
Abstract
Background
South Asia has one of the largest proportions of undernourished children in the world, especially stunting, wasting, and underweight as well as micronutrient deficiencies such as the deficiency of iron, vitamin A, and zinc. Undernutrition continues to pose a major threat to this region’s economic and social growth. This systematic review aims to assess the drivers and identify priorities for child undernutrition in South Asia. It aims to appraise, synthesise, and summarise literature to create an evidence base that looks at multiple faces of macro and micro child undernutrition in South Asia.
Methods
A systematic review of published and grey literature on child undernutrition, including macro and micronutrient deficiencies, in South Asia covering the period January 2000 to September 2019 will be undertaken. Studies with all relevant study designs and those published in English will be considered for inclusion. Five academic databases will be searched: CINAHL, EMBASE, PubMed, PsycINFO, and Scopus, in addition to various grey literature sources. The analysis will incorporate a narrative synthesis, meta-ethnography or a meta-analysis as appropriate, depending on the nature of the retrieved data. Quality of the included studies will be assessed by validated tools. The UNICEF conceptual framework on child undernutrition will be used to frame findings.
Discussion
This protocol is guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) guidelines. The protocol gives an insight into the scope and parameters for the systematic review to be carried out.
Systematic review registration
The protocol was registered by the PROSPERO international prospective register of systematic reviews, reference CRD42018112696.
Similar content being viewed by others

Background
Child undernutrition continues to be a major public health concern [1] and is considered an underlying cause of around 60% of deaths amongst children under 5 years of age in low- and middle-income countries (LMICs) [2]. Undernutrition encompasses macronutrient (fats, protein, and carbohydrate) and micronutrient (minerals and vitamins) deficiencies. Malnutrition encompasses both undernutrition (stunting, wasting, underweight and deficiencies of essential vitamins and minerals) and overnutrition (obesity or over-consumption of specific nutrients) [3]. Undernutrition has dire consequences for the health of children and the long-term economic productivity of nations [4,5,6]. It is associated with increased morbidity and mortality due to infections, increased risk of maternal, perinatal and neonatal mortality and increased risk of chronic diseases in adults. It is also associated with poor child development leading to poor school performance with long-term economic and social implications [6, 7].
Global estimates of undernutrition amongst children under 5 years of age suggest that in 2017, 151 million children were stunted, 50.5 million children were wasted [8] and 90 million children were underweight [9]. In addition, deficiencies of essential vitamins and minerals such as iron, vitamin A, and zinc affect an estimated two billion people or almost one-third of the world’s population [5]. These micronutrient deficiencies are often referred to as ‘hidden hunger’ or ‘hidden malnutrition’ as they may invisibly affect the health and development of a population [10]. Many countries have a high prevalence of more than one form of undernutrition. This multiple burdens of undernutrition are more prevalent in LMICs and concentrated amongst the poor [8].
Child undernutrition in South Asia
South Asia and Sub-Saharan Africa have nearly 90% of the world’s underweight children where half live in South Asia [9]. South Asia also bears the highest prevalence globally with 35% of stunted children and wasting prevalence above the 15% threshold along with micronutrient deficiencies [6, 11], all which establish child undernutrition as a ‘critical public health problem’ in the region. Collectively India, Bangladesh, and Pakistan have the highest global levels of disability-adjusted life years (DALYs) attributable to child undernutrition [5]. The three micronutrient deficiencies of iron deficiency anaemia, vitamin A, and zinc, each has a global significance in South Asia [12, 13]. Prevalence of anaemia continues to be a severe public health problem (≥ 40%) in all South Asian countries amongst children of 6–59 months, with the exception of Sri Lanka [5]. Vitamin A deficiency (VAD) affects an estimated 44–50% of preschool children in South Asian regions. In Bangladesh and India, mortality due to VAD and undernutrition constituted one-third of the global mortality rate [14]. Inadequate zinc intake continues to be highly prevalent in South Asia and the zinc deficiency burden is reported to be very high in the region compared with other low-income regions [15]. For instance, zinc deficiency defined as serum zinc concentration < 60 μg/dl was reported to be prevalent amongst 15% of children under 5 years in Afghanistan while in Bangladesh and Pakistan, the prevalence is much higher at 45% and 39%, respectively [5].
South Asia presents a paradox, also commonly known as the ‘South Asia enigma,’ a term used to describe the persistence of high levels of child undernutrition despite economic growth in the region [16]. The region has become the fastest-growing developing region in the world with significant economic progress, marked poverty reduction, improved health indicators, improved literacy rates, and improved agriculture outputs [17,18,19]. This same region also hosts the largest burden on child undernutrition and micronutrient deficiencies along with rapidly increasing rates of child obesity that can have increased risk in adulthood of cardiovascular diseases, cancers, type 2 diabetes, and dementia [20, 21].
UNICEF conceptual framework on child undernutrition
Studies on child undernutrition in individual countries or sub-regions within a country in South Asia have highlighted potential determinants that are consistent with the UNICEF conceptual framework, as part of UNICEF Nutrition Strategy for improving child nutrition (Fig. 1) [22]. The UNICEF conceptual framework on child undernutrition supports the development of interventions from a multi-factorial and multidimensional perspective, moving from micro to meso to macro levels. The framework includes the immediate, underlying, and basic determinants of child undernutrition and outlines that all these factors are interlinked and influence each other. The basic causes address the macro-systemic level challenges reflecting the structural and political processes which result in inadequate financial, human, physical, and social capital that influence household access to adequate quantity and quality of resources. The underlying causes focus on household food security, inadequate care and feeding practices, unhealthy household environment, and inadequate access to health services. The immediate causes of undernutrition such as inadequate food intake and disease are influenced by the basic and underlying causes [22]. The conceptual framework supports the development of multi-factorial interventions and has been modified for specific geographical contexts or with a focus on interventions [23, 24].

UNICEF conceptual framework of the determinants of child undernutrition
At present, there is no study that has collectively and systematically analysed the most consistent factors associated of child undernutrition, including of micronutrient deficiencies along with stunting, wasting, and underweight, across the entire South Asia region. There is also limited evidence that has analysed qualitative evidence (published qualitative articles and grey literature including programme reports and evaluation reports) which has resulted in a limited understanding of the factors of child undernutrition. This mixed-methods review will look at child undernutrition, including stunting, wasting, underweight and micronutrient deficiencies of iron, vitamin A, and zinc, assess its driving factors and identify priorities across the eight countries of South Asia.
Aim of this review and its public health significance
The review is necessary to appraise, synthesise, and summarise the literature on child undernutrition in South Asia. Most studies till date have focused either on undernutrition or on micronutrient deficiencies, and not both. This proposed review will look at various forms of undernutrition in children under 5 years of age, as defined in the scope of the review. It will create an evidence base that looks at multiple faces of macro and micro child undernutrition. It aims to contribute to the growing body of evidence needed to prioritise actions which are focused on the immediate, underlying, and basic determinants of child undernutrition. This review will include grey literature documents, including programme and evaluation reports and working papers. This research is also timely to generate evidence that will contribute to the policy discourse and to the Sustainable Development Goals (SDGs), especially Goal 2: end hunger, achieve food security and improved nutrition, and promote sustainable agriculture [25]. Findings from this study can be used to inform future programme and policy and also for knowledge enhancement and to drive region-specific interventions which could lead to a decline in child undernutrition within the region.
Review question
To assess the past drivers and identify priorities for child undernutrition including stunting, wasting, and underweight and micronutrient deficiencies of iron, vitamin A, and zinc, across eight South Asian countries.
Past drivers of undernutrition will focus on structural, underlying, and immediate determinants of child undernutrition to generate evidence for prioritising and planning for preventive action and identifying high-risk clusters of the population at the regional level.
Methods
Study design
This protocol is informed by the standard Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) reporting guidelines [26]. The PRISMA-P checklist is attached to this manuscript as Additional file 1. This mixed-methods review will look at both quantitative and qualitative evidence including peer-reviewed quantitative, qualitative, and mixed-methods studies and grey literature including programme reports and evaluation reports. The following criteria will be applied for inclusion.
Eligibility criteria
Participants
Children under 5 years of age and those residing in a South Asian country including Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka, as categorised in the United Nations geographical regions [27] will be included in the review. Any studies outside the defined population will be excluded from the review.
Intervention focus and design
Studies to be included in this systematic review will be those that focus on stunting, wasting and underweight and micronutrient deficiencies of iron, vitamin A, and zinc in a South Asian country. However, studies that look at child over nutrition, obesity, or overweight will be excluded.
Both published and unpublished literature [28, 29] will be included. Intervention designs of interest will be intervention studies (both randomised controlled trials (RCTs) and quasi-experimental studies), observational studies (e.g., longitudinal studies, case-control, and cross-sectional studies) as well as qualitative and mixed-methods studies. Unpublished grey literature will include programme and evaluation reports, and working papers. Grey literature such as editorials, dissertation and thesis, conference abstracts, opinion pieces, news articles, books, and book reviews will not be included. The grey literature sources included are based on the most frequently cited grey material in reviews [30]. Inclusion of programme and evaluation reports to the study will serve as a useful source to complement the findings from peer-reviewed literature. Due to resource restrictions, only studies published in English will be included. Studies published between January 2000 and September 2019 will be considered for review because this was the beginning of the Millennium Development Goals (MDGs) and will aid in tracking the progress of the region in line with the MDGs [31]. Aligning the base year of searching with the MDGs allows the outcomes to be more relevant within the international development policy framework. The MDGs created momentum across governments worldwide and formed an internationally agreed blueprint that most countries and leading multilateral and development institutions became signatories. The momentum created by MDGs needs to be sustained through the SGDs. Hence, the proposed systematic review is timely to provide a historical perspective of coordinated international efforts to end child undernutrition and to identify priorities for the SDGs.
Outcomes of interest
Outcomes will include factors and determinants of various forms of child undernutrition and other related outcomes including the following:
Primary outcome: Studies will be included in the review if they report about any one form of child undernutrition including stunting, wasting and underweight and the three micronutrient deficiencies with global significance in South Asia, namely, iron deficiency anaemia, vitamin A, and Zn [12, 13]. Stunting (height-for-age) is an indicator of linear growth retardation and cumulative growth deficits in children. Wasting (weight-for-height) measures body mass in relation to height and describes current nutritional status. However, underweight (weight-for-age) is a composite index of height-for-age and weight-for-height [32]. This systematic review focuses on children with a Z-score below minus two standard deviations (− 2 SD) from the median of the World Health Organisation (WHO) reference population [32, 33]. Anaemia measures in children 6–59 months will be of haemoglobin < 110 g/L, moderate anaemia of haemoglobin 70–99 g/L and severe anaemia of haemoglobin < 70 g/L [34]. Vitamin A deficiency, including both serum retinol concentrations < 10 μg/dL and subclinical vitamin A deficiency (serum vitamin A < 20 μg/dl) will be considered [35, 36]. Zinc deficiency will be considered as recommended by the International Zinc Nutrition Consultative Group [37, 38].
Secondary outcome: the secondary outcomes for this review will include low birth weight, intrauterine growth restriction, maternal body mass index, and maternal iron deficiency anaemia.
Search strategy
The search strategy of this protocol is designed to be as extensive as possible to identify all eligible studies, which will subsequently be refined according to the criteria outlined above. A multi-step search approach will be used to retrieve relevant studies from five academic databases. The databases that would be searched using a variety of subheadings and free-text terms:
-
1.
CINAHL
-
2.
EMBASE
-
3.
PubMed
-
4.
PsycINFO
-
5.
Scopus
A combination of the above-mentioned subheadings and free-text words will also be used to search grey literature in key organisations websites, as listed below. This list might be reviewed when undertaking the research.
-
1.
3ie impact assessment
-
2.
Action Against Hunger
-
3.
Bills and Melinda Gates Foundation (BMGF)
-
4.
Department for International Development (DFID)
-
5.
International Food and Policy Research Institute [10]
-
6.
Medecins Sans frontiers (Doctors without Borders)
-
7.
Nutrition International
-
8.
Save the Children
-
9.
UNICEF
-
10.
World Bank
-
11.
World Food Program
-
12.
World Health Organisation (WHO)
In addition, a lateral approach involving a review of reference lists in relevant papers/reviews will be undertaken. Forward-citation searches will also be undertaken. Search engines such as Google Scholar will be searched in conclusion to include any relevant articles and reports.
Search terms:
Child preschool [MeSH/Subheading] OR infan* [MeSH] OR under-five* OR preschool* OR paediatr* OR bab*
AND
Child malnutrition [MeSH/Subheading] OR Malnutr* [MeSH/Subheading] OR undernutr* [MeSH/Subheading] OR underweight [MeSH/Subheading] OR malnourish* OR undernourish* OR stunt* OR wast* OR “acute malnutrition” “OR chronic malnutrition” OR “micronutrient malnutrition” OR “micronutrient deficiency” OR “vitamin A deficiency” OR “iron deficiency” OR “iron deficiency aneamia” OR Anaemia OR “zinc deficiency”
AND
Caus* [MeSH/Subheading] OR Factor* OR determinant* OR correlate* OR “risk factor” OR multifactorial caus*OR priorit*
AND
“South Asia*” or “Southern Asia*” or Afghan* or Bangladesh* or Bhutan* or India* or Maldives or Nepal* or Pakistan* or Sri Lanka*These search terms provided are a combination of free-text words and the MeSH terms. The MeSH terms were tested in PubMed and were reviewed by all the authors. The School librarian was also consulted to finalise the search strategy. This search syntax has been tested and yielded a manageable number of records. The authors expect around 100–150 studies to be included in the final inclusion.
Data collection
Study selection process
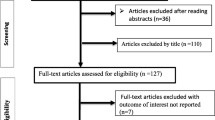
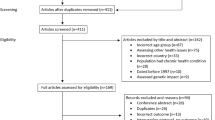
Studies yielded in the search will be imported into EndNote. Endnote software will be used to remove duplicates. The selection of studies will be done in three steps. Firstly, titles will be screened to remove any obviously irrelevant studies followed by the screening of abstracts to confirm eligibility and relevance. After this initial selection, full texts of studies will be reviewed for final inclusion. Final studies selected for full-text screening will be recorded and the reason for their exclusion will be documented in an MS excel sheet. This process will be undertaken independently by two researchers (NW and AR) and any disagreements will be resolved by the third researcher (KA).
Data extraction
The data extraction will comply with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [26]. Data extraction for studies for final included studies will be done using a piloted form including mainly: study details (such as author’s name, year of publication) study design, intervention type, study characteristics (including sample setting, population), and driver of child undernutrition and identified priorities, as documented in Table 1. This process will be undertaken independently by two researchers (NW and AR) and any disagreements will be resolved by the third researcher (KA).
Assessment of methodological quality
Final included studies will be assessed for methodological quality prior to inclusion in the review. The Critical Appraisal Skills Programme (CASP) will be used to assess the methodological quality of qualitative studies [39], randomised controlled trials [40], and observational studies such as longitudinal studies [41] and case-control studies [42]. CASP tool is a widely accepted and used tool to assess the quality of different study designs [43,44,45]. Mixed-methods studies will be assessed based on the MMAT (mixed-methods appraisal tool) by Pluye and colleagues. Grey literature will be appraised with the AACODS tool that looks at authority, accuracy, coverage, objectivity, date, and significance [46]. All studies will be appraised as having a high, medium or low quality and the overall quality of the body of evidence will be used using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [47]. Quality of all studies will be independently appraised by two researchers (NW and AR) and any disagreements will be resolved through discussions. Any further discrepancies will be independently reviewed by the third researcher (KA).
Data synthesis
Due to the heterogeneity and variation of the studies to be reviewed—especially the study methods, measurements, and outcomes—it might not be possible to determine the data synthesis methods priori. A narrative synthesis, a meta-ethnography, or a meta-analysis, as appropriate for the nature of the data retrieved, will be undertaken to understand the factors of and priorities for child undernutrition. The UNICEF conceptual framework of the determinants of child undernutrition will be used to frame the findings that enable to identify relationships between and across various determinants of child undernutrition and identify priorities.
Summary measures
Primary outcome measures will include the factors associated with stunting, wasting, underweight, iron deficiency anaemic, vitamin A deficiency, and zinc deficiency. Secondary outcome measures will include the factors associated with birth weight, intrauterine growth restriction, and maternal iron deficiency anaemia, as well as maternal nutrition status.
Discussion
There is increasing awareness and concern about child undernutrition especially the extent of stunting, wasting, underweight, and micronutrient deficiencies amongst children under 5 years of age, particularly in South Asia. This is also of mounting interest for governments and policy-makers, given its long-term consequences. Though there is ample literature on general nutritional status, there is limited synthesised evidence that collectively looks at micronutrient deficiencies along with stunting, wasting, and underweight. This systematic review will add to the extant literature by synthesising the evidence on the multiple faces of child undernutrition, including stunting, wasting, and micro deficiencies of iron, vitamin A, and zinc across the eight South Asian countries. Findings of this review can inform policies and strategies to combat child undernutrition in the region.
One of the major strengths of this review is the use of a systematic and transparent approach, employing UNICEF conceptual framework for data synthesis. We anticipate some limitations in the review, such as the exclusion of studies published in other languages than English. Exclusion of such studies could lead to missing key literature generated by non-English-speaking researchers and regional organisations. This limitation is addressed, partly, by expanding the search to include relevant grey literature documents from international organisations and by searching google scholar. This review will not look at child over nutrition, obesity, or overweight. This review will only include studies that were published before the year 2000 and could miss relevant articles published before this time frame that might have contributed to this review. In the final review, any discrepancies between the review and the protocol will be explained. We will ensure that the final manuscript is an accurate and transparent account of the review, and that no important aspects of the review will be omitted.
Target audience and dissemination plans
This work has been conducted as part of a PhD dissertation at the School of Social Sciences and Psychology, Western Sydney University. The findings of the review will be shared at conferences and other public forums. Target audience for this review are researchers, practitioners, and policy-makers.
Study registration
This systematic review has been registered with PROSPERO—the International Prospective Register of Systematic Reviews, registration number: CRD42018112696.
Availability of data and materials
Not applicable.
Abbreviations
- AACODS:
-
Authority Accuracy Coverage Objectivity Date and Significance
- BMGF:
-
Bills and Melinda Gates Foundation
- CINAHL:
-
Cumulative Index to Nursing and Allied Health Literature
- DALYs:
-
Disability Adjusted Life Years
- DFID:
-
Department for International Development (United Kingdom Government)
- EMBASE:
-
Excerpta Medica DataBASE
- IFPRI:
-
International Food and Policy Research Institute
- LMICs:
-
Low- and middle-income countries
- MDGs:
-
Millennium Development Goals
- MEDLINE:
-
Medical Literature and Retrieval System Online
- MMAT:
-
Mixed-Methods Appraisal Tool
- PRISMA-P:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- RCTs:
-
Randomised controlled trials
- SDs:
-
Standard deviations
- UNICEF:
-
United Nations International Children’s Emergency Fund
- VAD:
-
Vitamin A deficiency
- WHO:
-
World Health Organisation
References
United Nations United Nations International Children’s Fund; World Health Organization; & The World Bank. Joint child malnutrition estimates-levels and trends. New York, Geneva, Washington, DC; UNICEF, WHO, The World Bank; 2011.
Akhtar S. Malnutrition in South Asia—a critical reappraisal. J Crit Rev Food Sci Nutr. 2016;56(14):2320–30. https://doi.org/10.1080/10408398.2013.832143.
Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371(9608):243–60.
Martorell R. The nature of child malnutrition and its long-term implications. Food Nutr Bull. 1999;20(3):288–92.
Harding K, Aguayo V, Webb P. Hidden hunger in South Asia: a review of recent trends and persistent challenges. Public Health Nutr. 2018;21(4):785–95.
UNICEF. Child stunting, hidden hunger and human capital in South Asia: implications for sustainable development post 2015. Kathmandu: UNICEF; 2018. Available at https://www.unicef.org/rosa/media/1611/file/Child%20stunting,%20hidden%20hunger%20and%20human%20capital%20in%20South%20Asia.pdf.
Stewart CP, Iannotti L, Dewey KG, Michaelsen KF, Onyango AW. Contextualising complementary feeding in a broader framework for stunting prevention. Matern Child Nutr. 2013;9(S2):27–45.
Food and Agriculture Organisation. 2018, The state of food insecurity and nutrition in the world 2018. Available from: http://www.fao.org/state-of-food-security-nutrition/en/.
United Nations. The millenium development goals report 2015. New York: United Nations; 2015.
IFPRI, Welt Hunger Hilfe, CONCERN worldwide. Global hunger index: the challenge of hidden hunger. Bonn/Washington,D.C./Dublin: IFPRI, Welt Hunger Hilfe, CONCERN worldwide; 2014.
Harding KL, Aguayo VM, Webb P. Factors associated with wasting among children under five years old in South Asia: implications for action. PLoS One. 2018;13(7):e0198749.
Akhtar S, Ismail T, Atukorala S, Arlappa N. Micronutrient deficiencies in South Asia a current status and strategies. Trends Food Sci Technol. 2013;31(1):55–62.
Sumithra M, Jee Hyun R, Jonathan DS, Franz FR, Klaus K, Robert EB. The global hidden hunger indices and maps: an advocacy tool for action. (research article). PLoS One. 2013;8(6):e67860.
Akhtar S, Ahmed A, Randhawa MA, Atukorala S, Arlappa N, Ismail T, et al. Prevalence of vitamin a deficiency in South Asia: causes, outcomes, and possible remedies.(report). J Health Popul Nutr. 2013;31(4):413.
Wessells KR, Brown KH. Estimating the global prevalence of zinc deficiency: results based on zinc availability in national food supplies and the prevalence of stunting. PLoS One. 2012;7(11):e50568.
Vulimiri Ramalingaswami, Urban Jonsson, Jon Rohde. Commentary: The Asian enigma: UNICEF; 1996. Available from: https://www.unicef.org/pon96/nuenigma.htm.
Headey D, Hoddinott J, Ali D, Tesfaye R, Dereje M. The other Asian enigma: explaining the rapid reduction of undernutrition in Bangladesh. World Dev. 2015;66:749–61.
Akhmat G, Zaman K, Shukui T, Javed Y, Khan S. Social health indicators and economic growth: evidence from East Asia and Pacific, Middle East and North Africa, South Asia, and Sub-Saharan Africa. Soc Indic Res. 2014;119(2):663–86.
Bank W. South Asia Economic Focus, Spring 2016: Fading Tailwinds. Washington, DC: World Bank; 2016.
International Food and Policy Research Institute. Global nutrition report 2015: actions and accountability to advance nutrition and sustainable development. Washington DC: IFPRI; 2015.
Ranjani H, Mehreen T, Pradeepa R, Anjana R, Garg R, Anand K, et al. Epidemiology of childhood overweight & obesity in India: a systematic review. (systematic review)(report). Indian J Med Res. 2016;143(2):160.
United Nations International Children’s Fund. Multi-sectoral approaches to nutrition: nutrition-specific and nutrition-sensitive interventions to accelerate progress. New York: UNICEF; 2014.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–51.
Levitt EJ, Pelletier DL, Pell AN. Revisiting the UNICEF malnutrition framework to foster agriculture and health sector collaboration to reduce malnutrition: a comparison of stakeholder priorities for action in Afghanistan. Food Policy. 2009;34(2):156–65.
United Nations. Sustainable Development Goals: Overview 2018. Available from: https://unstats.un.org/sdgs/report/2016/goal-02/.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1.
United Nations International Children’s Fund. The State of the World’s Children 2014 in Numbers: Every Child Counts. Revealing Disparities, Advancing Children’s Rights. New York: United Nations International Children’s Fund; 2014.
Mahood Q, Van Eerd D, Irvin E. Searching for grey literature for systematic reviews: challenges and benefits. Res Synth Methods. 2014;5(3):221–34.
Godin K, Stapleton J, Kirkpatrick SI, Hanning RM, Leatherdale ST. Applying systematic review search methods to the grey literature: a case study examining guidelines for school-based breakfast programs in Canada. Syst Rev. 2015;4:138.
Adams Richard J, Smart P, Huff Anne S. Shades of Grey: guidelines for working with the Grey literature in systematic reviews for management and organizational studies. Int J Manag Rev. 2016;19(4):432–54.
UN Millennium Project. Investing in development: a practical plan to achieve the millennium development goals. New York: UNDP; 2005.
WHO Multicentre Growth Reference Study Group. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: World Health Organization; 2006.
Who Multicentre Growth Reference Study Group. WHO child growth standards based on length/height, weight and age. Acta Paediatr. 2006;450:76–85.
World Health Organisation. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva: World Health Organisation; 2018.
Gassmann B. Control of vitamin a deficiency and Xerophthalmia. Report of a joint WHO/UNICEF/USAID/Helen Keller international/IVA CG meeting. 74 seiten, 7 Abb., 15 tab. WHO technical report series 672. World Health Organization, Geneva 1982. Preis: 7,- sfrs. Food Nahrung. 1982;26(9):837.
Kurugöl, Egemen, Keskinoğlu, Darcan, Akşit. Vitamin A deficiency in healthy children aged 6–59 months in İzmir Province of Turkey. Paediatr Perinat Epidemiol. 2000;14(1):64–9.
Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lönnerdal B, et al. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004;25(1 Suppl 2):S99.
World Health Organisation. Conclusions of the joint WHO/UNICEF/IAEA/IZiNCGInteragency meeting on zinc status indicators. Food Nutr Bull. 2007;28:3.
Critical Appraisal Skills Programme. Ten questions to help you make sense of qualitative research. 2017. Available from: http://docs.wixstatic.com/ugd/dded87_25658615020e427da194a325e7773d42.pdf.
Critical Appraisal Skills Programme (CASP). 11 questions to help you make sense of a randomised controlled trial: CASP. Available from: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Randomised-Controlled-Trial-Checklist-2018.pdf.
Critical Appraisal Skills Programme (CASP). 12 questions to help you make sense of a cohort study: CASP; Available from: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist_2018.pdf.
Critical Appraisal Skills Programme (CASP). 11 questions to help you make sense of a case control study: CASP; Available from: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Case-Control-Study-Checklist-2018.pdf.
Paudyal V, Cunningham S, Gibson Smith K, MacLure K, Ryan C, Cordina M. Methodological considerations in clinical outcomes assessment of pharmacy-based minor ailments management: a systematic review. PLoS One. 2018;13(10):1.
Senra H, Barbosa F, Ferreira P, Vieira CR, Perrin PB, Rogers H, et al. Psychologic adjustment to irreversible vision loss in adults: a systematic review: a systematic review. Ophthalmology. 2015;122(4):851–61.
Smith T, Maidment I, Hebding J, Madzima T, Cheater F, Cross J, et al. Systematic review investigating the reporting of comorbidities and medication in randomized controlled trials of people with dementia. Age Ageing. 2014;43(6):868–72.
Tyndall J. AACODS Checklist.: Flinders University. 2010. Available from: https://dspace.flinders.edu.au/jspui/bitstream/2328/3326/4/AACODS_Checklist.pdf.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. Rating quality of evidence and strength of recommendations: GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Acknowledgements
This work has been conducted as part of a PhD dissertation at the School of Social Sciences and Psychology, Western Sydney University.
Funding
No specific funding has been sought for this systematic review. In addition, the review has not been sponsored by anyone else other than the authors.
Author information
Authors and Affiliations
Contributions
NW and AR conceived the original research idea. NW developed the first draft of the protocol. AR supervised the entire manuscript writing and contributed to the revision of the first draft and subsequent revisions of the protocol. KA edited the manuscript and enhanced its intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
PRISMA-P checklist. (DOCX 33 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wali, N., Agho, K. & Renzaho, A.M.N. Past drivers of and priorities for child undernutrition in South Asia: a mixed methods systematic review protocol. Syst Rev 8, 189 (2019). https://doi.org/10.1186/s13643-019-1112-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-019-1112-7