literature review. Ageing Soc. 30(8), 1373–1391 (2010)
Bleichrodt, H., Herrero, C., Pinto, J.L.: A proposal to solve the comparability problem in cost–utility analysis. J. Health Econ. 21(3), 397–403 (2002)
Brouwer, W.B., van Exel, N.J., Stolk, E.A.: Acceptability of less than perfect health states. Soc. Sci. Med. 60(2), 237–246 (2005)
EuroQol, G.: EuroQol—a new facility for the measurement of health-related quality of life. Health Policy 16(3), 199–208 (1990)
Smolen, J.S., Landewe, R., Breedveld, F.C., Buch, M., Burmester, G., Dougados, M., Emery, P., Gaujoux-Viala, C., Gossec, L., Nam, J., Ramiro, S., Winthrop, K., de Wit, M., Aletaha, D., Betteridge, N., Bijlsma, J.W., Boers, M., Buttgereit, F., Combe, B., Cutolo, M., Damjanov, N., Hazes, J.M., Kouloumas, M., Kvien, T.K., Mariette, X., Pavelka, K., van Riel, P.L., Rubbert-Roth, A., Scholte-Voshaar, M., Scott, D.L., Sokka-Isler, T., Wong, J.B., van der Heijde, D.: EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann. Rheum. Dis. 73(3), 492–509 (2014)
Poulos, C., Hauber, A.B., Gonzalez, J.M., Turpcu, A.: Patients’ willingness to trade off between the duration and frequency of rheumatoid arthritis treatments. Arthritis Care Res (Hoboken) (2013). doi:10.1002/acr.22265
Augustovski, F., Beratarrechea, A., Irazola, V., Rubinstein, F., Tesolin, P., Gonzalez, J., Lencina, V., Scolnik, M., Waimann, C., Navarta, D., Citera, G., Soriano, E.R.: Patient preferences for biologic agents in rheumatoid arthritis: a discrete-choice experiment. Value Health 16(2), 385–393 (2013)
Meesters, J., de Boer, I., van den Berg, M., Fiocco, M., Vliet Vlieland, T.: Unmet information needs about the delivery of rheumatology health care services: a survey among patients with rheumatoid arthritis. Patient Educ. Couns. 85(2), 299–303 (2011)
Harrison, M.J., Davies, L.M., Bansback, N.J., Ingram, M., Anis, A.H., Symmons, D.P.: The validity and responsiveness of generic utility measures in rheumatoid arthritis: a review. J. Rheumatol. 35(4), 592–602 (2008)
Szende, A., Nemeth, R.: Health-related quality of life of the Hungarian population. Orv. Hetil. 144(34), 1667–1674 (2003)
Maska, L., Anderson, J., Michaud, K.: Measures of functional status and quality of life in rheumatoid arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Improved Health Assessment Questionnaire (Improved HAQ), and Rheumatoid Arthritis Quality of Life (RAQoL). Arthritis Care Res (Hoboken) 63(Suppl 11), S4–S13 (2011)
Péntek, M., Rojkovich, B., Czirják, L., Géher, P., Keszthelyi, P., Kovács, A., Kovács, L., Náfrádi, L., Szanyó, F., Szekanecz, Z., Tamási, L., Tóth, E., Ujfalussy, I., Varjú, T., Gulácsi, L.: Biológikumok Alkalmazása Rheumatoid Arthritisben – Terápiafelmérés (BARAT vizsgálat): biológiai terápiát kezdő betegek klinikai jellemzői és egészségügyi szolgáltatások igénybevételének jellemzői. Immunol. Szle. 3(4), 36–48 (2011)
Péntek, M., Gulácsi, L., Rojkovich, B., Brodszky, V., van Exel, J., Brouwer, W.B.F.: Subjective health expectations at biological therapy initiation: a survey of rheumatoid arthritis patients and rheumatologists. Eur. J. Health Econ. (2014). doi:10.1007/s10198-014-0597-1
Anderson, J.K., Zimmerman, L., Caplan, L., Michaud, K.: Measures of rheumatoid arthritis disease activity: Patient (PtGA) and Provider (PrGA) Global Assessment of Disease Activity, Disease Activity Score (DAS) and Disease Activity Score with 28-Joint Counts (DAS28), Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), Patient Activity Score (PAS) and Patient Activity Score-II (PASII), Routine Assessment of Patient Index Data (RAPID), Rheumatoid Arthritis Disease Activity Index (RADAI) and Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5), Chronic Arthritis Systemic Index (CASI), Patient-Based Disease Activity Score With ESR (PDAS1) and Patient-Based Disease Activity Score without ESR (PDAS2), and Mean Overall Index for Rheumatoid Arthritis (MOI-RA). Arthritis Care Res (Hoboken) 63(Suppl 11), S14–S36 (2011)
Radbout University, N.: DAS28. http://www.das-score.nl/das28/en/. Accessed Jan 2014
Buitinga, L., Braakman-Jansen, L.M., Taal, E., van de Laar, M.A.: Worst-case future scenarios of patients with rheumatoid arthritis: a cross-sectional study. Rheumatology (Oxford) 51(11), 2027–2033 (2012)
Buitinga, L., Braakman-Jansen, L.M., Taal, E., van de Laar, M.A.: Future expectations and worst-case future scenarios of patients with rheumatoid arthritis: a focus group study. Musculoskeletal Care 10(4), 240–247 (2012)
Sanderson, T., Hewlett, S., Richards, P., Morris, M., Calnan, M.: Utilizing qualitative data from nominal groups: exploring the influences on treatment outcome prioritization with rheumatoid arthritis patients. J. Health Psychol. 17(1), 132–142 (2012)
Boncz, I., Sebestyen, A.: Economy and mortality in Eastern and Western Europe between 1945 and 1990: the largest medical trial of history. Int. J. Epidemiol. 35(3), 796–797; author reply 797–799 (2006)
Boncz, I., Sebestyen, A.: Financial deficits in the health services of the UK and Hungary. Lancet 368(9539), 917–918 (2006)
Kovacs, A., Dobrossy, L., Budai, A., Boncz, I., Cornides, A.: Cervical screening in Hungary: why does the “English model” work but the “Hungarian model” does not? Eur. J. Gynaecol. Oncol. 29(1), 5–9 (2008)
Krishnan, E., Sokka, T., Hakkinen, A., Hubert, H., Hannonen, P.: Normative values for the Health Assessment Questionnaire disability index: benchmarking disability in the general population. Arthritis Rheum. 50(3), 953–960 (2004)
Sokka, T., Makinen, H., Hannonen, P., Pincus, T.: Most people over age 50 in the general population do not meet ACR remission criteria or OMERACT minimal disease activity criteria for rheumatoid arthritis. Rheumatology (Oxford) 46(6), 1020–1023 (2007)
Sallai, J.R., Hunka, A., Hejj, G., Ratko, I., Ortutay, J., Markus, I., Ormos, G., Ujfalussy, A., Szekeres, L., Insperger, A., Varju, T., Balint, G.: Survey of quality of life of rheumatoid arthritis patients admitted to rehabilitation centres in Hungary. Orv. Hetil. 154(35), 1381–1388 (2013)
Cutolo, M., Kitas, G.D., van Riel, P.L.: Burden of disease in treated rheumatoid arthritis patients: going beyond the joint. Semin. Arthritis Rheum. 43(4), 479–488 (2014)
Marra, C.A., Woolcott, J.C., Kopec, J.A., Shojania, K., Offer, R., Brazier, J.E., Esdaile, J.M., Anis, A.H.: A comparison of generic, indirect utility measures (the HUI2, HUI3, SF-6D, and the EQ-5D) and disease-specific instruments (the RAQoL and the HAQ) in rheumatoid arthritis. Soc. Sci. Med. 60(7), 1571–1582 (2005)
Felson, D.T., Anderson, J.J., Boers, M., Bombardier, C., Furst, D., Goldsmith, C., Katz, L.M., Lightfoot Jr, R., Paulus, H., Strand, V., et al.: American College of Rheumatology. Preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum. 38(6), 727–735 (1995)
Pease, C., Pope, J.E., Truong, D., Bombardier, C., Widdifield, J., Thorne, J.C., Paul Haraoui, B., Psaradellis, E., Sampalis, J., Bonner, A.: Comparison of anti-TNF treatment initiation in rheumatoid arthritis databases demonstrates wide country variability in patient parameters at initiation of anti-TNF therapy. Semin. Arthritis Rheum. 41(1), 81–89 (2011)
Kobelt, G.: Thoughts on health economics in rheumatoid arthritis. Ann. Rheum. Dis. 66(Suppl 3), iii35–39 (2007)
Acknowledgments
The authors are grateful to the patients who participated in the study. The survey would not have been possible without the valuable work of the following colleagues: Fülöp A and Tandari M (Budapest); Bodnár N, Szamosi Sz, Szűcs G and Váncsa A (Debrecen); Abrudán K, Kovács H and Závada Zs (Gyula); Szanyó F (Győr); Böjte Gy, Eiben A and Sterba G (Kistarcsa); Fazekas K, Flórián Á and Lukács K (Miskolc); Encs E, Tisza A and Varjú T (Nyíregyháza); Balogh A and Hulló D (Szeged); Baksay B, Bíró J and Gácsi K (Szolnok); Náfrádi L (Szombathely); and Niedermayer D and Varjú C (Pécs). The survey was supported by an independent grant from the Centre for Public Affairs Studies Foundation and HTA Co. The work was supported by the European Union and the State of Hungary co-financed by the European Social Fund in the framework of TÁMOP-4.2.4.A/2-11/1-2012-0001 ‘National Excellence Program’ (Z.S., Debrecen), and the University of Debrecen, Faculty of Medicine Bridging Fund (Z.S., Debrecen). The proofreading of the manuscript was supported by the TÁMOP 4.2.2./B-10/1-2010-0023 project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Péntek, M., Rojkovich, B., Czirják, L. et al. Acceptability of less than perfect health states in rheumatoid arthritis: the patients’ perspective. Eur J Health Econ 15 (Suppl 1), 73–82 (2014). https://doi.org/10.1007/s10198-014-0596-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-014-0596-2