
Abstract
Background
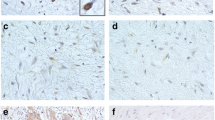
CTNNB1 gene mutations are the molecular key events in the majority of sporadic desmoid-type fibromatosis (DF). The specific S45F mutation has been reported to be associated with a more aggressive clinical course in DF. For the current study, the CTNNB1 mutation status was analyzed in DF samples from the prospective German Interdisciplinary Sarcoma Group (GISG) phase 2 study evaluating imatinib to induce progression arrest in DF Response Evaluation Criteria In Solid Tumors (RECIST) progressive patients.
Methods
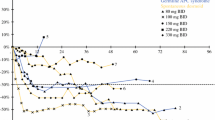
Thirty-seven patients were treated with a planned dose of imatinib 800 mg daily over 2 years (NCT01137916). The progression arrest rate (PAR) after 6 months of treatment was the primary endpoint of the study. CTNNB1 exon 3 mutation status was analyzed using Sanger sequencing.
Results
Thirty-three (97 %) of 34 patients reaching the primary endpoint were evaluable for CTNNB1 mutation exon 3 status. T41A mutations accounted for 30.3 % of the study samples and S45 mutations for 48.5 %, whereas CTNNB1 wild-type status was found in 21.2 %. The respective PAR at 6 months was 70, 81, and 43 %. Patients harboring CTNNB1 mutations demonstrated a higher PAR compared to wild-type DF. There was a statistically significant difference comparing patients with S45F mutations (85 % PAR) versus wild-type status (p = 0.05).
Conclusions
Mutations at position S45 were overrepresented in the GISG-01 trial recruiting RECIST progressive patients only. The positive correlation of CTNNB1 mutation status with the progression arrest rate after imatinib therapy supports the idea of a potential predictive impact of the mutation status on DF treatment decision making.


Similar content being viewed by others

References
Kasper B, Stroebel P, Hohenberger P. Desmoid tumors—clinical features and treatment options for advanced disease. Oncologist. 2011;16:682–93.
Goldblum JR, Fletcher JA. Desmoid-type fibromatosis. In: Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F, editors. World Health Organisation classification of tumours of soft tissue and bone. 4th ed. Lyon: IARC Press; 2013. p. 72–3.
Van Broekhoven DL, Grünhagen DJ, den Bakker MA, van Dalen T, Verhoef C. Time trends in the incidence and treatment of extra-abdominal and abdominal aggressive fibromatosis: a population-based study. Ann Surg Oncol. 2015;22:2817–23.
Kasper B, Baumgarten C, Bonvalot S, et al; Desmoid Working Group. Management of sporadic desmoid-type fibromatosis: a European consensus approach based on patients’ and professionals’ expertise—a Sarcoma Patients EuroNet (SPAEN) and European Organisation for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG) initiative. Eur J Cancer. 2015;51:127–36.
Janinis J, Patriki M, Vini L, Aravantinos G, Whelan JS. The pharmacological treatment of aggressive fibromatosis: a systematic review. Ann Oncol. 2003;14:181–90.
Heinrich MC, McArthur GA, Demetri GD, et al. Clinical and molecular studies of the effect of imatinib on advanced aggressive fibromatosis (desmoid tumour). J Clin Oncol. 2006;24:1195–203.
Penel N, Le Cesne A, Bui B et al. Imatinib for progressive and recurrent aggressive fibromatosis (desmoid tumors): an FNCLCC/French Sarcoma Group phase II trial with a long-term follow-up. Ann Oncol. 2011;22:452–7.
Miyaki M, Yamaguchi T, Iijima T, et al. Difference in characteristics of APC mutations between colonic and extracolonic tumors of FAP patients: variations with phenotype. Int J Cancer. 2008;122:2491–7.
Huss S, Nehles J, Binot E, et al. Beta-catenin (CTNNB1) mutations and clinicopathological features of mesenteric desmoid-type fibromatosis. Histopathology. 2013;62:294–304.
Lazar AJ, Tuvin D, Hajibashi S, et al. Specific mutations in the beta-catenin gene (CTNNB1) correlate with local recurrence in sporadic desmoid tumors. Am J Pathol. 2008;173:1518–27.
Colombo C, Miceli R, Lazar AJ, et al. CTNNB1 45F mutation is a molecular prognosticator of increased postoperative primary desmoid tumor recurrence: an independent, multicenter validation study. Cancer. 2013;119:3696–702.
Van Broekhoven DL, Verhoef C, Grünhagen DJ, et al. Prognostic value of CTNNB1 gene mutation in primary sporadic aggressive fibromatosis. Ann Surg Oncol. 2015;22:1464–70.
Domont J, Salas S, Lacroix L, et al. High frequency of beta-catenin heterozygous mutations in extra-abdominal fibromatosis: a potential molecular tool for disease management. Br J Cancer. 2010;102:1032–6.
Mullen JT, Delaney TF, Rosenberg AE, et al. Beta-catenin mutation status and outcomes in sporadic desmoid tumors. Oncologist. 2013;18:1043–9.
Therasse P, Arbruck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000;92:205–21.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–81.
Kasper B, Grünwald V, Reichardt P, et al. Phase II study evaluating imatinib to induce progression arrest in RECIST progressive desmoid tumors not amenable to surgical resection with R0 intent or accompanied by unacceptable function loss—a study of the German Interdisciplinary Sarcoma Group (GISG). Ann Oncol. 2014;25(suppl 4):iv494.
Chugh R, Wathen JK, Patel SR, et al; Sarcoma Alliance for Research through Collaboration (SARC). Efficacy of imatinib in aggressive fibromatosis: results of a phase II multicenter Sarcoma Alliance for Research through Collaboration (SARC) trial. Clin Cancer Res. 2010;16:4884–91.
Crago AM, Chmielecki J, Rosenberg M, et al. Near universal detection of alterations in CTNNB1 and Wnt pathway regulators in desmoid-type fibromatosis by whole-exome sequencing and genomic analysis. Genes Chromosomes Cancer. 2015;54:606–15.
Hamada S, Futamura N, Ikuta K, et al. CTNNB1 S45F mutation predicts poor efficacy of meloxicam treatment for desmoid tumors: a pilot study. PLoS One. 2014;9:e96391.
Colombo C, Bolshakov S, Hajibashi S, et al. “Difficult to diagnose” desmoid tumours: a potential role for CTNNB1 mutational analysis. Histopathology. 2011;59:336–40.
Le Guellec S, Soubeyran I, Rochaix P, et al. CTNNB1 mutation analysis is a useful tool for the diagnosis of desmoid tumors: a study of 260 desmoid tumors and 191 potential morphologic mimics. Mol Pathol. 2012;25:1551–8.
Gounder MM, Lefkowitz RA, Keohan ML, et al. Activity of sorafenib against desmoid tumor/deep fibromatosis. Clin Cancer Res. 2011;17:4082–90.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kasper, B., Gruenwald, V., Reichardt, P. et al. Correlation of CTNNB1 Mutation Status with Progression Arrest Rate in RECIST Progressive Desmoid-Type Fibromatosis Treated with Imatinib: Translational Research Results from a Phase 2 Study of the German Interdisciplinary Sarcoma Group (GISG-01). Ann Surg Oncol 23, 1924–1927 (2016). https://doi.org/10.1245/s10434-016-5132-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5132-4