
Abstract
Background
The rates of nonunion after femoral nailing are currently reported to be 4.1–12.5 %. The purpose of this study was to identify the risk factors of noninfected nonunion after femoral nailing, focusing in particular on the effects of the length of the distal main fragment.
Methods
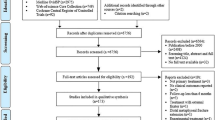
A case–control study was conducted with 105 patients, with a case (nonunion group)–control (control group) ratio of 1:2. The nonunion group (n = 35) comprised patients with consecutive symptomatic nonunions after femoral nailing who were treated in our institute; the control group (n = 70) were matched by age to the nonunion group. Type of fracture, soft tissue injury, length of femur and nail length, incidence of screw breakage, nail diameter, mean length of distal main fragment, and any episode of dynamization were retrospectively examined. Univariate and multivariate analyses were performed to elucidate the risk factors of nonunion after femoral nailing.
Results
Increased risk of nonunion after femoral nailing was associated with (1) open fracture, (2) screw breakage, (3) shorter length of a distal fragment, and (4) any episodes of dynamization. Receiver operating characteristic analysis showed that a distal fragment length of <43 % of the total femur length was the cutoff level for nonunion after nailing. The odds ratio for nonunion was 6.40 (95 % CI 2.70–15.2) when the length of the distal main fragment was <43 % of the femur length. Multivariate logistic analysis revealed that the risk of nonunion after femoral nailing increased (1) with breakage of locking screws (p = 0.0021), (2) with dynamization (p = 0.0029), (3) with a shorter distal fragment length (p = 0.0379), and (4) with an open fracture (p = 0.0397).
Conclusion
The elucidated risk factors of nonunion after femoral nailing were identified as open fracture, infra-isthmal femoral fracture, breakage of locking screw, and inappropriate dynamization. We believe that the surgeon should be consciously aware of the need for additional surgical fixation for the distal fragment when performing femoral nailing of infra-isthmal femoral fractures.


Similar content being viewed by others


References
Winquist RA, Hansen ST Jr, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am. 1984;66:529–39.
Brumback RJ, Uwagie-Ero S, Lakatos RP, Poka A, Bathon GH, Burgess AR. Intramedullary nailing of femoral shaft fractures. Part II: fracture-healing with static interlocking fixation. J Bone Joint Surg Am. 1988;70:1453–62.
Clatworthy MG, Clark DI, Gray DH, Hardy AE. Reamed versus unreamed femoral nails. A randomised, prospective trial. J Bone Joint Surg Br. 1998;80:485–9.
Taitsman LA, Lynch JR, Agel J, Barei DP, Nork SE. Risk factors for femoral nonunion after femoral shaft fracture. J Trauma. 2009;67:1389–92.
Pihlajamaki HK, Salminen ST, Bostman OM. The treatment of nonunions following intramedullary nailing of femoral shaft fractures. J Orthop Trauma. 2002;16:394–402.
Canadian OTS. Nonunion following intramedullary nailing of the femur with and without reaming. Results of a multicenter randomized clinical trial. J Bone Joint Surg Am. 2003;85-A:2093–6.
Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma. 2001;15:161–9.
Selvakumar K, Saw KY, Fathima M. Comparison study between reamed and unreamed nailing of closed femoral fractures. Med J Malaysia. 2001;56 Suppl D:24–8.
Noumi T, Yokoyama K, Ohtsuka H, Nakamura K, Itoman M. Intramedullary nailing for open fractures of the femoral shaft: evaluation of contributing factors on deep infection and nonunion using multivariate analysis. Injury. 2005;36:1085–93.
Augat P, Margevicius K, Simon J, Wolf S, Suger G, Claes L. Local tissue properties in bone healing: influence of size and stability of the osteotomy gap. J Orthop Res. 1998;16:475–81.
Claes L, Eckert-Hubner K, Augat P. The fracture gap size influences the local vascularization and tissue differentiation in callus healing. Langenbecks Arch Surg. 2003;388:316–22.
Malik MH, Harwood P, Diggle P, Khan SA. Factors affecting rates of infection and nonunion in intramedullary nailing. J Bone Joint Surg Br. 2004;86:556–60.
Giannoudis PV, MacDonald DA, Matthews SJ, Smith RM, Furlong AJ, De Boer P. Nonunion of the femoral diaphysis. The influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg Br. 2000;82:655–8.
Park J, Kim SG, Yoon HK, Yang KH. The treatment of nonisthmal femoral shaft nonunions with im nail exchange versus augmentation plating. J Orthop Trauma. 2010;24:89–94.
Tan WJ, Kwan MK, Deepak AS, Saw A, Peng BC, Jalalullah W. Size of interlocking nails used in the treatment of diaphyseal femoral fractures. Med J Malaysia. 2006;61 Suppl B:18–22.
Tigani D, Fravisini M, Stagni C, Pascarella R, Boriani S. Interlocking nail for femoral shaft fractures: is dynamization always necessary? Int Orthop. 2005;29:101–4.
Wu CC. The effect of dynamization on slowing the healing of femur shaft fractures after interlocking nailing. J Trauma. 1997;43:263–7.
Wu CC, Shih CH. Effect of dynamization of a static interlocking nail on fracture healing. Can J Surg. 1993;36:302–6.
Basumallick MN, Bandopadhyay A. Effect of dynamization in open interlocking nailing of femoral fractures. A prospective randomized comparative study of 50 cases with a 2-year follow-up. Acta Orthop Belg. 2002;68:42–8.
De Bastiani G, Aldegheri R, Renzi Brivio L. The treatment of fractures with a dynamic axial fixator. J Bone Joint Surg Br. 1984;66:538–45.
Epari DR, Kassi JP, Schell H, Duda GN. Timely fracture-healing requires optimization of axial fixation stability. J Bone Joint Surg Am. 2007;89:1575–85.
Augat P, Burger J, Schorlemmer S, Henke T, Peraus M, Claes L. Shear movement at the fracture site delays healing in a diaphyseal fracture model. J Orthop Res. 2003;21:1011–7.
Watanabe Y, Takai S, Yamashita F, Kusakabe T, Kim W, Hirasawa Y. Second-generation intramedullary supracondylar nail for distal femoral fractures. Int Orthop. 2002;26:85–8.
Conflict of interest
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Watanabe, Y., Takenaka, N., Kobayashi, M. et al. Infra-isthmal fracture is a risk factor for nonunion after femoral nailing: a case–control study. J Orthop Sci 18, 76–80 (2013). https://doi.org/10.1007/s00776-012-0316-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-012-0316-7