
Abstract
Background
FESS is a common minimally invasive surgery that requires a clear field to be performed well. Hypotensive anesthesia is one of the most common maneuvers performed to help in keeping the field clear. An ideal drug for hypotensive anesthesia should be cheap and familiar to the anesthesiologist. So, being familiar with propofol and by using its cardio-depressant action, the idea of the research was developed. The idea of the study was to compare propofol infusion versus nitroglycerine infusion as a hypotensive agent.
Results
The mean duration of surgery was longer in the NTG to the propofol group. There was a high statistical significance in the average blood loss in the propofol group compared to the NTG group. The visibility of the operative field also was significant in the propofol group as compared with the NTG group. The mean heart rate in the NTG group was higher than the mean heart rate in the propofol group. The MAP in both groups was within a close range.
Conclusion
Propofol and NTG can produce a safe and effective controlled hypotension during FESS. Whereas, propofol has better surgical field visibility, less surgical bleeding, and less tachycardia during FESS.
Similar content being viewed by others

Background
FESS (functional endoscopic sinus surgery) is a popular minimally invasive surgical technique for the management of a patient with sinus pathological conditions (El-Shmaa et al. 2017; Shaban et al. 2019; Jacobi et al. 2000). The aim of this sinus endoscopic surgery is to restore a normal mucociliary clearing function and drainage of sinuses (El-Shmaa et al. 2017; Shaban et al. 2019; Jacobi et al. 2000). Although it is a minimally invasive surgery, it can lead to serious complications such as optic nerve injury, orbital cellulitis, meningitis, and rhino-oral fistulas (Ankichetty et al. 2011). Bleeding is one of the obstacles that is associated with this technique that can decrease the surgical field visualization and increase the probability of complications (El-Shmaa et al. 2017; Jacobi et al. 2000; Ankichetty et al. 2011).
One of the most important maneuvers used to minimize this bleeding is hypotensive anesthesia (Shaban et al. 2019; Jacobi et al. 2000; Ankichetty et al. 2011). The ideal hypotensive agent for anesthetist must be a familiar drug, easy to use, rapid onset and offset, and with minimal side effects (Shaban et al. 2019; Jacobi et al. 2000). Nitroglycerin infusion is a frequently used drug to produce controlled hypotension, as it is cheap and easy to use drug rapid onset and offset time. But it has common side effects which are reflex tachycardia and venous congestion which may also obscures the surgical field and decreases surgeon satisfaction (El-Shmaa et al. 2017; Shaban et al. 2019; Srivastava et al. 2013).
Propofol is one of the most common intravenous anesthetic agents, used both for induction and as a part of total intravenous anesthesia (TIVA) (Ankichetty et al. 2011; Tirelli et al. 2004). It has a rapid onset and offset and one of its side effects is hypotension. Recently total intravenous anesthesia (TIVA) using propofol and remifentanil is a common procedure used in western countries (Tirelli et al. 2004; Mandal 2003) to produce hypotensive anesthesia. In Egypt, remifentanil is not freely available.
The objective of the study is to assess the use of propofol infusion in comparison to nitroglycerine infusion as a hypotensive agent on the surgical field visibility.
Methods
This is a prospective, comparative, randomized, single-blind study; between propofol and nitroglycerin infusion as regards their hypotensive effect; on 40 patients undergoing FESS under general anesthesia. This study was approved by the Research Ethics committee at Faculty of Medicine, Ain Shams University Hospital, Cairo, Egypt (FMASU R 60/2019). Clinical trial registration was done with the ID (NCT04220281). All patients gave written informed consent. The sample size was calculated as 20 in each group based on previous studies.
Forty patients admitted to Ain Shams University Hospital in Egypt, scheduled for FESS procedure. Patients were ASA I and II diagnosed with chronic sinusitis. Age range was determined between 18 and 60 years, undergoing elective FESS without septoplasty under general anesthesia. The patient enrollment started from the 1st of December till the 12th of February.
Exclusion criteria included any patient with bleeding disorder, on anticoagulant therapy, renal, hepatic, or cardiac dysfunction, history of cerebrovascular stroke, peripheral vascular diseases, allergic to any of the study drugs, hypertension, morbid obesity, and recurrent endoscopic sinus surgeries.
The primary outcomes of this study were to compare the visibility of the operative field between the study groups. The secondary outcomes recorded were mean blood pressure and pulse rate every 5 min, duration of surgery, amount of blood loss intraoperative, and the emergence time.
Patients were randomly allocated into two groups according to the drug used (propofol group, n = 20; nitroglycerin group, n = 20). Randomization was done by a computer-generated, random number list. The patients, the ENT surgeon (same surgeon in all surgeries), and the anesthetist collecting data all were blinded to the groups. The anesthetist performing the general anesthesia was aware of the patient’s group to be able to deal with any complications and he was not one of the study participants.
All patients were kept fasting as per the standard protocol and were premedicated with midazolam 0.05 mg kg−1 IV in the holding area prior to the induction of anesthesia. All patients were continuously monitored for heart rate (5-lead electrocardiogram), blood pressure (noninvasive automated blood pressure measurement every 2.5 min), oxygen saturation (pulse oximetry), capnography, and bispectral index (BIS) to assess the depth of anesthesia (whenever available) aimed to keep it between 40 and 60.
Vascular access, via peripheral vein cannula (18G) was secured. And all patients received isotonic crystalloid (5 ml/kg) as a loading before anesthesia to compensate for the anticipated hypotension. Preoxygenation for 3 min, then induction of general anesthesia, with fentanyl (1.5 μg kg−1), propofol (1.5 mg kg−1) then atracurium (0.5 mg kg−1) IV. Orotracheal intubation and ventilation were performed. A saline-soaked throat pack was used. All patients were kept in head-up position to 30° and all had gauze soaked with xylocaine adrenalin solution inserted in their nostrils for 5 min before starting the surgery to reduce the amount of blood loss. Anesthesia was maintained with 50% oxygen in air and isoflurane by 1 Mac, and fentanyl 50 μg every 60 min and atracurium 0.1 mg kg−1 every 20–30 min.
In the NTG group, patients received an intravenous infusion of NTG (Nitronal; Sunny pharmaceutical, G.Pol-Boskamp GmbH&Co. KG-Germany) started at a rate of 0.5 μg kg−1 min−1 and increased gradually not to exceed 5 μg kg−1 min−1 guided by MAP. In the Prop group, an intravenous infusion of propofol (Xi’an Libang Shaanxi, China), at a rate of 1–2 mg kg−1 h−1 10 min to be titrated up to 4 mg kg−1 h−1 according to its hypotensive response to achieve a mean arterial pressure that is 20–30% less than the baseline mean arterial pressure or reaching a MAP not less than 60 mmHg without changing the isoflorane given concentration.
A pulse rate of less than 50/min was treated by atropine 0.5 mg IV once and can be repeated if no response within 1–2 min. A pulse rate of more than 100/min was treated by propranolol 1 mg slowly IV; if no response within 5 min, another 1 mg IV can be given up to 3 mg. MAP less than 60 mmHg was treated by decreasing the rate of the studied infusions by 50% and increasing an IV fluid infusion rate. If no response within 5 min, the studied infusions were stopped. If the MAP still low after another 5 min, ephedrine 5 mg IV was administered and the patient would be excluded. If hypotensive anesthesia could not be achieved by the studied drugs, the patient was excluded from the study and managed according to the guidelines.
Near the end of the surgery and before the application of the nasal packs, the studied infusions were stopped, at the end of the surgery the isoflurane was stopped, then reversal of the muscle relaxant, removal of the oral pack, and extubation were done, the patients were transferred to the recovery unit. Upon arrival to PACU, pulse oximetry and noninvasive blood pressure (NIBP) monitors were attached to the patient for continuous monitoring till discharge. Any hypotension was dealt with according to the guidelines. Discharge criteria from PACU were stable vital signs, pain score less than or equal to 2, no nausea or vomiting, calm and alert patient.
To assess the amount of blood loss during surgery, the anesthetist giving anesthesia recorded the amount of blood loss in each surgery. For evaluation of the visibility of the operative field during surgery, the average category scale proposed by Fromm et al. (1986) and Boezaart et al. (1995) was used. The operative field conditions were assessed by the same operating surgeon as:
-
Grade 0: No bleeding.
-
Grade 1: Slight bleeding—No suctioning of blood required.
-
Grade 2: Slight bleeding—Occasional suctioning required. The surgical field is not threatened.
-
Grade 3: Slight bleeding—Frequent suctioning required. Bleeding threatens the surgical field a few seconds after suction is removed.
-
Grade 4: Moderate bleeding—Frequent suctioning required. Bleeding threatens the surgical field directly after suction is removed.
-
Grade 5: Severe bleeding—Constant suctioning required. Bleeding appears faster than can be removed by suction. The surgical field was severely threatened and surgery impossible.
Data recorded
Collection of demographic data, ASA, duration of surgery, visibility of the surgical field, amount of blood loss, and the emergence time (the time from discontinuation of anesthetics till first eye-opening in response to verbal command). Pulse rate and MAP were recorded at baseline and every 5 min
Sample size
Using PASS11 program for sample size calculation and according to Elshama et al. (2017) and Ankichetty et al. (2011), the expected mean amount of intraoperative blood loss in the propofol group = 109 ± 83 ml and in the NTG group = 172.5 ± 28.5 ml, a sample size of 20 patients in each group achieves 80% power to detect this difference with α − error 0.05.
Statistical analysis
Data were analyzed using SPSS 19.0 (IBM, Armonk, NY, USA). Continuous data were summarized in the form of mean and standard deviation (SD) and were analyzed using Student’s T test. The power of significance (P value <0.05) was considered statistically significant.
Results
Forty patients were included in this study, all underwent FESS. They were divided into two groups (NTG group, n = 20 and Prop group, n = 20). The demographic characteristics of both groups were compared as regards age, sex, weight, and ASA status (Table 1), there was no statistically significant difference between both groups (P > 0.05).
Table 2 shows the results of the comparison of studied variables during surgery as regards the duration of surgery, the average blood loss, and the visibility of the surgical field. The mean duration of surgery was longer in the NTG group (98.9 ± 13.6) compared with the propofol group (89.5 ± 8.3) but there was no statistical significance. There was a high statistical significance in the average blood loss in the propofol group compared with NTG group (P value <0.001). The visibility of the operative field also was significant in the propofol group as compared with NTG group (P value = 0.031). The emergence time—was defined as the time from discontinuation of anesthetics till the first eye-opening in response to a verbal command—was slightly longer in the Prop group as compared to NTG group but without statistical significance (P value = 0.334).
Figure 1 showing compared means of heart rate/min between the NTG and Propofol groups recorded every 5 min. It was noticed that the mean heart rate in the NTG group is higher than the mean heart rate in the propofol group.

Mean heart rate (beats min–1) in the two groups at different time intervals
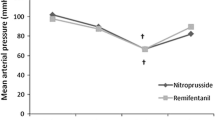
Figure 2 showing compared means of mean arterial blood (MAP) pressure/mmHg between the NTG and propofol groups recorded every 5 min. It was noticed that the MAP in both groups within close range.

(MAP) mean arterial blood pressure (mmHg-1) in the two groups at different time intervals
No significant side effects of hypotensive anesthesia were noticed in all patients. No patient needed the use of atropine or propranolol either during surgery or in the PACU. All patients were closely followed up during the whole procedure and for 30 min postoperatively in the PACU. Any complication that happened, it was dealt with as mentioned in the methodology.
Discussion
One of the main goals of hypotensive anesthesia is to lower the blood pressure to a level that causes minimal bleeding, but at the same time, maintain well perfusion to the vital organs (El-Shmaa et al. 2017; Ankichetty et al. 2011; Srivastava et al. 2013). Decreasing the bleeding in the surgical field improves surgical outcomes and decreases the complications (Srivastava et al. 2013; Tirelli et al. 2004; Baker and Baker 2010).
NTG has been used in many studies and proved efficient as a hypotensive agent to produce hypotensive anesthesia. It is a cheap drug and easy to use and easily available. It produces its action via vasodilatation especially of veins. But one of the adverse effects of NTG that it causes reflex tachycardia. Working in a very small field as in FESS, tachycardia can worsen the surgical field visibility.
Propofol infusion has been used as a deep sedative agent as in endoscopy (Fanti et al. 2004; Hsu et al. 2013) and ICU (Xia et al. 2013). Hypotension was always a reported side effect with the use of propofol (Ankichetty et al. 2011; Claeys et al. 1988; Shafer 1993). So, the idea of this paper is to benefit from this side effect by using propofol as a hypotensive agent.
This study was designed to evaluate the efficacy of propofol infusion in minimal dose as a hypotensive agent as compared to NTG as a routine hypotensive agent during FESS. The main findings in the present study are that propofol and NTG groups both achieved the desired level of hypotension needed for FESS surgery. The MAP was in a similar range in both groups all over the surgery. The mean heart rate measured at different time intervals was lower in the propofol group as compared with the NTG group as seen in Fig. 1. The mean blood loss was significantly lower in the propofol group. It was noticed that the surgical field was significantly better in the propofol group. The emergence time was slightly longer in the Prop group but without statistical significance.
In this study, heart rate decreased after initiation of propofol infusion, this can be explained by its direct inhibitory effects on the cardiovascular system (Claeys et al. 1988; Shafer 1993; Boillot et al. 1999) in it, and by decreasing sympathetic nerve discharge centrally (Krassioukov et al. 1993; Boillot et al. 1999).
The present study is in agreement with the study by Shen. et al. (2015), which compared a combination of etomidate—remifentanil and propofol—remifentanil, MAP and heart rate decreased significantly in the propofol group. This also occurs in the study by Wihelm et al. (2002) which compared the effects of remifentanil versus fentanyl on anesthetic characteristics of propofol and also the propofol group had a lower heart rate.
Hypotensive anesthesia leads to the release of endogenous catecholamines. Propofol has a direct inhibitory effect on the cardiovascular system (Krassioukov et al. 1993; Boillot et al. 1999) and decreases systemic vascular resistance without reflex tachycardia (Claeys et al. 1988; Shafer 1993; Boillot et al. 1999). In contrast, NTG has a direct vasodilator action on vascular smooth muscles without any central effect this leads to hypotension with more oozing at the site of surgery due to reflex tachycardia that occur (Srivastava et al. 2013).
In the present study, the duration of surgery and the amount of bleeding were less in the propofol group. This can be explained by the better surgical field visualization and less time lost in repeated suctioning. This was in agreement with the study by El-Shmaa et al. (2017) in which the group with less tachycardia (using labetalol) has less duration of surgery.
In the present study, the patients already received inhalational anesthesia so we aim to use propofol in a minimal dose of 1–3 mg kg−1 hr−1, adjusted according to the hemodynamic response of the patient. This dose has been used as a sedative dose with local anesthesia (Yoon et al. 2002). The same dose has been used in ICU patients for sedation (Jakob et al. 2012; Memis et al. 2009; Kaneko 2008). All these researches noted hypotension and a decrease in heart rate in their studies which coincide with the present study.
We noticed that the emergence time (Bajwa et al. 2016; Misal et al. 2016) in the propofol group was longer than the nitroglycerin group but without a statistical significant difference. This can be explained by the additional anesthetic effect of propofol with isoflurane used in this case. But as we used a minimal dose of propofol infusion, this did not cause a significant effect.
Recently in European anesthesia, hypotensive anesthesia becoming less popular cause of its side effects (Soghomonyan et al. 2017). Despite that many researchers still using hypotensive anesthesia (Hamed 2018; Prasant et al. 2014; Rokhtabnak et al. 2017; Barak et al. 2015; Kim et al. 2020; Escamilla et al. 2019) but with proper selection of patient as it is proved to be a confident maneuver to decrease blood loss and improve the surgical field visibility. In the present study, using propofol—in FESS—decreases the blood loss and improves the surgical field visibility despite that the MAP was not decreased compared with the NTG group which can avoid the possible side effects that can occur.
Study limitation
One of the main issues—in this study—is that there were no similar researches using different doses of propofol so to perform a better comparison. The number of the enrolled patient was not enough to do more data analysis, to explain more the idea of the study.
Conclusion
Propofol and NTG can produce a safe and effective controlled hypotension during FESS. Whereas, propofol—in a very small infusion rate—has better surgical field visibility, less surgical bleeding, and less tachycardia during FESS.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FESS:
-
Functional endoscopic sinus surgery
- TIVA:
-
Total intravenous anesthesia
- ASA:
-
American Society of Anesthesiology
- ENT surgeon:
-
Ear, nose and throat surgeon
- NTG:
-
Nitroglycerin
- Prop:
-
Propofol
- MAP:
-
Mean arterial pressure
- ICU:
-
Intensive care unit
References
Ankichetty SA, Ponniah M, Cherian VT et al (2011) Comparison of total intravenous anesthesia using propofol and inhalational anesthesia using isoflurane for controlled hypotension in functional endoscopic sinus surgery. J Anaesthesiol Clin Pharmacol 27:328–332. https://doi.org/10.4103/0970-9185.173400
Bajwa SJ, Kaur J, Kulshrestha A, Haldar R, Sethi R, Singh A (2016) Nitroglycerine, esmolol and dexmedetomidine for induced hypotension during functional endoscopic sinus surgery: a comparative evaluation. J Anaesthesiol Clin Pharmacol 32(2):192–197. https://doi.org/10.4097/kjae.2016.69.6.543
Baker AR, Baker AB (2010) Anaesthesia for endoscopic sinus surgery. Acta Anaesthesiol Scand 54:795–803. https://doi.org/10.1111/j.1399-6576.2010.02259.x
Barak M, Yoav L, Abu el-Naaj I (2015) Hypotensive anesthesia versus normotensive anesthesia during major maxillofacial surgery: a review of the literature. ScientificWorldJournal. https://doi.org/10.1155/2015/480728
Boezaart AP, van der Merwe J, Coetzee A (1995) Comparison of sodium nitroprusside- and esmolol-induced controlled hypotension for functional endoscopic sinus surgery. Can J Anaesth 42:373–376. https://doi.org/10.1007/BF03015479
Boillot A, Laurant P, Berthelot A (1999) Effects of propofol on vascular reactivity in isolated aortae from normotensive and spontaneously hypertensive rats. Br J Anaesth 83:622–629. https://doi.org/10.5114/aoms.2018.77256
Claeys MA, Gepts E, Camu F (1988) Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth 60:3–9. https://doi.org/10.1093/bja/60.1.3
El-Shmaa NS, Ezz HA, Younes A (2017) The efficacy of Labetalol versus Nitroglycerin for induction of controlled hypotension during sinus endoscopic surgery. A prospective, double-blind and randomized study. J Clin Anesth 39:154–158. https://doi.org/10.1016/j.jclinane.2017.03.003
Escamilla Y, Cardesín A, Samara L et al (2019) Randomized clinical trial to compare the efficacy to improve the quality of surgical field of hypotensive anesthesia with clonidine or dexmedetomidine during functional endoscopic sinus surgery. Eur Arch Otorhinolaryngol 276:3095–3104. https://doi.org/10.1007/s00405-019-05575-6
Fanti L, Agostoni M, Casati A et al (2004) Target-controlled propofol infusion during monitored anesthesia in patients undergoing ERCP. Gastrointest Endosc 60:361–366. https://doi.org/10.1155/2011/542159
Fromme GA, MacKenzie RA, Gould AB et al (1986) Controlled hypotension for orthognatic surgery. Anesth Analg 65:683–686 PMID: 3706806
Hamed MA (2018) Comparative study between magnesium sulfate and lidocaine for controlled hypotension during functional endoscopic sinus surgery: a randomized controlled study. Anesth Essays Res 12(3):715–718. https://doi.org/10.4103/aer.AER_103_18
Hsu W-H, Wang SS, Shih H-Y et al (2013) Low effect-site concentration of propofol target-controlled infusion reduces the risk of hypotension during endoscopy in a Taiwanese population. J Dig Dis 14:147–152. https://doi.org/10.1111/1751-2980.12020
Jacobi KE, Bohm BE, Richauar AJ et al (2000) Moderate controlled hypotension with sodium nitroprusside does not improve surgical condition or decrease blood loss in endoscopic sinus surgery. J Clin Anesth 12:202–207. https://doi.org/10.1016/S0952-8180(00)00145-8
Jakob SM, Ruokonen E, Grounds RM et al (2012) Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA 307:1151. https://doi.org/10.1001/jama.2012.304
Kaneko T (2008) Postoperative management of carotid endarterectomy with dexmedetomidine comparison with propofol. Masui 57:696 PMID: 18546896
Kim DH, Lee J, Kim SW, Hwang SH (2020) The efficacy of hypotensive agents on intraoperative bleeding and recovery following general anesthesia for nasal surgery: a network meta-analysis. Clin Exp Otorhinolaryngol. https://doi.org/10.21053/ceo.2020.00584 [published online ahead of print, 2020 Aug 28].
Krassioukov AV, Gelb AW, Weaver LC (1993) Action of propofol on central sympathetic mechanisms controlling blood pressure. Can J Anesth 40(8):761–769. https://doi.org/10.1007/BF03009773
Mandal P (2003) Hypotensive anaesthesia with remifentanil for functional endoscopic sinus surgery. J Anaesth Clin Pharmacol 19:411–415
Memis D, Kargi M, Sut N (2009) Effects of propofol and dexmedetomidine on indocyanine green elimination assessed with LIMON to patients with early septic shock: a pilot study. J Crit Care 24:603. https://doi.org/10.1016/j.jcrc.2008.10.005
Misal US, Joshi SA, Shaikh MM (2016) Delayed recovery from anesthesia: a postgraduate educational review. Anesth Essays Res 10(2):164–172. https://doi.org/10.4103/0259-1162.165506
Prasant MC, Kar S, Rastogi S, Hada P, Ali FM, Mudhol A (2014) Comparative study of blood loss, quality of surgical field and duration of surgery in maxillofacial cases with and without hypotensive anesthesia. J Int Oral Health 6(6):18–21
Rokhtabnak F, Djalali Motlagh S, Ghodraty M et al (2017) Controlled hypotension during rhinoplasty: a comparison of dexmedetomidine with magnesium sulfate. Anesth Pain Med 7(6):e64032. https://doi.org/10.5812/aapm.64032
Shaban AAE, Mohammed HF, Zaher AAA (2019) Role of gabapentin in controlled hypotension for nasal surgeries: a randomized controlled study. Sci J Al-Azhar Med Fac Girls 3:172. https://doi.org/10.4103/sjamf.sjamf_74_18
Shafer SL (1993) Advances in propofol pharmacokinetics and pharmacodynamics. J Clin Anesth 5(Suppl. 1):14–21S. https://doi.org/10.1016/0952-8180(93)90003-W
Shen XC, Ao X, Cao Y et al (2015) Etomidate-remifentanil is more suitable for monitored anesthesia care during gastroscopy in older patients than propofol-remifentanil. Med Sci Monit 21:1–8. https://doi.org/10.12659/MSM.891183
Soghomonyan S, Stoicea N, Sandhu GS, Pasternak JJ, Bergese SD (2017) The role of permissive and induced hypotension in current neuroanesthesia practice. Front Surg 4:1. https://doi.org/10.3389/fsurg.2017.00001 Published 2017 Jan 30
Srivastava U, Dupargude AB, Kumar D et al (2013) Controlled hypotension for functional endoscopic sinus surgery: comparison of Esmolol and nitroglycerine. Indian J Otolaryngol Head Neck Surg 65:440–444. https://doi.org/10.1007/s12070-013-0655-5
Tirelli G, Bigarini S, Russolo M (2004) et al.- Total intravenous anaesthesia in endoscopic sinus surgery. Acta Otorhinolaryngol Ital 24:137–144. https://doi.org/10.1002/alr.22173
Wilhelm W, Biedler A, Huppert A et al (2002) Comparison of the effects of remifentanil or fentanyl on anaesthetic induction characteristics of propofol, thiopental or etomidate. Eur J Anaesthesiol 19:350–356. https://doi.org/10.5812/kowsar.22287523.2130
Xia ZQ, Chen SQ, Yao X et al (2013) Clinical benefits of dexmedetomidine versus propofol in adult intensive care unit patients: a meta-analysis of randomized clinical trials. J Surg Res 185:833–843. https://doi.org/10.1016/j.jss.2013.06.062
Yoon HD, Yoon ES, Dhong ES et al (2002) Low-dose propofol infusion for sedation during local anesthesia. Plast Reconstr Surg 109(3):956–963. https://doi.org/10.1097/00006534-200203000-00023
Acknowledgements
We thank our colleagues from the ENT and anesthesia departments who provided help, insight, and expertise that greatly assisted the research, although they may not agree with all of the interpretations/conclusions of this paper.
Funding
None.
Author information
Authors and Affiliations
Contributions
RGA contributed to the conception and design of the study, organized the data collection, reviewed and greatly contributed to the interpretation of results, checked the statistical analysis, and revised the manuscript critically for important intellectual content. TNA performed data collection and organized data preparation. Both authors actively discussed the manuscript, critically reviewed its comprehensive content, and finally approved the version to be submitted for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee at Faculty of Medicine, Ain Shams University Hospital, Cairo, Egypt (FMASU R 60/2019). All patients gave written informed consent. A Clinical Trial registration was done with the ID (NCT04220281) at February 17, 2020.
Consent for publication
Not applicable.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abu-sinna, R.G., Abdelrahman, T.N. Comparison of the hypotensive efficacy of propofol infusion versus nitroglycerin infusion in functional endoscopic sinus surgery. Ain-Shams J Anesthesiol 12, 65 (2020). https://doi.org/10.1186/s42077-020-00109-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42077-020-00109-3