
Abstract
Introduction
Excisional biopsy is currently recommended for atypical ductal hyperplasia (ADH) diagnosed on core needle breast biopsy (CNB), due to risk of upstaging to invasive or in situ carcinoma (DCIS). The study goal was to identify patients who may potentially forego excisional biopsy if the risk of upstaging is low.
Methods
We conducted a retrospective review of patients diagnosed with ADH on CNB who underwent excisional biopsy at one institution (5/2000–5/2011). We evaluated the upstaging rate and clinicopathologic factors associated with increased upstaging risk.
Results
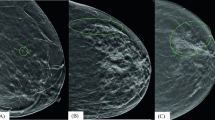
A total of 114 cases of ADH were diagnosed on CNB. The median patient age was 64 years. On mammography, a mass/density/area of distortion was present in 23 % of cases; calcifications were present in 77 %. Most biopsies (79 %) were performed stereotactically. Twenty lesions (18 %) were upstaged to infiltrating carcinoma (5 %) or DCIS (13 %). Residual ADH was present in 43 biopsies (38 %). On univariate analysis, significant variables associated with upstaging included age >50 years, a mass lesion on mammography, and shorter length of biopsy core (p < 0.05). No patient ≤50 years of age was upstaged. Three patients who were not upstaged (3 %) developed ipsilateral disease (2 DCIS and 1 infiltrating ductal carcinoma) at a median time of 37 months.
Conclusions
The rate of upstaging when ADH is diagnosed on CNB at our institution is 18 %, and routine excisional biopsy is currently recommended for all patients. However, patients <50 years old with focal atypia only and no residual calcifications postbiopsy may represent a low-risk group who could potentially avoid excisional biopsy.

Similar content being viewed by others


References
Nguyen CV, Albarracin CT, Whitman GJ, Lopez A, Sneige N. Atypical ductal hyperplasia in directional vacuum-assisted biopsy of breast microcalcifications: considerations for surgical excision. Ann Surg Oncol. 2011;18(3):752–61.
Winchester DJ, Bernstein JR, Jeske JM, et al. Upstaging of atypical ductal hyperplasia after vacuum-assisted 11-gauge stereotactic core needle biopsy. Arch Surg. 2003;138(6):619–22.
Polat AK, Kanbour-Shakir A, Andacoglu O, Polat AV, Johnson R, Bonaventura M, Soran A. Atypical hyperplasia on core biopsy: is further surgery needed? Am J Med Sci. 2012;344(1):28–31.
Jain RK, Mehta R, Dimitrov R, et al. Atypical ductal hyperplasia: interobserver and intraobserver variability. Mod Pathol. 2011;24(7):917–23.
Darvishian F, Singh B, Simsir A, Ye W, Cangiarella JF. Atypia on breast core needle biopsies: reproducibility and significance. Ann Clin Lab Sci. 2009;39(3):270–6.
Kohr JR, Eby PR, Allison KH, DeMartini WB, Gutierrez RL, Peacock S, Lehman CD. Risk of upgrade of atypical ductal hyperplasia after stereotactic breast biopsy: effects of number of foci and complete removal of calcifications. Radiology. 2010;255(3):723–30.
Ingegnoli A, d’Aloia C, Frattaruolo A, Pallavera L, Martella E, Crisi G, Zompatori M. Flat epithelial atypia and atypical ductal hyperplasia: carcinoma underestimation rate. Breast J. 2010;16(1):55–9.
Ely KA, Carter BA, Jensen RA, Simpson JF, Page DL. Core biopsy of the breast with atypical ductal hyperplasia: a probabilistic approach to reporting. Am J Surg Pathol. 2001;25(8):1017–21.
Bendifallah S, Defert S, Chabbert-Buffet N, et al. Scoring to predict the possibility of upgrades to malignancy in atypical ductal hyperplasia diagnosed by an 11-gauge vacuum-assisted biopsy device: an external validation study. Eur J Cancer. 2012;48(1):30–6.
Page DL, Dupont WD, Rogers LW, Rados MS. Atypical hyperplastic lesions of the female breast. A long-term follow-up study. Cancer. 1985;55(11):2698–708.
Page DL, Rogers LW. Combined histologic and cytologic criteria for the diagnosis of mammary atypical ductal hyperplasia. Hum Pathol. 1992;23(10):1095–7.
Eby PR, Ochsner JE, DeMartini WB, Allison KH, Peacock S, Lehman CD. Is surgical excision necessary for focal atypical ductal hyperplasia found at stereotactic vacuum-assisted breast biopsy? Ann Surg Oncol. 2008;15(11):3232–8.
Chae BJ, Lee A, Song BJ, Jung SS. Predictive factors for breast cancer in patients diagnosed atypical ductal hyperplasia at core needle biopsy. World J Surg Oncol. 2009;7:77.
Deshaies I, Provencher L, Jacob S, et al. Factors associated with upgrading to malignancy at surgery of atypical ductal hyperplasia diagnosed on core biopsy. Breast. 2011;20(1):50–5.
Londero V, Zuiani C, Linda A, Battigelli L, Brondani G, Bazzocchi M. Borderline breast lesions: comparison of malignancy underestimation rates with 14-gauge core needle biopsy versus 11-gauge vacuum-assisted device. Eur Radiol. 2011;21(6):1200–6.
Arora S, Moezzi M, Kim U, Menes TS. Is surgical excision necessary for atypical ductal hyperplasia diagnosed with 8-gauge stereotactic biopsy? Breast J. 2009;15(6):673–4.
Forgeard C, Benchaib M, Guerin N, et al. Is surgical biopsy mandatory in case of atypical ductal hyperplasia on 11-gauge core needle biopsy? A retrospective study of 300 patients. Am J Surg. 2008;196(3):339–45.
Villa A, Tagliafico A, Chiesa F, Chiaramondia M, Friedman D, Calabrese M. Atypical ductal hyperplasia diagnosed at 11-gauge vacuum-assisted breast biopsy performed on suspicious clustered microcalcifications: could patients without residual microcalcifications be managed conservatively? AJR Am J Roentgenol. 2011;197(4):1012–8.
Sneige N, Lim SC, Whitman GJ, Krishnamurthy S, Sahin AA, Smith TL, Stelling CB. Atypical ductal hyperplasia diagnosis by directional vacuum-assisted stereotactic biopsy of breast microcalcifications. Considerations for surgical excision. Am J Clin Pathol. 2003;119(2):248–53.
Wagoner MJ, Laronga C, Acs G. Extent and histologic pattern of atypical ductal hyperplasia present on core needle biopsy specimens of the breast can predict ductal carcinoma in situ in subsequent excision. Am J Clin Pathol. 2009;131(1):112–21.
Allison KH, Eby PR, Kohr J, DeMartini WB, Lehman CD. Atypical ductal hyperplasia on vacuum-assisted breast biopsy: suspicion for ductal carcinoma in situ can stratify patients at high risk for upgrade. Hum Pathol. 2011;42(1):41–50.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McGhan, L.J., Pockaj, B.A., Wasif, N. et al. Atypical Ductal Hyperplasia on Core Biopsy: An Automatic Trigger for Excisional Biopsy?. Ann Surg Oncol 19, 3264–3269 (2012). https://doi.org/10.1245/s10434-012-2575-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2575-0