
Abstract
Purpose
This review summarizes the published methods of colonic EFTR, examining data on feasibility and safety. Due to the introduction of bowel cancer screening programs, there is an increasing incidence of complex colonic polyps and early colonic cancer that requires segmental colectomy. Traditional radical surgery is associated with significant morbidity, and there is a need for alternative treatments.
Methods
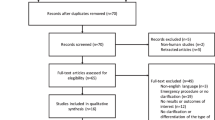
Systematic literature search identified articles describing EFTR techniques of colon, published between 1990 and 2012. Complication rates, anastomotic bursting pressures, procedure duration, specimen size and quality, and postmortem findings were analyzed.
Results
Five research groups reported four EFTR techniques using endoscopic stapling devices, T-tags, compression closure, or laparoscopic assistance for defect closure before or after specimen resection. A total of 113 procedures were performed in 99 porcine models, with an overall success rate of 89 and 4 % mortality. The intraoperative complication rate was 22 % (0–67 %). Post-resection closure methods more commonly resulted in failure to close the defect (5–55 %) and a high incidence of abnormal findings at postmortem examination (84 %). Significant heterogeneity was observed in procedure duration (median or mean 3–233 min) and size of the excised specimen (median or mean 1.7–3.6 cm). Anastomotic bursting pressures and specimen quality were poorly documented.
Conclusions
The technique of EFTR is developing, but the inability to close the resection defect reliably is a major obstacle. The review highlights the challenges that need to be addressed in future preclinical studies.




Similar content being viewed by others


References
Gill M, Rutter M, Holtham S (2013) Management and short-term outcome of malignant colorectal polyps in the North of England. Colorectal Dis 15(2):169–176
Saito Y, Fukuzawa M, Matsuda T, Fukunaga S, Sakamoto T, Uraoka T, Nakajima T, Ikehara H, Fu KI, Itoi T, Fujii T (2010) Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surg Endosc 24:343–352
Conio M, Repici A, Demarquay J-F, Blanchi S, Dumas R, Filiberti R (2004) EMR of large sessile colorectal polyps. Gastrointest Endosc 60:234–241
Saito Y, Uraoka T, Yamaguchi Y, Hotta K, Sakamoto N, Ikematsu H, Fukuzawa M, Kobayashi N, Nasu J, Michida T, Yoshida S, Ikehara H, Otake Y, Nakajima T, Matsuda T, Saito D (2010) A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc 72:1217–1225
Church J (2003) Avoiding surgery in patients with colorectal polyps. Dis Colon Rectum 46:1513–1516
Harrow P, Nayagam S, Stafford N, Hopkins K, Loke R (2011) A comparison of incidence of colorectal cancer and polyps in bowel cancer screening programme patients with symptomatic patients referred under 2 week wait in a demographically matched population. Gut 60:A114
Lee TJ, Pascall G, Wood T, Westwood C, Gunning K, Moncur P, Waddup G, Rees C, Rutter M, Dhar A (2009) Colonic polyps are different in the UK bowel cancer screening programme population compared to the symptomatic population. Gastrointest Endosc 69:AB290–AB291
Logan RFA, Patnick J, Nickerson C, Coleman L, Rutter MD, von Wagner C (2011) Outcomes of the bowel cancer screening programme (BCSP) in England after the first 1 million tests. Gut 61(10):10439–10446
Vlug MS, Wind J, Hollmann MW, Ubbink DT, Cense HA, Engel AF, Gerhards MF, van Wagensveld BA, van der Zaag ES, van Geloven AAW, Sprangers MAG, Cuesta MA, Bemelman WA, LAFA study group (2011) Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). Ann Surg 254:868–875. doi:10.1097/SLA.0b013e31821fd1ce
Kesisoglou I, Sapalidis K (2010) Treatment of early rectal cancer. Tech Coloproctol 14:33–34
Lee W, Lee D, Choi S, Chun H (2003) Transanal endoscopic microsurgery and radical surgery for T1 and T2 rectal cancer. Surg Endosc 17:1283–1287
Kopelman Y, Siersema PD, Bapaye A, Kopelman D (2012) Endoscopic full-thickness GI wall resection: current status. Gastrointest Endosc 75:165–173
Schurr MO, Buess G, Raestrup H, Arezzo A, Buerkert A, Schell C, Adams R, Banik M (2001) Full-thickness resection device (FTRD) for endoluminal removal of large bowel tumours: development of the instrument and related experimental studies. Minim Invasive Ther Allied Technol 10:301–309
Rajan E, Gostout CJ, Burgart LJ, Leontovich ON, Knipschield MA, Herman LJ, Norton ID (2002) First endoluminal system for transmural resection of colorectal tissue with a prototype full-thickness resection device in a porcine model. Gastrointest Endosc 55:915–920
Raju GS, Malhotra A, Ahmed I (2009) Colonoscopic full-thickness resection of the colon in a porcine model as a prelude to endoscopic surgery of difficult colon polyps: a novel technique (with videos). Gastrointest Endosc 70:159–165
von Renteln D, Schmidt A, Vassiliou MC, Rudolph HU, Caca K (2010) Endoscopic full-thickness resection and defect closure in the colon. Gastrointest Endosc 71:1267–1273
Rieder E, Martinec DV, Dunst CM, Swanstrom LLA (2011) A novel technique for natural orifice endoscopic full-thickness colon wall resection: an experimental pilot study. J Am Coll Surg 213:422–429
von Renteln D, Kratt T, Rosch T, Denzer UW, Schachschal G (2011) Endoscopic full-thickness resection in the colon by using a clip-and-cut technique: an animal study. Gastrointest Endosc 74:1108–1114
Kennedy RH, Cahill RA, Sibbons P, Fraser C (2011) The “FLEX” procedure: a new technique for full-thickness laparo-endoscopic excision in the colon. Endoscopy 43:223–229
Martin JP, Batt SC, Smith GV, Dawson P, Cohen P (2011) Malignant polyps removed from the bowel cancer screening programme in London. Gut 60:A70
Fearon KCH, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CHC, Lassen K, Nygren J, Hausel J, Soop M, Andersen J, Kehlet H (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24:466–477
Zlatanic J, Waye JD, Kim PS, Baiocco PJ, Gleim GW (1999) Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointest Endosc 49:731–735
Noshirwani KC, van Stolk RU, Rybicki LA, Beck GJ (2000) Adenoma size and number are predictive of adenoma recurrence: implications for surveillance colonoscopy. Gastrointest Endosc 51:433–437
Young-Fadok TM (2009) Pro: a large colonic polyp is best removed by laparoscopy. Am J Gastroenterol 104:270–272
Acknowledgment
The authors thank Mr. Aaron Southgate who produced the figures for this article.
Disclosures
N. R. A. Symons, O. Faiz, C. Fraser, S. K. Clark, and R. H. Kennedy have no conflict of interests. Adela Brigic is funded by Ethicon EndoSurgery.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brigic, A., Symons, N.R.A., Faiz, O. et al. A systematic review regarding the feasibility and safety of endoscopic full thickness resection (EFTR) for colonic lesions. Surg Endosc 27, 3520–3529 (2013). https://doi.org/10.1007/s00464-013-2946-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-2946-z