
Abstract
Much progress has been made in the past decade in the understanding of the genetic contribution to the development of human disease in general, and critical care illness specifically. With the mapping of the human genome and on-going mapping of genetic polymorphisms and haplotypes in humans, the field of critical care is now in prime position to study the impact of genetics on common illnesses that affect children who require critical care, to examine how differences of the host defense response lead to variable outcomes in outwardly appearing similar disease states, and to study how genetic differences in response to therapy will help practitioners tailor therapeutic interventions to an individual child’s genetic composition. While we are still years away from true individualized medicine, we are now closer than ever to understanding why two might children respond to the same environmental insult in vastly different ways.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Septic Shock
- Lung Injury
- Angiotensin Converting Enzyme
- Respiratory Syncytial Virus
- Acute Respiratory Distress Syndrome
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Learning Objectives
-
Understand the basics of human genetics, including terminology related to inheritance, predisposition to human disease, and gene expression.
-
Review advances that have been made in the field of human genetic research into the development of critical illness.
-
Identify genetic variants in genes that predispose certain individuals to critical illness, or protect individuals from the development of certain critical illnesses.
Introduction
Much progress has been made in the past decade in the understanding of the genetic contribution to the development of human disease in general, and critical care illness specifically. With the mapping of the human genome and on-going mapping of genetic polymorphisms and haplotypes in humans, the field of critical care is now in prime position to study the impact of genetics on common illnesses that affect children who require critical care, to examine how differences of the host defense response lead to variable outcomes in outwardly appearing similar disease states, and to study how genetic differences in response to therapy will help practitioners tailor therapeutic interventions to an individual child’s genetic composition. While we are still years away from true individualized medicine, we are now closer than ever to understanding why two might children respond to the same environmental insult in vastly different ways.
Before being able to appreciate the advances in research that have been accomplished in relation to the genetic impact on critical illness in children in recent years, it is important to understand the basics of human genetics, and become familiar with the terminology that is utilized to discuss these remarkable advances. Once the genetic basics are clear, discussion can then proceed to genetic associations that have been determined in critical illness in children.
Human Genetics
Structure and Function of Genes
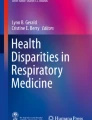
The nucleus of all cells holds chromosomes that contain deoxyribonucleic acid (DNA), the genetic material that is inherited from parents. DNA is responsible for determining the structure of the cell, the function and activity of the cell in response to various stimuli, and the interaction the cell has with other cells and the extracellular environment. The DNA molecule consists of two chains of deoxyribonucleotides held together by complementary base pairs. The deoxyribonucleotides contain the four nucleotide bases, adenine (A), thymine (T), guanine (G), and cytosine (C) that are covalently bound together by phosphodiesterase bonds linking the 5′ carbon of one deoxyribose group to the 3′ carbon of the next group. The two chains of deoxyribonucleotides are linked by hydrogen bonds between the A’s of one strand and the T’s of the other. Likewise, the G’s of one strand are linked by hydrogen bonds to the C’s of the complementary strand. These two complementary strands form the DNA double helix (Fig. 11-1), with one strand running in the 5′ to 3′ direction while the other strand runs in the 3′ to 5′ direction. The order of nucleotides bases is termed the sequence and is read in the 5′ to 3′ direction. The genetic information of an individual is encoded by the precise positioning and order of these base pairs.

The four nucleotides of the DNA double helix (From National Human Genome Research Institute’s Talking Glossary of Genetics (http://www.genome.gov/glossary.cfm#s))
The entire DNA content of an organism is their genome. Every cell of an organism contains two copies of the DNA, with the exception of red blood cells which lack a nucleus and DNA and sperm and egg cells which contain one copy of the DNA. Overall, humans have 46 chromosomes, including 22 pairs of autosomal chromosomes and one pair of sex chromosomes. Each chromosome is made up of a centromere and two telomeres (ends) (Fig. 11-2). The two arms of the chromosome are the short arm (p) and long arm (q). The parts of the genome that contain nucleotide sequences that code for proteins are the genes and it is estimated that the human genome contains about 20,000–30,000 genes. The structure of genes is very complex and highly variable. Genes are made up of a variable number of exons, which contain the actual coding sequence for the proteins, and introns, which are noncoding regions which separate the exons. While the function of the introns is unclear, some disease processes have been found to be associated with certain nucleotide variations located in these intron regions (Fig. 11-3). Genes also have regulatory regions, including promoter sequences that generally reside at the 5′ end of the gene (referred to as upstream) and regions at the 3′ end associated with stability of the mRNA.

The structure of a chromosome (From National Human Genome Research Institute’s Talking Glossary of Genetics (http://www.genome.gov/glossary.cfm#s))

The structure of a gene, including the exons (coding sequence) and introns (noncoding sequence) (From National Human Genome Research Institute’s Talking Glossary of Genetics (http://www.genome.gov/glossary.cfm#s))
Genetic Recombination
Genetic recombination, which is the re-shuffling of genes from generation to generation, is the basis of genetic diversity in sexually reproducing organisms. The analysis of genetic recombination is a useful method of mapping genes in the genome. Genetic recombination results in an exchange of genetic material between homologous chromosome pairs. This results in segments of DNA being exchanged with the other chromosome of the pair, thereby shuffling the genetic material.
The basic principal of linkage analysis, a method used to find disease causing genes, relies on the genetic recombination frequency between two loci on a single chromosome. This allows the estimation of the relative distance between them, and is crucial for the mapping of genes in the genome. Recombination frequencies can be measured by genotyping individuals in a family pedigree. The closer together two loci are on a chromosome, the lower the likelihood of recombination to occur between them. If loci are very close, they are said to be linked. The reliability of genetic linkage between loci is determined using the LOD score, which is an estimate of whether two loci are likely to lie near each other on a chromosome and are therefore likely to be inherited together. A LOD score of 3 or more, which represents odds of 1000:1 or greater in favor of linkage, is used to indicate statistically significant linkage, and therefore concludes that the two loci of interest are close.
The development of genetic maps has been very useful in finding genes which may cause human disease. Genes may be mapped to a particular location in the genome based on being inherited with respect to a marker of known map location, and with the assumption of no genetic recombination. There are a number of polymorphic markers which may be utilized for genetic map construction, including minisatellites, microsatellites, and single nucleotide polymorphism (SNPs). Linkage disequilibrium (LD), often referred to as allelic association, is a measure of physical association between two alleles and occurs when closely linked alleles are inherited together during many generations. No significant degree of genetic recombination occurs between them, and they continue to be passed along together throughout generations. Therefore, knowledge of one marker can be used to study the other.
There are many potential benefits of identifying genes/gene variants involved in disease. These include, but are not limited to, an improved understanding of the disease etiology, insight into the mechanisms of disease pathogenesis, an ability to develop an early disease risk assessment, the potential to discover novel therapeutic drug targets, the ability to estimate the therapeutic response to specific pharmacologic therapies, the possibility of targeted disease prevention strategies to be utilized in high-risk populations based on genetic predisposition, and the movement from the classic symptoms-based disease definition towards a true molecular definition of complex disease processes.
Genetic Mutations
Genetic mutations are changes that occur in the sequence of DNA. Mutations can be classified as somatic mutations, which occur in somatic cells and are not commonly passed on to offspring, and germ-line mutations which occur in the reproductive cells and are passed on to offspring. There are several different types of mutations. Translocations are large-scale mutations comprised of switching of chromosomal regions between one chromosome and another chromosome. Mutations can also consist of single changes in the nucleotide bases and include substitution, deletion, or insertion of nucleotides. Insertions and deletions can also involve hundreds of nucleotides. Mutations that occur in the coding regions can have several consequences: they can change the amino acid of the protein at a single site, they can cause a premature stop codon resulting in early termination of translation, and, consequently, lead to a truncated protein, or they may have no effect at all if the mutation leads to a nucleotide substitution that does not alter the amino acid. Likewise, mutations in noncoding regulatory regions (such as promoters) may also affect the expression of the gene by altering the quantity of mRNA transcribed and, hence, the level of the protein. Mutations in the intron/exon boundary region may also lead to incorrectly spliced mRNAs and result in significantly different proteins or differences in levels of protein products.
The sequencing of the human genome has revealed that most genes are polymorphic; that is, there are small differences in the nucleotide sequences. There are estimates that the human genome may contain over 10 million of these types of variations. These differences in the nucleotide sequence are what give rise to our genetic variability; they account for inherited differences in our physical traits and the way we respond to environmental stimuli and medications. While the majority of these nucleotide variations do not cause a disease, some genetic variations may influence the development of certain diseases. The mutations discussed in the preceding paragraph are variations that occur in less than 1% of the population and are, thereby, rare. On the other hand, variations that occur at a frequency greater than 1% in the population are referred to as polymorphisms. If the polymorphism is a change in a single nucleotide, it is referred to as a single nucleotide polymorphism (SNP). These more common genetic variations, whether SNPs or small insertions or deletions of nucleotides, are the ones currently being examined in many studies for associations with susceptibility to and outcome from diseases seen in the intensive care unit setting. Copy number variations (CNVs) are stretches of DNA of greater than 1 kb that show differences in the expected number of copies of the DNA in greater than 1% of the human population. Very recently it has become clear that CNVs are also common in human genomes and contribute significantly to human genetic variation.
Another important concept in genetics is a locus, which refers to the location in the genome of a specific gene or variant. Keeping in mind the above discussion of genetic variations, a locus may contain two slightly different sequences for a specific gene. These alternative forms of a gene are termed alleles, or variants. The alleles for a specific individual at a genetic locus is that person’s genotype. An example is the surfactant protein B (SP-B) +1580 site. An individual’s genotype at that site may either be TT, CT, or CC. Individuals are heterozygous if they possess two different alleles at the locus of interest and homozygous if they possess two identical alleles at that locus. But we obviously do not contain only one genetic variation in our genome. A haplotype represents a combination of polymorphic alleles on a single chromosome delineating a pattern that is inherited together and transmitted from parent to offspring. Haplotype analysis is a useful tool for analysis of disease gene discovery, as investigators may capitalize on the fact that many of the polymorphisms of interest are not transmitted independently of each other, and the presence of one gene variant can tag the presence of another polymorphism from the same chromosome. In some cases, haplotype assessment can provide a higher level of specificity, sensitivity, and accuracy in “true” associations with disease risk or severity. By focusing on haplotypes as well as SNPs, researchers are now able to more accurately study genetic predisposition to various diseases of interest. With the recent report of the International HapMap Consortium, and the identification and cataloging of haplotypes now available, the utility of this type of study is brought into focus as an important tool to guide genetic association studies on complex human diseases.
Genetic polymorphisms, like the rarer mutations, may also influence the quantity of the mRNA made if present in a regulatory region, or they may also influence the functional activity of the protein product. There has been an explosion of studies attempting to determine if these genetic polymorphisms may account for some of the clinical variability we as clinicians observe at the bedside in the PICU. For example, can the difference in disease severity between two children with pneumonia be associated with variations in their genes coding for one of the surfactant proteins?
Gene Expression
Gene expression is the process by which the information contained within genes is used to make proteins (Fig. 11-4). This occurs by a combination of two distinct processes: transcription and translation. Transcription is the process by which the genetic information in DNA is transcribed into messenger ribonucleic acid (mRNA). mRNA differs from DNA in that it is single-stranded, has a modified sugar backbone, and contains uracil (U) instead of T. The process of transcription involves the unwinding of the two complementary strands of DNA, the enzyme RNA polymerase binding to the promoter region of a gene on a single strand of DNA, and synthesizing the mRNA molecule by adding ribonucleotides in an order that is complementary to the DNA strand. The transcribed mRNA thus contains all the genetic information between the transcriptional start and stop sites on the DNA including exons and introns. The non-coding intron sequences are removed by a process referred to as splicing which connects all the exons together to form the final mRNA product. This mRNA represents the coding DNA sequences for a single gene. (It should be noted that splicing variations have been identified that influence disease processes that impact the final protein product by altering the mRNA sequences that are spliced together.) The mRNA is then transported to the cytoplasm, and translation occurs, in which the genetic information from mRNA is utilized to guide the synthesis of proteins. Proteins are composed of amino acids. There are 20 different amino acids in humans, and each is encoded by a set of 3 nucleotides in the mRNA. These three nucleotides are called triplets or codons. The corresponding anticodon on the transfer RNA (tRNA) links with a codon, presenting its unique amino acid in the process of translational protein synthesis.

Gene expression (transcription and translation), the process by which proteins are synthesized based on the information coded on DNA (From National Human Genome Research Institute’s Talking Glossary of Genetics (http://www.genome.gov/glossary.cfm#s))
Since all cells that contain a nucleus carry the full set of genetic information, it is necessary for gene expression to be selective and tightly controlled, in a way that guarantees specific proteins are expressed in specific cells under appropriate conditions. This differential expression of genes ensures that cells develop correctly, can differentiate and function as specialized cells, and can mount various responses to external stimuli. In certain disease states, expression of specific genes may change, thereby providing a clue as to which genes may be important in that disease process. Recent advances in technology have provided a valuable tool to evaluate the expression of genes during various diseases, including sepsis. These technologies include DNA microarrays, in which the basic approach is as follows: small strands of DNA probes representing the genes of interest, for example, tumor necrosis factor alpha (TNF-α), are attached to a solid substrate such as a glass slide or silicon chip (in reality, thousands of probes are applied to the same micorarray chip). mRNA is then isolated from, for example, a patient without acute lung injury (ALI) and one with ALI. These two samples are then separately converted to complementary DNA (cDNA) in a manner which incorporates different fluorophores in the two samples of cDNA (e.g., red into all the cDNAs from the patient with ALI which would also include cDNA made from the mRNA coding for TNF-α, and green into all the cDNAs from the patient without ALI including the cDNA made from the mRNA coding for TNF-α). The cDNAs from the two patients are then mixed and hybridized to the chip containing the DNA probes. Thus, if TNF-α is up-regulated in ALI and there is significantly more cDNA in the ALI sample than the non-ALI sample, then more red fluorophore –labeled cDNA would be present. When the mixture of cDNAs is hybridized to the chip containing the probes, the probe for TNF-α would light up red and represent increased expression of the TNF-α gene in ALI. If TNF-α is expressed at a lower concentration in the patient with ALI then when the samples are mixed, more green fluorophore-labeled cDNA would be present than red fluorophore-labeled cDNA, and the probe for TNF-α on the microarray chip would light up green indicating decreased expression of TNF-α gene in ALI. Finally, if there is no change in the expression of the TNF-α gene, the amounts of red and green fluorophore-labeled cDNAs would be equal, and the probe for the TNF-α gene would light up yellow. In this fashion, one can identify specific genes that are expressed in the development of ALI. Several examples of the use of this technology in the critically ill patient have been published which have aided our understanding of the pathophysiology of certain ICU specific diseases.
Phenotype
Up to this point, we have discussed the structure of DNA and the process of getting from the code in the DNA to protein. It is the functional aspects of these proteins that give rise to the observed traits, whether it be the color of one’s eyes, the rate of metabolism of a drug, or the efficiency with which a protein receptor on a cell surface recognizes a pathogen. The observable characteristics of an individual define that individual’s phenotype. This may include common physical and biochemical characteristics, but can also describe a person’s disease status (such as in cystic fibrosis). Phenotypes caused by mutations in a single gene may show Mendelian inheritance patterns. These patterns can be autosomal dominant (where a single copy of the gene causes the phenotype), autosomal recessive (where both copies of the gene are necessary for the phenotype), or sex linked (where the mutation occurs on the X chromosome). It is crucial to note that Mendelian inheritance patterns are only seen for single gene disorders. Critical care diseases and syndromes, such as sepsis and acute respiratory distress syndrome (ARDS), are complex disorders whose genetic predisposition to the development of the disease is due to multiple genes and other factors, such as environmental exposures. The multifaceted gene-gene and gene-environment interactions make the study of these diseases extremely complex.
Genetics of Common Complex Disorders
There are many common complex disorders that display obvious familial aggregation of cases, but have no clear Mendelian inheritance patterns. The most commonly studied in medicine are cancer, diabetes, hypertension, and obesity, among others. The disease aggregation may be due to complex genetic factors, the interaction of multiple genes on the development of the disease of interest, a host of environmental factors which place the individual at risk for the disease, or, most commonly, a combination of all of the above factors (Fig. 11-5). In other words, a person’s genetic background may make them prone to a specific disease; this is called susceptibility gene variants or susceptibility genes. Due to their inherited genetic make-up, the individual is at a higher inborn risk for developing the disease of interest, but only if they are exposed to the environmental stressor that is known to associate with the disease. The susceptibility gene variant will not directly lead to the disease, but will put that person at a higher risk if they are exposed to the environmental risk. For example, individuals may possess a susceptibility gene variant for the development of lung cancer, but this will only lead to the development of cancer if they are subject to a known environmental risk factor, such as smoking. Alternatively, a newborn may possess one or more susceptibility gene variants for the development of bronchopulmonary dysplasia, but if they are not born prematurely and do not require mechanical ventilation in the newborn period (and therefore are not subject to the environmental stressors known to impact the development of this lung disease), they will never develop this disease despite being genetically susceptible.

The complex interactions that can occur between genes that may impact a disease process (gene-gene interaction) as well as between the genes of interest and environmental factors (gene-environment interaction)
Gene variants can also decrease the susceptibility, or increase the resistance against a disease. These are protective gene variants. To give an example, there are individuals who smoke their entire adult lives and yet never develop chronic obstructive pulmonary disease. It is likely that these individuals possess protective gene variants against the development of this disease, even in the face of a strong environmental insult. A person may possess both susceptibility and protective genetic variants for the same disease, and the mix of these variants will impact together the overall genetic risk of that person to the disease of interest. This resultant genetic risk also interacts with the environmental risk of the individual, leading to the overall risk of that person developing the disease. In critical care, it is unlikely that one gene will cause the diseases that are treated in the intensive care unit; it is more likely that multiple genes will interact with multiple environmental insults to predispose individuals to diseases processes resulting in an overall risk for an individual patient to develop a certain disease of interest. Interestingly, certain populations seem to be immune to certain complex diseases. Examples include the Australian aborigines and Inuits from Greenland, in which both populations appear to be resistant to the development of type 1 diabetes. It is plausible that the disease resistance observed in these populations is due to absence of susceptibility gene variants or presence of protective gene variants in the group’s gene pool.
When it is determined that a complex disease has familial aggregation, it is important to take into account that families may also share environmental or social factors that predispose to the disease of interest, and therefore the entire impact may not be genetic. One example would be radon gas present in a neighborhood leading to an increased incidence of lung cancer in families living in close proximity. While it may be assumed that the genetic impact is responsible for the development of the disease, environmental exposure is the likely source. Twin studies and adoption studies are utilized to attempt to determine the relative weight of genetics and environment in the development of a certain disease.
Genetic Studies in Critical Care
Genomic medicine and the concept that an individual’s genetic makeup may influence not only the severity of and outcome from their critical illness, but also their response to the therapies, has begun to makes it’s way into the intensive care unit. This section will highlight studies involving analysis of gene expression and genetic association studies in patients with critical illness. While it may appear that advances have been made in the field, it is important to understand that we are not yet in the age of personalized medicine and much work needs to be done.
Gene Expression Studies in the ICU
The expression of specific genes in many cases represents the body’s specific and complex response to environmental stimuli, such as in the case of a severe infection, trauma, or cardiopulmonary bypass. Examining gene expression may, therefore, provide a clue as to which genes are important in a specific critical illness. Many studies have examined gene expression in critically ill patients, but most examine the expression of only a few genes. With the advent of the DNA microarray technology discussed above investigators have begun to explore gene expression patterns in thousands of genes in children with septic shock using mRNA isolated from whole blood representing the gene expression response in circulating white blood cells. These studies have compared gene expression from blood samples obtained within 1 day of admission to the PICU with that observed in blood of healthy controls, examined longitudinal changes in gene expression in children with septic shock (days 1 and 3) and compared expression in patients with septic shock to expression in children with sepsis or systemic inflammatory response syndrome (SIRS). Genes that were up-regulated, down-regulated, or unchanged between the groups were examined. The genes that were up-regulated when the septic shock group was compared to healthy controls included genes related to immunity and inflammation as would be expected. Unexpectedly the study demonstrated that many genes related to zinc biology and zinc homeostasis were down-regulated. The significance of this finding was supported by the observation that children who did not survive septic shock had lower serum levels of zinc and the demonstration in a murine model that zinc depletion leads to increased mortality from sepsis. In addition, genes involved in T-cell receptor signaling and antigen presentation appeared decreased suggesting that septic shock may be associated with depression of the adaptive immune system. Interestingly expression studies of adults with sepsis and septic shock did not identify a down-regulation of genes related to zinc biology although up-regulation of genes related to immunity and inflammation and down-regulation of genes related to the adaptive immune system was observed.
The longitudinal study in children with septic shock demonstrated that in general the observed changes in up-regulated and down-regulated gene expression persisted over time. In addition, the study comparing expression in children with shock to those with sepsis or SIRS indicated that while there were patterns of expression that were similar in all three groups (such as genes involved in innate immunity that were up-regulated) there were genes that were unique to the septic shock group with relation to the degree, and duration, of the response. Examples include the finding that up-regulated genes that were involved in the IL-10 signaling pathway had a greater signal which persisted for longer in the septic shock patients and down-regulation of genes for zinc biology and the adaptive immune system was greater and lasted longer than that seen in the other two groups. In addition to providing insight into the pathophysiology of sepsis and identifying potentially important proteins in early sepsis, the use of this technology may also provide physicians with a unique diagnostic tool. If the gene expression profile of a patient who is in the early stages of sepsis is different from a patient who exhibits SIRS but does not develop sepsis, then earlier therapies could be initiated before full blown sepsis is clinically evident. There is also some evidence that various subclasses of sepsis and septic shock may be able to be identified using this technique.
DNA microarrays have also been used to investigate the expression profile in adults with ALI. mRNA for pre-B-cell colony enhancing factor (PBEF), a cytokine that is involved in the maturation of B-cell precursors, inhibition of neutrophil apoptosis, and perhaps regulation of endothelial cell calcium-dependent cytoskeletal arrangement was noted to be significantly increased in adults with ALI, a finding that was also consistent in both a canine and mouse model of ALI. In addition to the elevated mRNA levels, PBEF protein in bronchoalveolar lavage fluid was also elevated in adults with ALI. It is also worth mentioning an important study in a canine model of lung injury to highlight the value of gene expression arrays. The use of mechanical ventilation is invariably needed to treat patients with ALI though the use of positive pressure ventilation itself may exacerbate the lung injury. Gene expression arrays in a canine model of ventilator associated lung injury have identified a number of genes that are regulated during ALI. Many of the genes can be grouped into biological processes known to important in the pathophysiology of ALI; these include inflammation (e.g., IL-1b, IL-6, IL-1ra, MMIF), coagulation (tissue factor, PAI-1), and chemotaxis/cell motility (myosin light chain kinase, cell chemokine receptor 2). Several other genes also appeared to be expressed including PBEF, heat shock protein 70 (HSP 70), and vascular endothelial growth factor (VEGF). Thus, the use of expression arrays has identified a number of candidate genes that may play important roles in the development of ALI. As will be discussed below, genetic variations that influence the activity or level of the protein in several of these candidate genes have been examined in gene association studies in patients with ALI.
Genetic Predisposition in the PICU
As described above, a large amount of genetic variability exists throughout our genome. Whether these differences influence the susceptibility to or outcome from diseases in the critical care setting is an area receiving a great deal of interest. Perhaps the greatest amount of focus of genetic association studies on critical illnesses is in sepsis and ALI. The general approach has been to compare the frequencies of polymorphisms in specific candidate genes between a cohort of patients with sepsis or ALI and an at-risk cohort without sepsis or ALI. This section will review some of these studies.
Influence of Genetic Variation in Patients with Sepsis
Individual variability in the susceptibility to and outcome from sepsis and lung injury has long been observed in critically ill patients. Why one child with pneumococcal pneumonia has little consequence of their infection and can be treated as an outpatient while another child develops refractory septic shock and respiratory failure has been attributed to a number of factors. These have included virulence of the pathogen, length of time between onset of symptoms and appropriate treatment, and comorbid conditions. While all these certainly contribute to the severity of disease, a growing body of evidence suggests that genetic variations in the individual patient may also contribute to the severity of and outcome from critical disease. These genetic polymorphisms may not be of any consequence during normal healthy periods but their importance may only become evident during a severe stressor such as an infection, trauma, cardiopulmonary bypass, or other scenarios seen in the intensive care unit (Table 11.1). A strong genetic influence on the outcome from infections was indicated by a family based study of adoptees. Adoptees with a biological parent who died due to infection before the age of 50 had a relative risk of death due to infection of 5.81 (CI = 2.47–13.7); a higher relative risk than that seen when risk related to early death of a biologic parent due to cardiovascular and cerebrovascular disease (4.52; 1.32–15.4) or cancer (1.19; 0.16–8.99) was examined. Thus, an individual’s genetic makeup may influence the severity of disease in infection and sepsis.
Given the tens of thousands of genes in the human genome and the millions of genetic polymorphisms, on which polymorphisms and in which genes should investigators focus? One approach in choosing the candidate gene is to examine the pathways by which pathogens lead to the clinical symptoms of sepsis. The body’s response to infections involves recognition of pathogen-associated products followed by an inflammatory response that involves a large number of cellular proteins. Genetic variations that lead to alterations in the amount or functional activity of any of these proteins involved in the recognition of or response to pathogen-associated products may influence the individual’s response. Examples of the influence of genetic variations in proteins involved in recognition of pathogens on the severity of infections include polymorphisms in the genes coding for mannose binding lectin (MBL), the receptor for Fcγ, and toll-like receptor (TLR) 4. The heterotrimeric MBL is involved in binding bacterial surface carbohydrates and the opsonization of bacteria. A helical domain in the tertiary structure of the protein is crucial for formation of the active heterotrimer. Three genetic polymorphisms in the gene coding for MBL result in amino acid changes in the helical tails of the protein and result in increased degradation and decreased serum levels of MBL. Genetic association studies have demonstrated associations between the 3 MBL genetic polymorphisms and increased susceptibility to infections, hospitalizations due to infections, number of acute respiratory infections, and risk of meningococcal infections in children, and pneumonia and sepsis in neonates. In adults these polymorphisms have been associated with recurrent respiratory infections, invasive pneumococcal infections and viral coinfections with pneumococcal pneumonia.
The family of leukocyte Fcγ receptors is also involved in the recognition of bacteria such as Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitides. Fcγ receptors bind the Fc portion of IgG bound to bacteria, thereby facilitating phagocytosis and inducing the inflammatory response. Several polymorphisms have been described in the genes coding for the various Fcγ receptors that alter their binding affinity to the various subclasses of IgG. Two such polymorphisms have been described in the genes coding for the FcγRIIIb receptor and the FcγRIIa receptor. In the case of the FcγRIIIb receptor, the genetic polymorphism results in a four amino acid substitution (allotypes FcγRIIIb-NA1 or -NA2) in the receptor that alters the opsonization efficiency. In the case of the FcγRIIa receptor, the genetic polymorphism results in replacing a histidine for an arginine in the extracellular domain of the receptor at amino acid position 131. The variant FcγRIIa receptor containing the histidine binds the Fc region of IgG2 with a lower affinity and results in reduced phagocytocytosis in vitro compared with the more common FcγRIIa receptor containing the arginine. In association studies, a higher frequency of individuals homozygous for the NA2 allotype of the FcγRIIIb receptor or an arginine at position 131 in the FcγRIIa receptor was found in patients with severe meningococcal disease or fulminant meningococcal sepsis.
The final examples of genetic variation in genes coding for pathogen recognition products influencing the severity of sepsis are the polymorphisms in the gene coding for the TLR4 receptor. This receptor is a component of a complex that includes CD-14 and myeloid differentiation (MD)-2 that binds lipopolysaccharide (LPS), one of the major cell wall components of Gram negative bacteria. In addition, TLR4 recognizes the F protein of the respiratory syncytial virus (RSV). Two genetic polymorphisms have been identified in the gene coding for TLR4 that result in the change of a threonine for a glycine at amino acid position 299 and a threonine for a isoleucine at amino acid position 399. The Gly299Ile399 variant form of the receptor appears to be expressed on the cell surface in lower amounts and result in a lower systemic cytokine response to LPS and RSV. Genetic association studies have demonstrated an association between the TLR4 Gly299Ile399 variant and Gram negative bacterial infections and septic shock as well as mortality in patients with systemic inflammatory response syndrome. However, a number of studies have also shown conflicting results. These TLR4 variants have also been reported to be associated with susceptibility to and severity of respiratory syncytial virus infections in children. Future studies with more participants will be required to determine whether variations in the TLR4 gene are involved in infection and/or severity of disease.
Thus far, the focus has been on genetic variations in genes coding for proteins involved in pathogen recognition, and in each case, the variation results in an inferior host response resulting in more severe disease. Currently it is thought that severe sepsis and septic shock may be the result of an imbalance in the inflammatory response. The mechanism by which this imbalance occurs is thought to be multi-factorial. One possibility that has attracted much interest is that the host may harbor genetic variations in the regulatory regions of genes involved in the response to noxious stimuli resulting in an imbalance between pro- and anti-inflammatory cytokines. These variations can result in an over-expression of pro-inflammatory cytokines, such as TNF-α and interleukin (IL)-6, or an under-expression of anti-inflammatory cytokines, such as IL-10. In either case, the normal inflammatory response is dysregulated.
One of the pro-inflammatory genes in which genetic polymorphisms influence expression is TNF-α. As a key pro-inflammatory cytokine, TNF-α is responsible for the activation of the inflammatory response and by itself can produce many of the clinical manifestations of sepsis such as capillary leak, hypotension, and multiple organ dysfunction syndrome. The regulatory region of the gene coding for TNF-α has several polymorphisms that alter transcription of TNF-α, thereby influencing the amount of TNF-α produced. Several of these polymorphisms alter nucleotides which make up the recognition sequences of some of the transcription factors that regulate transcription. Two of these polymorphisms in particular have been studied. The rarer A allele (TNF-α-308) at a location 308 base pairs upstream from the transcriptional start site results in greater transcription than the more common G allele. A second rare A allele (TNF-α-238) at a location 238 base pairs upstream from the transcriptional start site results in lower transcription than the G allele. In addition, another site located ∼3,200 base pairs upstream from the transcriptional start site of the TNF-α gene and located in the gene coding for another gene, lymphotoxin (LT)-α, (also referred to as the TNFB allele, TNF-β + 252, and LT-α + 250) also appears to regulate transcription of the TNF-α gene. In genetic association studies, the frequency of the TNF-α-308 A allele has been shown to be higher in children who died from meningococcal infections and adults who died with septic shock compared with controls. Genetic association studies examining the influence of the polymorphic LT-α + 250 site has shown a higher frequency of the A allele in adults with pneumonia presenting with the clinical symptoms of sepsis, in adults in post-operative and trauma intensive care units who develop sepsis and who have a higher mortality, and in bacteremic children who exhibit higher serum TNF-α levels and have a higher mortality. However other genetic association studies examining the TNF-α gene have reported conflicting results. Recently a well designed, prospective study examining a number of polymorphisms in the gene for TNF-α (including those described above) in adults with trauma admitted to the ICU demonstrated that the A allele of TNF-α-308 was associated with elevated TNF, sepsis syndrome and death in trauma patients both in their initial cohort and a replication cohort. The gene for IL-6 (another pro-inflammatory cytokine) also contains variations which multiple studies suggest are associated with the susceptibility to or outcome from sepsis.
As mentioned above, the progression to severe sepsis is believed to be an imbalance in the pro- and anti-inflammatory mediators. In addition to polymorphisms that result in increased levels of pro-inflammatory cytokines, examples of polymorphisms that result in lower levels of anti-inflammatory cytokines also exist. IL-1 receptor antagonist (IL-1ra) is one of the body’s mechanisms for keeping the inflammatory reaction in check by binding to the IL-1 receptor without activating the signal transduction pathway. The gene coding for IL-1ra contains a polymorphic region consisting of a variable number of 86 base-pair tandem repeats. These different IL-1ra alleles have been associated with variable circulating levels of both IL1-ra and IL-1β (the two genes are located close to one another on chromosome 2), and several association studies have suggested an influence of this variation on a variety of diseases in which inflammation plays an important role, including the susceptibility to sepsis. IL-10 is another anti-inflammatory cytokine for which genetic polymorphisms appear to alter transcription levels. A number of studies have demonstrated an association between an increased susceptibility to sepsis and certain IL-10 polymorphisms although conflicting results have also been reported.
It is important to remember that the cytokines and their receptors mentioned above activate a complex signal transduction pathway composed of dozens of proteins with the end result of a well coordinated cellular response to the noxious stimulus. Genetic variation in any of the proteins in the pathway may also influence the final response. Recent studies have begun to analyze components of various pathways involved in the development of sepsis. One example is IL-1 receptor-associated kinase-1 (IRAK-1) that plays an important role in the signal transduction pathway initiated by the activation of the IL-1 receptor. Activation of IRAK-1 results in increased transcription of a variety of pro-inflammatory genes modulated by NF-κB, a key transcription factor in the inflammatory response. Genetic variations in the gene coding for IRAK-1 have been shown to be associated with elevated nuclear levels of NF-κB as well as the presence of shock and a higher 60-day mortality in patients with sepsis. The association of a variant in IRAK-I with severity of septic shock has been independently replicated in a large multi-centered cohort of adult patients with septic shock. Interestingly, this study also indicated that age might modify the relationship as this association was stronger for younger patients. Many other proteins involved in these complex signaling pathways have yet to be investigated for the influence of genetic variations on critical illnesses.
Many of the genes discussed thus far have a role in inflammation, a key component in the pathophysiology of sepsis. Loss of homeostatic mechanisms regulating the coagulation/fibrinolytic system also plays an important role in sepsis. Plasminogen activator inhibitor 1(PAI-1) inhibits fibrinolysis thereby favoring the formation of microthrombi in the capillaries. The pathophysiology of multiple organ dysfunction syndrome in patients with sepsis is thought to involve, in part, intravascular fibrin deposition. Thus, elevated PAI-1 activity could contribute to organ failure in sepsis and elevated plasma concentrations have been observed in patients with sepsis. A genetic variation in the gene coding for PAI-1 consisting of either the presence of 4 guanines or 5 guanines at a specific location appears to influence the amount of PAI-1 produced. Individuals homozygous for the 4G genotype (4G/4G) produce more PAI-1 than individuals homozygous for the 5G genotype (5G/5G) or individuals that are heterozygous (4G/5G). Association studies have demonstrated that children with meningococcal disease who were 4G/4G at this site had an increased risk of death compared to children who were 4G/5G or 5G/5G. More recent studies in both children and adults have demonstrated higher mortality in individuals homozygous for the 4G allele in a number of infectious diseases. Since fibrin deposition is thought to play a role in the multiple organ system failure in patients with sepsis, genetic variations that influence the production of fibrin might also influence the severity of disease in patients with sepsis. The production of fibrinogen, the precursor to fibrin, is dependent on the transcription of fibrinogen-beta. Several polymorphisms in the promoter region have been associated with higher plasma levels of fibrinogen, and higher levels of fibrinogen have been associated with improved outcomes in sepsis. Association studies have demonstrated that the GAA haplotype, consisting of the genotypes at the −854, −455, and +9006 sites, is associated with higher levels of fibrinogen and with decreased mortality and less organ dysfunction. Protein C has anticoagulant activity as well as anti-inflammatory and anti-apoptotic effects suggesting that diminished activity of protein C may lead to increased fibrin deposition, inflammation, and apoptosis. Genetic polymorphisms located in the promoter region of the gene coding for protein C result in decreased levels. Association studies in Caucasian and Han Chinese adults have demonstrated increased mortality and organ dysfunction in adults with sepsis who carry the A allele at the −1641 site and the C allele at the −1654 site. This haplotype has also been reported to be associated with decreased protein C concentration. Interestingly, an increased risk of more severe sepsis has been observed in children less than 1 year of age with meningococcal disease who carry the G allele at the −1641 site along with the C allele at the −1654 site. This haplotype was not associated with severe sepsis in older children suggesting a potential developmental difference in these variations on the severity of sepsis.
Influence of Genetic Variation on Acute Lung Injury and Acute Respiratory Distress Syndrome
Severe lung injury in both adults and children can be precipitated by a diverse array of causes and are classified as either direct injury when the insult is from the alveolar side of the alveolar/capillary membrane or indirect injury when the insult is from the capillary side. Major causes of direct lung injury include pneumonia, aspiration, pulmonary contusion, and inhalation while major causes of indirect injury include sepsis, trauma without pulmonary contusion, cardiopulmonary bypass, and multiple transfusions. Despite these various causes, the central pathogenesis of ALI involves derangements in multiple biological processes. These include activation of inflammation, loss of coagulation and fibrinolytic homeostasis, disruption of vascular permeability, epithelial and endothelial cell apoptosis as well as proliferation, and derangements in surfactant. Some of these processes, notably inflammation and coagulation, play key roles in the pathophysiology of sepsis as well as ALI. Thus, it is not surprising to find that the candidate genes examined in genetic association studies for ALI are in many cases the same as those examined in sepsis (Table 11.2). This section will review some of the genetic association studies examining the influence of genetic variations on the development of ALI.
Pulmonary surfactant is synthesized by the type II alveolar epithelial cells and is required for normal lung function. One of surfactant’s primary functions is to lower the surface tension at the alveolar air-liquid interface. Surfactant is composed of phospholipids and four proteins, surfactant protein (SP)-A, SP-B, SP-C, and SP-D. Knockout models in mice have demonstrated that of these four proteins, only SP-B is absolutely required for post-natal survival. Deficiency in, or impaired activity of SP-B appears responsible for a number of interstitial pulmonary diseases in humans including ARDS. Several genetic variations exist in the genes coding for the surfactant proteins and two will be discussed here; the SP-B + 1580 T/C polymorphism and insertion/deletion polymorphism consisting of dinucleotide (CA) tandem repeats in intron 4. Several studies have demonstrated an association between these polymorphisms and the need for mechanical ventilation in children (SP-B + 1580 T/C) and mechanical ventilation and ARDS in adults (SP-B + 1580 T/C polymorphism and insertion/deletion of dinucleotide (CA) tandem repeats). The consequences of these variations are not fully known. The SP-B + 1580 T/C polymorphism results in an amino acid change in exon 4 in a region of the amino terminal propeptide which is thought to play a role in targeting of SP-B to lamellar bodies. The resulting amino acid change alters glycosylation of SP-B and may affect the level of SP-B by altering its processing or stability. Aberrant proteolytic processing of the SP-B product encoded by the C allele is supported by a recent report demonstrating that the C allele is associated with absence of a specific pro-SP-B cleavage product in neonates. The intron 4 dinucleotide repeat length variation polymorphism is associated with incompletely spliced SP-B mRNA. Interestingly, in Caucasians this length variation polymorphism in intron 4 is in linkage disequilibrium with the SP-B + 1580 T/C polymorphism; the C allele of rs1130866 is associated with the deletion variants at the intron 4 polymorphic site. Further work is needed to not only define the consequence of these genetic variations on surfactant function but also to further evaluate whether these genetic variations influence the development of ALI.
Another study of interest involves the susceptibility to pneumonia, the leading cause of ALI and ARDS in both children and adults. As discussed above, the 4G/4G genotype in the gene coding for PAI-1 is associated with higher levels of PAI-1 expression. In a large cohort of adults, those individuals with the 4G allele demonstrated a significantly higher susceptibility to pneumonia. While PAI-1 activity inhibits fibrinolysis leading to formation of microthrombi, it also demonstrates anti-inflammatory activity, and in this fashion, may increase the susceptibility to infection. In patients with ALI, plasma levels of PAI-1 levels are elevated and protein C levels are diminished. In addition, alveolar levels of PAI-1 are elevated suggesting a possible local activation of the fibrinolytic system. Recent studies have demonstrated that the 4G allele of PAI-1 is associated with increased mortality in patients with severe pneumonia and patients with ARDS. To date there are no reports indicating association of specific protein C variants with ALI.
Inflammation is one of the hallmarks of ALI and as with sepsis, it is thought that one of the central components of ALI is an imbalance between pro- and anti-inflammatory cytokines in the lung. The influence of genetic variation in several genes involved with inflammation on the development of ALI has been examined. The TNF-α-308 A allele appears to be associated with increased mortality in adults with ARDS but not with the susceptibility to ARDS when compared with adults who were at-risk for the development of ARDS. The LT-α + 250 polymorphism that appears to be associated with more severe sepsis did not influence the severity of ARDS.
Macrophage migration inhibitory factor (MIF) plays a central role in regulating the inflammatory response by directly increasing TNF-α and IL-8 and countering the anti-inflammatory actions of glucocorticoids. MIF mRNA has been demonstrated in cells from bronchoalveolar lavage of patients with ALI and MIF concentrations in serum are elevated in patients with ALI compared with controls. Haplotypes composed of polymorphisms in the 3’ end of the gene coding for MIF are associated with the development of ALI in both Caucasian and African American populations. A number of studies have demonstrated association of specific haplotypes in another gene involved in the regulation of inflammation, the gene for IL-6, with the development of ALI. Whether these haplotypes are associated with elevated levels of IL-6 is still unclear. Association studies have also been performed examining the genetic variants discussed earlier in the promoter region of the anti-inflammatory cytokine IL-10. The −1082 GG genotype results in higher levels of IL-10 and is associated with the development of ARDS in younger adults. Furthermore, the adults with ARDS who carried the GG genotype at this site demonstrated lower mortality and organ failure.
The genetic variants in the gene coding for MBL have also been examined for their influence on ALI. One of the variants described previously that results in decreased serum levels of MBL, variant B, is associated with the susceptibility to ARDS and a greater degree of organ dysfunction and higher mortality in patients with ARDS. While no reports have described the TLR4 polymorphisms specifically in ALI or ARDS, the Gly299Ile399 variant form of the receptor is associated with an increased risk of severe RSV bronchiolitis and increased risk for hospitalization for RSV in previously healthy infants suggesting a potential role for TLR4 in influencing the severity of lung injury.
Signal transduction pathways activated after stimulation of a variety of immune receptors including the TLRs and members of the family of IL-1 and TNF receptors result in the up-regulation of specific genes involved in the innate and adaptive immune responses. Several transcription factors are involved in this process and genetic variation in any of these factors may influence the level of transcription. One such factor is nuclear factor κB (NF-κB) which under non-stimulated conditions is inhibited by the cytoplasmic inhibitor NFκBIA. Upon activation of cytokine-mediated signal transduction pathways, NFκBIA is degraded allowing NF-κB to translocate to the nucleus. A number of polymorphisms located in the promoter region of the gene coding for NFκBIA have been described but their functional consequence is unknown. When individual NFκBIA promoter polymorphisms were examined to determine if they are associated with the development of ALI, none by themselves demonstrated an association. However, the haplotype of −881 G/−826 T/−297 C was found in a higher frequency in adults who developed ARDS especially in males with direct lung injury. Another transcription factor is NF-E2 related factor 2 (NRF2) which, under non-stressed conditions, is located in the cytoplasm. Under oxidative stress NRF2 translocates to the nucleus and results in transcription of several anti-oxidant enzymes. Several polymorphisms within the promoter region of the gene coding for NRF2 have been identified that reduce transcription. One such variant, −617 A allele, is associated with the development of ALI in adult trauma patients.
The role of angiotensin converting enzyme (ACE) in lung injury has recently attracted uch interest. ACE is present in pulmonary endothelium and is responsible for converting ATI to ATII. ACE levels are elevated in the bronchoalveolar lavage fluid of adults with ARDS and higher levels are associated with mortality from ARDS. The key component is most likely ATII, which has apoptotic effects on alveolar epithelial and endothelial cells in vitro. ATII receptor antagonists block pneumocyte apoptosis in a model of meconium aspiration. Another important component of this system is ACE2, a homologue of ACE expressed in human lungs, which is a negative regulator of the renin-angiotensin system as well as the probable receptor for the SARS virus in humans. Lung injury models using knockout mice lacking the ACE2 gene have higher ATII levels and exaggerated lung injury compared to wild type mice. However, the lung injury is reversed if the ACE gene is inactivated in the ACE2 knockout mice. This suggests that ACE induces lung injury through ATII and that ACE2 protects against lung injury. Indeed, ACE inhibitors and ATII antagonists appear to decrease the severity of lung injury in animal models, the risk of aspiration pneumonia in some adult populations, and reduce the 30-day mortality in adults with pneumonia. Several studies have demonstrated the D/D genotype appears associated with the susceptibility to and outcome from ARDS.
As discussed previously, expression microarrays have been invaluable in identifying other potential mediators involved in the pathophysiology of lung injury. The expression of pre-B cell colony enhancing factor (PBEF) was found to be significantly elevated in both animal and human studies of ALI using this approach. PBEF is a lesser studied cytokine involved in the maturation of B-cells, inhibition of neutrophil apoptosis, and perhaps regulation of the endothelial cell calcium-dependent cytoskeletal arrangement. Two genetic polymorphisms have been identified in the promoter region, −1001 T/G and −1543 C/T which appear to influence the development of ALI. Carriers of the G allele at position −1001 had a 2.75-fold increased risk of ALI and the G allele remained an independent risk factor after controlling for several other variables. The T allele at position −1543 was found at a lower frequency in adults with ALI. Combining these two polymorphisms in a haplotype analysis demonstrated that adults with the −1001 G/ −1543 C haplotype had a higher risk of ALI (7.7 fold). The consequence of these two polymorphisms remains to be elucidated though the −1543 T allele may result in reduced expression.
One final gene to be discussed in this section is the myosin light chain kinase (MLCK) gene. Three isoforms of the protein exist, and one isoform is a key component in the cytoskeletal arrangement regulating vascular permeability, angiogenesis, endothelial cell apoptosis, and leukocyte diapedesis. Several polymorphisms in the gene coding for MLCK have recently been identified. Analysis was performed not only on the influence of single polymorphisms on the development of ALI but also a number of haplotypes using a sliding window approach. Several strong associations between various single nucleotide polymorphisms as well as haplotypes and the risk of ALI and sepsis were identified in adults. This included one haplotype, GGT, composed of markers MYLK_021, MYLK_022, and MYLK_011 spanning a region of 846 base pairs between the 5′ untranslated region and the first exon that appeared to be specifically associated with the risk of ALI and not sepsis. The functional significance of these haplotypes remains to be determined. Specific variants in the MYLK gene were also shown to be associated with trauma-induced ALI, however association of specific genetic variants and lung injury were not observed in children or adults with pneumonia.
Other Potential Areas of Interest in Genetic Variation in the PICU
Two other areas should be mentioned in regards to the influence of genetic variations in the PICU. The first is in the area of coagulation. Several examples of genetic polymorphisms in genes coding for proteins involved in coagulation and fibrinolysis were discussed above in relation to sepsis and ALI. However, these and many other genetic variations that exist in other components of the coagulation cascade could also influence the development of thrombosis including deep venous thrombosis in critically ill patients. Thrombosis of central venous catheters is a recurring problem in PICUs and while certain environmental factors play a role (eg, length of time catheter is in place, size of the patient and vessel), genetic polymorphisms in the patient favoring the formation of thrombi may also play a role.
Finally, the action of every drug that is used in the PICU can potentially be influenced by genetic variation in the patient. Whether it be inhaled β2-agonists, or the array of intravenous vasoactive agents, sedatives, muscle relaxants, antibiotics, steroids, etc.; all bind to protein receptors and either activate or block specific signal transduction pathways, many bind protein carriers or transporters, and most are metabolized by various protein enzymes. Every gene coding for each of these proteins has multiple genetic variations with the potential to influence the levels or activities of these proteins. The area of pharmacogenomics attempts to determine the influence of genetic variations in genes affecting these various aspects of drug action. However, while the list of genetic polymorphisms in genes affecting drug action is growing rapidly, there are few clinical examples of the degree of influence that these genetic variations have on the response to drugs in the PICU. For example, warfarin is the most widely used oral anticoagulant for long-term prophylaxis and treatment of thromboembolic disorders and is used in many children and adults with mechanical valves. The metabolism of and response to warfarin involves several enzymes, two of which exhibit genetic variations that dramatically alter the levels of warfarin. For one of these genes, CYP2C9, the common allele is referred to as CYP2C9*1 and is consider the wildtype while CYP2C9*2 contains a C to T nucleotide change at position 430 in exon 3 and CYP2C9*3 contains an A to C nucleotide change in exon 7. CYP2C9*2 has approximately 80% of the metabolic activity of the wild type CYP2C9*1 while CYP2C9*3 contains only 20% of the wildtype activity. By also using genetic variation in a second gene, vitamin K epoxide reductase complex subunit 1 or VKORC1, one can account for more than 50% of the observed dosing variability. Current practice in the use of warfarin usually involves starting at an age and weight specific dose and monitoring coagulation studies. However, because of the genetic variations in these two enzymes and perhaps others, different patients take different amounts of time to achieve the appropriate therapeutic dose. Knowing the specific genotypes of patients prior to initiating warfarin may allow for more appropriate dose selection, less time to achieve therapeutic levels, and less risk of adverse events. Recently, an algorithm using the patient’s genotypes at these two sites has been developed that allows for more accurate dosing in some populations. Although these algorithms are being developed and tested it should be kept in mind that they do not account for drug-drug interactions.
Conclusions
The era of the study of the genetic impact on critical illness in children is present. Clinicians must be prepared to deal with the growing body of literature related to genetic influence on critical disease development, treatment and outcome, and be able to critically review the literature in order to determine the impact on the patients they are caring for daily. For the results of these representative genetic association studies to take the leap into clinically impacting care, they must meet certain criteria. First and foremost, the phenotype must be well defined; that is, the enrolling patients with ALI/ARDS or sepsis must meet strict and well accepted criteria. Second, they must be high quality studies, utilizing highly sensitive and specific methods for genotyping. Third, the studies must use a large sample size to assure that no type I or type II errors are made based simply upon the number of individuals studied. Fourth, they must be validated in an independent cohort of patients with the same disease phenotype, preferably by a different group of investigators. Finally, the impact of the genetic variant on the protein product must possess biologic plausibility as impacting the development or the outcome of the disease of study. Only after all of these criteria are met should clinicians be comfortable moving to the arena of tailoring therapy based on genetic variations.
Review Questions
-
1.
Which part of the genetic composition of a cell contains the actual coding sequence for the production of proteins?
-
A.
Alleles
-
B.
Codons
-
C.
Exons
-
D.
Introns
-
E.
Promoter regions
-
A.
-
2.
Which of the following cells lack a nucleus and deoxyribonucleic acid (DNA)?
-
A.
Astrocytes
-
B.
Cardiomyocytes
-
C.
Erythrocytes
-
D.
Neutrophils
-
E.
Type II pneumocytes
-
A.
-
3.
Which of the following statements regarding genetic mutations is most accurate?
-
A.
Germ-line mutations which occur in reproductive cells are the only mutations of clinical consequence.
-
B.
Mutations in the intron/exon boundary region are of no clinical significance because they are excised during the process of splicing.
-
C.
Mutations in the noncoding regulatory regions may alter the quantity of mRNA transcribed, but do not affect the expression of the gene.
-
D.
Mutations that occur in the coding regions of the gene may have several consequences including no effect at all on the end product protein.
-
E.
Translocations are large scale mutations that entail switching of chromosomal regions between different loci on the same chromosome.
-
A.
-
4.
You are caring for two brothers with acute lung injury secondary to smoke inhalation from an apartment fire. These two infants were apparently sleeping in the same crib when they were rescued simultaneously by fire fighters. The first infant was extubated within 48 h of intubation and is doing well with a minimal oxygen requirement. The second has experienced a much more severe lung insult and remains intubated on high frequency oscillatory ventilation. In attempting to understand the difference in their clinical response to the seemingly identical insult, you suspect that it may be related to a polymorphism in one of the genes that codes for surfactant protein B. In considering this possibility, which of the following is true?
-
A.
Although plausible, it is unlikely to be associated with a polymorphism because polymorphisms are rare occurring in less than one percent of the population.
-
B.
It is not plausible because variances in the translation of such a complex protein require differences in an entire haplotype, and not simply a single nucleotide polymorphism.
-
C.
It is plausible because genetic polymorphisms may influence the quantity of mRNA transcribed and/or the functional activity of the surfactant protein B.
-
D.
It is unlikely as there are no reports of associations between surfactant protein gene polymorphisms and outcomes from pulmonary disease.
-
E.
It is unlikely because dysfunctional surfactant protein B demonstrates an X-linked pattern of inheritance.
-
A.
-
5.
The term used to describe a difference of only one nucleotide in the DNA sequence of a gene that may influence the susceptibility to and the outcome from diseases associated with critical illness?
-
A.
Allele
-
B.
Codon
-
C.
Exon
-
D.
Linkage disequilibrium
-
E.
Single nucleotide polymorphism
-
A.
Answers
-
1.
C
-
2.
C
-
3.
D
-
4.
C
-
5.
E
Suggested Readings
Adamzik M, Frey U, Sixt S, et al. ACE I/D but not AGT (−6)A/G polymorphism is a risk factor for mortality in ARDS. Eur Respir J. 2007;29:482–8.
Binder A, Endler G, Muller M, et al. 4G4G genotype of the plasminogen activator inhibitor-1 promoter polymorphism associates with disseminated intravascular coagulation in children with systemic meningococcemia. J Thromb Haemost. 2007;5:2049–54.
Cornell TT, Wynn J, Shanley TP, et al. Mechanisms and regulation of the gene-expression response to sepsis. Pediatrics. 2010;125: 1248–58.
Fang XM, Schroder S, Hoeft A, Stuber F. Comparison of two polymorphisms of the interleukin-1 gene family: interleukin-1 receptor antagonist polymorphism contributes to susceptibility to severe sepsis. Crit Care Med. 1999;27:1330–4.
Gao L, Barnes KC. Recent advances in genetic predisposition to clinical acute lung injury. Am J Physiol Lung Cell Mol Physiol. 2009;296:L713–25.
Gao L, Grant A, Halder I, et al. Novel polymorphisms in the myosin light chain kinase gene confer risk for acute lung injury. Am J Respir Cell Mol Biol. 2006;34:487–95.
Gao L, Flores C, Fan-Ma S, et al. Macrophage migration inhibitory factor in acute lung injury: expression, biomarker, and associations. Transl Res. 2007;150:18–29.
Gong MN, Zhou W, Williams PL, et al. Polymorphisms in the mannose binding lectin-2 gene and acute respiratory distress syndrome. Crit Care Med. 2007;35:48–56.
Harding D, Baines PB, Brull D, et al. Severity of meningococcal disease in children and the angiotensin-converting enzyme insertion/deletion polymorphism. Am J Respir Crit Care Med. 2002;165: 1103–6.
Lin Z, Pearson C, Chinchilli V, et al. Polymorphisms of human SP-A, SP-B, and SP-D genes: association of SP-B Thr131Ile with ARDS. Clin Genet. 2000;58:181–91.
Lin Z, Thomas NJ, Wang Y, et al. Deletions within a CA-repeat-rich region of intron 4 of the human SP-B gene affect mRNA splicing. Biochem J. 2005;389:403–12.
Mandelberg A, Tal G, Naugolny L, et al. Lipopolysaccharide hyporesponsiveness as a risk factor for intensive care unit hospitalization in infants with respiratory syncitial virus bronchiolitis. Clin Exp Immunol. 2006;144:48–52.
Manocha S, Russell JA, Sutherland AM, et al. Fibrinogen-beta gene haplotype is associated with mortality in sepsis. J Infect. 2007;54:572–7.
Menges T, Konig IR, Hossain H, et al. Sepsis syndrome and death in trauma patients are associated with variation in the gene encoding for tumor necrosis factor. Crit Care Med. 2008;36:1456–62.
Mira JP, Cariou A, Grall F, et al. Association of TNF2, a TNF-alpha promoter polymorphism, with septic shock susceptibility and mortality: a multicenter study. JAMA. 1999;282:561–8.
Nadel S, Newport MJ, Booy R, Levin M. Variation in the tumor necrosis factor-alpha gene promoter region may be associated with death from meningococcal disease. J Infect Dis. 1996;174: 878–80.
Quasney MW, Waterer GW, Dahmer MK, et al. Association between surfactant protein B + 1580 polymorphism and the risk of respiratory failure in adults with community-acquired pneumonia. Crit Care Med. 2004;32:1115–9.
Shanley TP, Cvijanovich N, Lin R, et al. Genome-level longitudinal expression of signaling pathways and gene networks in pediatric septic shock. Mol Med. 2007;13(9-10):495–508.
Simon BA, Easley RB, Grigoryev DN, et al. Microarray analysis of regional cellular responses to local mechanical stress in acute lung injury. Am J Physiol Lung Cell Mol Physiol. 2006;291:L851–61.
Sorensen TI, Nielsen GG, Andersen PK, Teasdale TW. Genetic and environmental influences on premature death in adult adoptees. N Engl J Med. 1988;318:727–32.
The National Human Genome Research Institute’s Talking Glossary of Genetic Terms. http://www.genome.gov/glossary.cfm#s.
Toubiana J, Courtine E, Pene F, et al. IRAK1 functional genetic variant affects severity of septic shock. Crit Care Med. 2010;38: 2287–94.
Wong HR, Shanley TP, Sakthivel B, et al. Genome-level expression profiles in pediatric septic shock indicate a role for altered zinc homeostasis in poor outcome. Physiol Genomics. 2007;30: 146–55.
Ye SQ, Simon BA, Maloney JP, et al. Pre-B-cell colony-enhancing factor as a potential novel biomarker in acute lung injury. Am J Respir Crit Care Med. 2005;171:361–70.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer-Verlag London Limited
About this chapter
Cite this chapter
Thomas, N.J., Dahmer, M.K., Quasney, M.W. (2012). Genetic Predisposition to Critical Illness in the Pediatric Intensive Care Unit. In: Lucking, S., Maffei, F., Tamburro, R., Thomas, N. (eds) Pediatric Critical Care Study Guide. Springer, London. https://doi.org/10.1007/978-0-85729-923-9_11
Download citation
DOI: https://doi.org/10.1007/978-0-85729-923-9_11
Published:
Publisher Name: Springer, London
Print ISBN: 978-0-85729-922-2
Online ISBN: 978-0-85729-923-9
eBook Packages: MedicineMedicine (R0)