
Abstract
Background
Retrospective studies have shown that occult nipple–areolar complex (NAC) involvement in breast cancer is low, occurring in 6–10% of women undergoing skin-sparing mastectomy (SSM). The cosmetic result and high patient satisfaction of nipple-sparing mastectomy (NSM) has prompted further evaluation of the oncologic safety of this procedure.
Methods
We conducted a retrospective chart review of 36 self-selected patients who underwent 51 NSM procedures between 2002 and 2007. Criterion for patient selection was no clinical evidence of nipple–areolar tumor involvement. All patients had the base of the NAC evaluated for occult tumor by permanent histologic section assessment. We also evaluated tumor size, location, axillary node status, recurrence rate, and cosmetic result.
Results
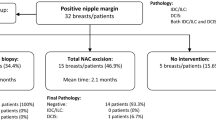
Malignant NAC involvement was found in 2 of 34 NSM (5.9%) completed for cancer which prompted subsequent removal of the NAC. Of the 51 NSM, 17 were for prophylaxis, 10 for ductal carcinoma in situ (DCIS), and 24 for invasive cancer. The average tumor size was 2.8 cm for invasive cancer and 2.5 cm for DCIS. Nine patients had positive axillary nodes. Overall, 94% of the tumors were located peripherally in the breast. After mean follow-up of 18 months, only two patients (5.9%) had local recurrence.
Conclusion
Using careful patient selection and careful pathological evaluation of the subareolar breast tissue at surgery, NSM can be an oncologically safe procedure in patients where this is important to their quality of life. A prospective study based on focused selection criteria and long-term follow-up is currently in progress.
Similar content being viewed by others


References
Rowland JH, Desmond KA, et al. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J Natl Cancer Inst 2000; 17:1422–9
Pelusi J. Sexuality and body image. AJN 2006; 106:32–8
Wilmoth MC. The after math of breast cancer: an altered sexual self. Cancer Nurs 2001; 24:278–86
Cocquyt VF, Blondeel PN, Depypere HT, et al. Better cosmetic results and comparable quality of life after skin-sparing mastectomy and immediate autologous breast reconstruction compared to breast conservative treatment. Br J Plast Surg 2003; 56:462–70
Jabor MA, Shayani P, et al. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg 2002; 110:457–63
Newman LA, Kuerer HM, Hunt KK, et al. Presentation, treatment, and outcome of local recurrence after skin-sparing mastectomy and immediate breast reconstruction. Ann Surg Oncol 1998; 5:620–6
Simmons RM, Fish SK, Gayle L, et al. Local and distant recurrence rates in skin-sparing mastectomies compared with non-skin-sparing mastectomies. Ann Surg Oncol 1999:6:676–81
Carlson GW, Styblo TM, et al. Local recurrence after skin-sparing mastectomy: tumor biology or surgical conservatism? Ann Surg Oncol 2003; 10:108–12
Ho CM, Mak CKL, Lau Y, et al. Skin involvement in invasive breast carcinoma: safety of skin-sparing mastectomy. Ann Surg Oncol 2003;10:102–7
Cunnick GH, Mokbel K. Skin-sparing mastectomy, review. Am J Surg 2004;188:78–84
Laronga C, Kemp B, et al. The incidence of occult nipple-areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol 1999;6:609–13
Fisher B, Bauer M, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med 1985;312:665–73
Fisher B, Anderson S, et al. Twenty year follow-up of a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 2002;347:1233–41
Gerber B, Krause A, et al. Skin-sparing mastectomy with conservation of the nippl-areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg 2003;238:120–7
Crowe JP, Kim JA, et al. Nipple-sparing mastectomy, technique and results of 54 procedures. Arch Surg 2004;139:148–50
Petit JY, Veronesi U, et al. When mastectomy becomes inevitable: the nipple-sparing approach. Breast 2005;14:527–31
Caruso F, Ferrara M, et al. Nipple-sparing mastectomy: sixty-six months follow-up. EJSO 2006;32:937–40
Benediktsson KP, Perbeck L. Survival in breast cancer after nipple-sparing subcutaneous mastectomy and immediate reconstruction with implants: a prospective trial with 13 years median follow-up in 216 patients. EJSO 2008;34(2):143–8
Kennedy MJ, Abeloff MD. Management of locally recurrent breast cancer. Cancer 1993;71:2395–409
Stolier AJ, Wang J. Terminal duct lobular units are scarce in the nipple: Implications for prophylactic nipple-sparing mastectomy. Ann Surg Oncol 2008;15(2):438–42
Fisher E, Gregorio RM, Fisher B, et al. The pathology of invasive breast cancer. Cancer 1975;36:1–85
Rusby JE, Brachtel EF, Taghian A, et al. Microscopic anatomy within the nipple: implications for nipple-sparing mastectomy. Am J Surg 2007;194(4):433–7
Lambert PA, Kolm P, Perry RR. Parameters that predict nipple involvement in breast cancer. J Am Coll Surg 2000;191:354–9
Andersen JA, Pallesen RM. Spread to the nipple and areola in carcinoma of the breast. Ann Surg 1979;189(3):367–72
Lagios MD, Gates EA, et al. A guide to the frequency of nipple involvement in breast cancer. Am J Surg 1979;138:135–42
Santini D, Taffurelli M, et al. Neoplastic involvement of nipple-areolar complex in invasive breast cancer. Am J Surg 1989;158:399–403
Vlajcic Z, Zic R, Stanec S, et al. Nipple–areola complex preservation, predictive factors of neoplastic nipple-areola complex invasion. Ann Plast Surg 2005;55:240–4
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Voltura, A.M., Tsangaris, T.N., Rosson, G.D. et al. Nipple-Sparing Mastectomy: Critical Assessment of 51 Procedures and Implications for Selection Criteria. Ann Surg Oncol 15, 3396–3401 (2008). https://doi.org/10.1245/s10434-008-0102-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-008-0102-0