
Abstract
Background
Under nutrition is linked with poor water, sanitation and hygiene (WASH) condition. However, there is conflicting evidence on the effect of WASH on nutritional status of children. This review was, therefore, conducted to estimate the pooled effect of WASH interventions on child under nutrition.
Methods
All published and unpublished cluster-randomized, non-randomized controlled trials, and before and after intervention studies conducted in developing countries were included. Relevant articles were searched from MEDLINE/PubMed, Cochrane Collaboration’s database, Web of Science, WHO Global Health Library, Google Scholar, Worldcat and ProQuest electronic databases. The methodological quality of the included studies was assessed using JBI critical appraisal checklist for randomized and non-randomized controlled trials. The risk of bias was assessed using the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. The treatment effect was expressed as standardized mean differences (SMD) with 95% confidence interval (CI).
Results
This meta-analysis of 10 studies including 16,473 children (7776 in the intervention and 8687 in the control group) indicated that WASH interventions significantly associated with increased pooled mean height-for-age-z-score (SMD = 0.14, 95% CI = (0.09, 0.19); I2 = 39.3%]. The effect of WASH on HAZ was heterogeneous in age and types of interventions. WASH intervention had more effect on HAZ among under two children [SMD = 0.20, 95% CI = (0.11, 0.29); I2 = 37%]. Children who received combined WASH interventions grew better compared with children who received single interventions [SMD = 0.15, 95% CI = (0.09, 0.20); I2 = 43.8%].
Conclusion
WASH interventions were significantly associated with increased mean height-for-age-z score in under 5 years old children. The effect of WASH on linear growth is markedly different with age and types of interventions, either single or combined. Implementing combined WASH interventions has a paramount benefit to improve nutritional status of children.
Similar content being viewed by others


Background
Children are the most vulnerable group to a wide range of infections unless special attention is given. The highest proportions of infections among children are poor WASH related diarrheal and parasitic diseases. Globally, there are nearly 1.7 billion cases of childhood diarrheal disease every year and diarrhea is responsible for killing around 525,000 children every year [1]. About 3.5 billion people (the majority of these cases were children) in the world were infected with intestinal parasites caused by helminthes and protozoa during 2009 [2].
Repeated exposure to diarrheal and parasitic infections causes environmental enteropathy (EE) or sometimes called environmental enteric dysfunction (EED). EE is an inflammatory condition of the gut of children which is characterized by villous atrophy, crypt hyperplasia, increased permeability, inflammatory cell infiltrate, and modest malabsorption [3,4,5].
Diarrhea, parasitic infections and EE are key mediating pathways linking poor WASH to developmental deficit [6,7,8]. A large body of evidence suggests that malnutrition is linked with poor WASH practice [9,10,11,12]. Poor WASH is associated with under nutrition as a result of diarrhea, nematode infection and EE. Diarrhea and intestinal worms cause nutrient losses and diversion of nutrients from growth to the immune system to fight the infection [13,14,15,16,17,18,19]. EE increases the small intestine’s permeability and reduces nutrient absorption [20,21,22,23,24]. The link of poor WASH and under nutrition has also socio-economical mechanism. For instance the energy cost of carrying water for long distances from the source to home. The average woman carrying a typical load of 20 l on level ground would consume about 39 cal per kg of body weight per hour with an assumption that 1 g of maize meal yields 3.5 cal [25].
WASH interventions are the most holistic and effective approaches to prevent stunting and wasting among under two children. However, there is conflicting evidence on the effect of WASH on linear growth. Some studies reported that there is no significant association between WASH and linear growth [26,27,28,29,30] and some others reported that WASH has significant effect [8, 31,32,33]. This systematic review and meta-analysis was, therefore, aimed to estimate the pooled effect of WASH on linear growth among under five children.
Methods
Research question
Does access to improved WASH facilities have effect on child growth?
Criteria for considering studies for this review
Types of studies
All published and unpublished community-based trials (including cluster-randomized, quasi-randomized, non-randomized controlled trials, controlled before and after intervention studies) conducted in developing countries to analyze the effect of WASH on the mean height-for-age- z score were included. Studies published in English language in the last 10 years were also included. Citations with no abstracts and/or full texts, duplicate studies, and studies with poor quality were excluded.
Types of participants
Children aged under 5 years.
Types of interventions
-
1.
Any intervention aimed at improving the microbiological quality of drinking water, including household and community level water treatment, water source protection and household water handling.
-
2.
Interventions aimed to reduce direct and indirect contact with human faeces (pour flush, water sealed flush toilet, piped sewer system, septic tank, simple pit latrines, VIP latrine or use off scoop for the disposal of child faeces).
-
3.
Interventions aimed at the promotion of hand washing with soap or ash after defecation, disposal of child faeces and prior to preparing and handling food
-
4.
Any WASH promotion aimed at WASH behavioral change like community-led total sanitation (CLTS)
-
5.
Any combination of the WASH interventions listed above
Control
-
1.
Water quality: participants who continued with usual practice, or a less stringent version of the intervention (i.e. new protected well but no household disinfection).
-
2.
Sanitation: participants who continued with usual practice rather than following the prescribed intervention.
-
3.
Hygiene: no hand washing promotion and participants who continued with usual practice.
-
4.
WASH promotion: participants who did not receive WASH behavioral change education
Types of outcome measures
Child nutritional status or stunting measured by mean height-for-age-z score.
Search strategy and study selection
We searched relevant articles from MEDLINE/PubMed, Cochrane Collaboration’s database, Web of Science, WHO Global Health Library, Google Scholar, Worldcat and ProQuest. A three-step search strategy was utilized in this review. An initial limited search of MEDLINE was undertaken followed by analysis of the text words contained in the title and abstract, and of the index terms used to describe articles. A second search using all identified keywords and index terms was undertaken across all included databases. Thirdly, references of all identified articles were searched to get additional studies. The below box shows terms used to search literatures.
(((“child”[MeSH Terms] OR “child”[All Fields] OR “children”[All Fields]) OR (“child”[MeSH Terms] OR “child”[All Fields])) AND ((((((((“sanitation”[MeSH Terms] OR “sanitation”[All Fields]) OR “Wastemanagement”[All Fields]) OR “Latrine utilization”[All Fields]) OR “Water quality”[All Fields]) OR “Food hygiene”[All Fields]) OR “Personal hygiene”[All Fields]) OR “Hand washing”[All Fields]) OR “Water, sanitation and hygiene”[All Fields])) AND ((((((((“malnutrition”[MeSH Terms] OR “malnutrition”[All Fields] OR “undernutrition”[All Fields]) OR (“malnutrition”[MeSH Terms] OR “malnutrition”[All Fields])) OR (“growth disorders”[MeSH Terms] OR (“growth”[All Fields] AND “disorders”[All Fields]) OR “growth disorders”[All Fields] OR “stunting”[All Fields])) OR “Linear growth deficit”[All Fields]) OR “Growth faltering”[All Fields]) OR “Growth failure”[All Fields]) OR “Growth impairment”[All Fields]) OR “Growth disorder”[All Fields]) |
Assessment of methodological quality
Search results from different electronic databases were exported to Endnote reference manager to remove duplication. We screened out articles using titles and abstracts. We further investigated and assessed full-text articles against the inclusion and exclusion criteria. The methodological quality of the included studies was assessed using JBI critical appraisal checklist for randomized and non-randomized controlled trials (Additional file 1) [34].
Data extraction
We independently extracted data from papers included in the review using the JBI standardized data extraction tool (Additional file 2). The data extraction form was piloted on randomly selected papers and modified accordingly. Eligibility assessment was performed independently by the two reviewers. We invested our maximum effort to avoid introduction of errors (e.g. entering wrong numerals into a spreadsheet and failure to identify required data from a study report) or bias during extraction. Data were systematically extracted relating to the nature of studies.
Assessment of risk of bias in included studies
We independently assessed the risk of bias of included studies using the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials [35]. Random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other possible risk of bias (buffer to prevent information contamination and measure or adjust potential confounders) were items used to assess risk of bias. We assessed studies for each item with answers of ‘low’ indicating low risk of bias, ‘high’ indicating high risk of bias and ‘unclear’ indicating either lack of information or uncertainty over the potential for bias (Additional file 3).
Measures of treatment effect
Stata version 11 was used to measure treatment effect and to conduct other analysis. We expressed treatment effect sizes as SMD with 95% CI using their original scale. We used forest plot to present results.
Sensitivity analysis
Sensitivity analysis was carried out to see the impact of individual studies for the pooled result.
Assessment of heterogeneity
We assessed statistical heterogeneity using the I2 statistics. Galbraith plot was also used to observe heterogeneity.
Assessment of publication bias
Funnel plot was used to see publication bias subjectively and Egger’s test was used to objectively check potential publication bias.
Dealing with missing data
We contacted authors of potentially relevant studies that did not report the outcome and asked them to provide information on the availability of outcome data. Articles with incomplete data were excluded from the meta-analysis while they were included in the systematic review.
Results
The search process
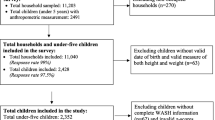
The search strategy identified 815 titles and abstracts (663 from PubMed and 152 from other sources) published before 11 August 2018. We obtained 782 articles after we removed duplicated articles. Following assessment by title and abstract, 153 articles were retrieved for more evaluation. Twelve articles were included for systematic review and 10 articles were included for meta-analysis based on the inclusion criteria. Of the 12 included reports, 9 were published in journals, one was a CEDLAS report, one was a Feinstein International Center report and one was dissertation. All of the included studies were published in English. The study selection process is outlined in Fig. 1.

Study selection flow diagram
Description and characteristics of included studies
Two studies [Arnold, 2009 and Langford, 2011] were non-randomized trial and the rest were randomized trial. All included studies were conducted in low-income or middle income country settings. Two studies were conducted in Mali [Alzua, 2015 and Pickering, 2015], two in Uganda [Marshak, 2015 and Muhoozi, 2017], two in India [Clasen, 2014 and Patil, 2014], One in Bangladesh [Shafique, 2013], one in Kenya [Arnold, 2018], one in Pakistan [Bowen, 2012], one in Guatemala [Arnold, 2009], one in Cambodia [McGuigan, 2011] and one in Nepal [Langford, 2011].
Intervention duration was ranged from 6 to 36 months. Three interventions were implemented for 6 months [Muhoozi, 2017; Marshak, 2015 and Langford, 2011], One intervention for 9 months [Bowen, 2012], one intervention for 10 months [Alzua, 2015], two interventions for 12 months [Shafique, 2013 and McGuigan, 201], one intervention for 13 months [Clasen, 2014], one intervention for 17 months [Pickering, 2015], one intervention for 21 months [Patil, 2014], one intervention for 24 months [Arnold, 2018], and one intervention for 36 months [Arnold, 2009]. Two studies [Alzua, 2015 and Pickering, 2015] implemented CLTS, one study [Patil, 2014] implemented total sanitation campaign (TSC), one study [Arnold, 2018] implemented WASH and nutrition, two studies [Marshak, 2015 and Muhoozi, 2017] implemented nutrition and food hygiene, one study [Arnold, 2009] implemented water treatment and hand washing, one study [Shafique, 2013] implemented nutrition, health and hygiene education and hand hygiene, two studies [Bowen, 2012 and Langford, 2011] implemented hand washing, one study [McGuigan, 2011] implemented home based water treatment, and one study [Clasen, 2014] implemented latrine construction and promotion.
Height-for-age-z score was reported in all studies. Except two studies [McGuigan, 2011 and Arnold, 2018], all others measured weight-for-age z-scores, five studies [Alzua, 2015; Arnold, 2018; Marshak, 2015; Pickering, 2015 and Shafique, 2013] reported stunting, three studies [Alzua, 2015; Marshak, 2015 and Pickering, 2015] reported underweight, three studies [Muhoozi, 2017; Patil, 2014 and Arnold, 2009] reported mid upper arm circumference z-scores, one study [Muhoozi, 2017] reported head circumference z-scores, two studies [Bowen, 2012 and Patil, 2014] reported body mass index, nine studies [Alzua, 2015; Arnold, 2018; Bowen, 2012; Clasen, 2014; Pickering, 2015; Arnold, 2009; Langford, 2011; McGuigan, 2011; and Shafique, 2013] reported diarrhea, five studies [Alzua, 2015; Pickering, 2015; Arnold, 2009; Langford, 2011 and Shafique, 2013] reported respiratory illness, two studies [Clasen, 2014 and Patil, 2014] reported STHs, one study [Patil, 2014] reported anemia, three studies [Arnold, 2018; Bowen, 2012 and Muhoozi, 2017] reported child development quotients, and one study [Arnold, 2018] reported markers of EE.
Risk of bias in included studies
Allocation
With the exclusion of the two non-randomized studies [Arnold, 2009 and Langford, 2011], we judged sequence generation is adequate in all other studies. All other studies allocated the intervention and control groups randomly. Random number generator [Arnold, 2018; Bowen, 2012 and Pickering, 2015], computer generated sequence [Clasen, 2014 and Shafique, 2013] and raffle system [McGuigan, 201]) were used to generate random sequence. However, allocation concealment was not possible in all studies except Bowen, 2012.
Blinding
Four of the include studies [Alzua, 2015; Bowen, 2012; Clasen, 2014 and Muhoozi, 2017] made study participants or personnel blind and we judged these studies to be at low risk of performance bias. Alzua, 2015; Arnold, 2018; Bowen, 2012; Clasen, 2014 and Pickering, 2015 concealed group allocation from personnel who measured outcome variables in and thus judged to be at low risk of detection bias.
Incomplete outcome data
There was lose of follow-up in all studies, however the majority of studies [Alzua, 2015; Arnold, 2018; Clasen, 2014; McGuigan, 2011; Muhoozi, 2017; Patil, 2014; Pickering, 2015 and Shafique, 2013] balanced participants in both arms and conducted intention-to-treat analysis to manage attrition bias and we judged these studies to be at low risk of attrition bias.
Selective reporting
We assessed the trial registries and protocols of six studies; Arnold, 2018 and McGuigan, 2011 were not reported as per protocol. We found Alzua, 2015; Bowen, 2012; Patil, 2014 and Shafique, 2013 reported as per protocol.
Other potential sources of bias
We assessed authors’ investment to prevent information cross contamination among clusters and potential effect of confounders. Alzua, 2015; Marshak, 2015 and Pickering, 2015 used buffer to prevent information contamination and Patil, 2014 and Shafique, 2013 measured and adjusted anticipated confounders (see Figs. 2 and 3 for the risk summary of studies).

Risk of bias summary: review authors’ judgments about each risk of bias item for each included study

Risk of bias graph: review authors judgment about each risk of bias item presented as percentages across all included studies
Effects of WASH interventions on linear growth
Different community-based randomized and non-randomized trials discussed the effect of single or/and combined WASH interventions on child linear growth (expressed as mean height-for-age-z score in this study). The effect of WASH interventions on mean height-for-age-z score is summarized below.
Alzua, 2015 was a cluster-randomized controlled trial conducted among 7328 (3564 in the control arm and 3764 in the intervention arm) children in Mali. This study reported that children in CLTS villages were taller (0·18 increase in height-for-age- z score, 95% CI 0.03–0.32) and less likely to be stunted (PR 0·86, 95% CI 0·74–1·0) compared to children in the control arm.
Arnold, 2009 was a non-randomized intervention conducted among 877 children under 5 years of age in Guatemala. Compared to children in the control, a water quality and hand washing intervention had no effect on weight- for-age- z score (MD = − 0.053, 95% CI = (− 0.331, 0.206), weight-for-height-z score (MD - 0.066, 95% CI = (− 0.248, 0.124), height-for-age- z score (MD = 0.041, 95% CI = (− 0.305, 0.326) or mid-upper arm circumference (cm) (MD = − 0.014, 95% CI = (− 0.166, 0.145).
Arnold, 2018 was a cluster-randomized controlled trial conducted in Kenya among 2101children (364 in the intervention arm and 1737 in the control arm) and in Bangladesh among 712 children (199 in the intervention arm and 513 in the control arm). The study reported that children who had access to improved latrine were taller [MD = 0·15, 95% CI = (0·02–0·28] in Kenya and [MD = 0·22, 95% CI = (0·03–0·40)] in Bangladesh.
Bowen, 2012 was a cluster-randomized controlled trial conducted in Pakistan among 461 children (160 in the control group, 141 in the hand washing group and 160 in hand washing and water treatment group). This study found that 24.9% (95% CI, 20.0–30.6%) and of children had z scores that were more than 2 SDs below the expected z score for height for age which did not differ significantly across study groups.
Clasen, 2014 was a cluster-randomized controlled trial conducted in India among 24, 969 individuals in intervention villages and 25, 982 individuals in control villages. The study reported that the mean height-for-age-z-score was not significantly differ between children from households with functional latrine and with no functional latrine [MD = − 0·06, 95% CI = (− 0·27 to 0·15)].
Langford, 2011 was a non-randomized controlled trial study among 88 children under 1 year of age in Nepal to see the effect of hand washing on subclinical infections and growth. The study reported that hand washing intervention had no effect on weight-for-age z-score (MD = − 0.24, 95% CI = (− 0.76, 0.28), weight-for-height z-score (MD = − 0.11, 95% CI = (− 0.53, 0.31) or height-for-age z-score (MD = − 0.13, 95% CI = (− 0.54, 0.28).
Marshak, 2015 was a randomized control trial conducted in Uganda to see the impacts of a program entitled “Community Resilience to Acute Malnutrition”. This study included 1762 children in the control group (647 children in the baseline, 572 children in the midline, 543 in the endline) and 1656 children in the WASH intervention group (614 children in the baseline, 555 children in the midline, and 487 in the endline). The report of the assessment indicated that children living in intervention settlements were less likely to be stunted compared to children living in non-intervention settlements. This relationship is further supported by a significant difference between intervention (HAZ = − 1.07) and non-intervention (HAZ = − 1.27) settlements.
McGuigan, 2011 was a cluster-randomized controlled trial conducted among 928 children (nutrition outcome data were available for 760 children) under 5 years of age in Cambodia to the impact of solar disinfection of drinking water on childhood diarrhea. Compared to children in the control arm, a water quality (SODIS) intervention had no effect on weight-for-age- z score (MD = 0.26, 95% CI = (− 0.01, 0.53), weight-for-height- z score (MD = 0.15, 95% CI = (− 0.15, 0.45) or height-for-age- z score (MD = 0.22, 95% CI = (− 0.04, 0.48).
Muhoozi, 2017 was a community-based, open cluster-randomized trial conducted in Uganda among 511 children aged 6–8 months (263 in the intervention group and 248 in the control group). This study revealed that there was no evidence of a difference in mean length-for-age- z score at 20–24 months between the two study groups [MD = 0.10, 95% CI = (− 0.17, 0.36)].
Patil, 2014 was a cluster-randomized controlled trial conducted in India among 5209 children (2609 in the control arm and 2600 in the intervention arm) to see the effect of India’s total sanitation campaign on defecation behaviors and child health. The study depicted that the intervention had no significant effect on length/height-for-age-z score (HAZ in the control group = − 1.38 and in the intervention group = − 1.81).
Pickering, 2015 was a cluster-randomized controlled trial conducted in Mali to see the effect of CLTS on child diarrhea and child growth. Researchers enrolled 2365 households to receive the CLTS intervention and 2167 households to the control group. The finding of the study showed that children in CLTS villages were taller (0·18 increase in height-for-age-z score, 95% CI 0·03–0·32) and less likely to be stunted (35% versus 41%, PR 0·86, 95% CI 0·74–1·0) than children in control villages.
Shafique, 2013 is a randomized controlled trial conducted in Bangladesh to measure the relative effect of directed use of benzalkonium chloride-containing, water-based hand sanitizers and broad-range multiple micronutrient powder (MNP) along with nutrition, health and hygiene education (NHHE) to prevent infections and linear growth faltering reported that combined intervention of directed hand-sanitizer use and micronutrient powder along with NHHE significantly improved linear growth of low birth weight infants compared to NHHE alone.
This systematic review and meta-analysis of 10 studies including 16,473 children (7776 in the intervention group and 8687 in the control group) indicated that single or/and combined WASH interventions significantly associated with increased mean height-for-age-z-score (SMD = 0.14, 95% CI = (0.09, 0.19); I2 = 39.3%] (Fig. 4).

Forest plot of comparison: height-for-age-z score (all community-based trial studies)
Assessment of heterogeneity
The I2 statistics of the aggregate pooled estimate (I2 = 39.3%) showed moderate heterogeneity. As a result, Galbraith plot was used to observe heterogeneity. The plot indicated that Patil S, 2014 caused the heterogeneity (Fig. 5).

Galbraith plot for heterogeneity
Subgroup analysis
A subgroup analysis by age showed that single or/and combined WASH intervention had more effect on mean height-for-age-z score among under two children compared with under 5 years old children[SMD = 0.20, 95% CI = (0.11, 0.29); I2 = 37%] (Fig. 6).

Forest plot of comparison: height-for-age-z score (subgroup analysis by age)
A subgroup analysis by type of WASH interventions (single interventions and combined interventions) was done. The result of the analysis showed that combined WASH interventions significantly associated with increased mean height-for-age-z score. Children who received combined WASH interventions grew better compared with children who received single interventions [SMD = 0.15, 95% CI = (0.09, 0.20); I2 = 43.8%] (Fig. 7).

Forest plot of comparison: height-for-age-z score (subgroup analysis by intervention)
Sensitivity analysis
The sensitivity analysis test result showed that the pooled effect of WASH intervention on the mean height-for-age-z score was 0.19 [SMD = 0.19, 95% CI = 0.15, 0.23]. There are studies which become out of the pooled result when they are out of the analysis. The maximum impact for these studies was from 0.13 to 0.26, which is a 95% CI. There was no any significant difference of each study for the total pooled result (Fig. 8).

Sensitivity analysis to assess the impact of individual studies to the mean height-for-age-z score pooled estimate
Publication bias
The funnel plot (Fig. 9) and Egger’s test (Table 1) show that there was no publication bias. The funnel plot is symmetric and p value for Egger’s test is 0.988.

Funnel plot with pseudo 95% CI to show publication bias
Discussion
Summary of evidence
Twelve studies are included in this review. The review included ten community-based cluster-randomized controlled trials and two non-randomized community based trials. Studies included various water, sanitation and hygiene (WASH) interventions either singly or in combination. Most of the included studies were considered to be at low risk of bias. Height-for-age-z-score, the primary outcome variable of this review was available from all studies. However, two of the studies didn’t report SD for the mean height. As a result, the meta-analysis was limited to data from ten studies.
In this systematic review and meta-analysis, WASH interventions significantly associated with increased height-for-age z-scores in children. The report of this review is consistent with the reports of other systematic reviews. For instance, a systematic review and meta-analysis which included seven RCT comparators reported that WASH intervention was marginally associated with mean height-for-age-z score (MD = 0.08, 95% CI = 0.00–0.16)) [36]. Similarly, a review conducted on the impact of combined WASH intervention on growth, non-diarrheal morbidity and mortality in children residing in low and middle-income countries found that WASH interventions improved height-for-age-z scores (MD = 0.22; 95% CI 0.12, 0.32) and decreased the risk of stunting by 13% (RR = 0.87; 95% CI = 0.81, 0.94)) [37]. Other individual studies also reported that WASH interventions were significantly associated with children’s height [38,39,40,41]. The link of WASH and increased mean height-for-age-z score is due to improved WASH condition prevents diarrhea and parasitic infections which could cause reduced absorption and nutrient losses, reduced appetite, and diversion of energy and nutrients from growth to the immune system to fight the infection [13,14,15,16,17,18,19]. Improved WASH prevents EE which increases the small intestine’s permeability and reduces nutrient absorption [20,21,22,23,24].
This systematic review and meta-analysis indicated that WASH interventions are more effective to improve childhood nutrition among under two children compared with interventions in under five children. This might be due to the fact that the first 2 years of life are the window to child’s future. Exposed to sanitation related diarrheal and intestinal parasitic infections in the first 1000 days of a child’s life causes irreversible, long-term damage to a child’s health. Nutritional interventions during this time [42, 43].
We found that combined WASH interventions were more effective to improve child nutritional status than single interventions. This can be justified that the exposures to faecal-oral pathogens through drinking water, sanitation or hygiene, which is the mediating pathway to WASH and nutrition is complex. Hand washing or treatment of drinking water or food safety or sanitation alone cannot prevent the occurrence of faecal-oral diseases. The integration of interventions is effective to prevent infections and to promote nutrition status [44, 45].
Applicability of evidence
There is suggestive evidence from cluster-randomized controlled trials on the effect of WASH interventions on nutritional status of children. However, there is limited evidence on the effect of WASH interventions on nutritional outcomes in children. We believe, the result of this meta-analysis provides supportive evidence on the effect of WASH interventions on nutritional status of children. The finding of this review provides evidence for policy makers, health practitioners, WASH and nutrition advocators to enhance child health, child nutrition and sanitation condition, and to prevent sanitation related infectious diseases. Further large scale studies designed to measure the impact of WASH interventions on nutritional outcomes in children are needed.
Limitation
We entirely relied on freely access electronic databases to search relevant articles. We didn’t include articles available in hard copy. During the process of the review, we identified one study that collected but did not report nutritional outcomes in children. It is possible that other studies which we did not identify collected data on child nutritional status and WASH that we have been unable to include in this review. Due to these, the searching was not exhaustive. We believed we could get more relevant articles if we had access to other databases and hard prints.
Conclusion
WASH interventions were significantly associated with increased mean height-for-age-z score in under 5 years old children. The effect of WASH on linear growth is markedly different with age and types of WASH interventions, either single or combined. Implementing combined WASH interventions has a paramount benefit to improve nutritional status of children.
Availability of data and materials
The extracted data will be made available upon requesting the primary author.
Abbreviations
- CI:
-
Confidence interval
- CLTS:
-
Community leading total sanitation
- c-RCT:
-
Clustered randomized controlled trial study
- HAZ:
-
Height-for-age-z score
- HS:
-
Hand sanitizers
- JBI:
-
The Joanna Briggs Institute
- MD:
-
Mean difference
- MNP:
-
Multiple micronutrient powder
- NHHE:
-
Nutrition, health and hygiene education
- RCT:
-
Rndomized controlled trial
- SD:
-
Standard deviation
- SMD:
-
Standardized mean difference
- TS:
-
Total sanitation
- VIP latrine:
-
Ventilated improved latrine
- WASH:
-
Water, sanitation and hygiene
- WAZ:
-
Weight-for-age-z score
- WHO:
-
World health organization
References
WHO. Diarrhoeal disease. WHO online liberary 2017;Available at http://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease. Accessed 11 Sept 2018.
Brooker S, Kabatereine NB, Smith JL, Mupfasoni D, Mwanje MT, Ndayishimiye O, et al. An updated atlas of human helminth infections: the example of East Africa. Int J Health Geogr. 2009;8(1):42.
Kelly P, Menzies I, Crane R, Zulu I, Nickols C, Feakins R, et al. Responses of small intestinal architecture and function over time to environmental factors in a tropical population. Am J Trop Med Hyg. 2004;70(4):412–9.
Crane RJ, Jones KD, Berkley JA. Environmental enteric dysfunction: an overview. Food Nutr Bull. 2015;36(1_suppl1):S76–87.
Brown J, Cairncross S, Ensink JH. Water, sanitation, hygiene and enteric infections in children. Arch Dis Child. 2013;98(8):629–34.
Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E, et al. What works? Interventions for maternal and child undernutrition and survival. Lancet. 2008;371(9610):417–40.
Checkley W, Gilman RH, Black RE, Epstein LD, Cabrera L, Sterling CR, et al. Effect of water and sanitation on childhood health in a poor Peruvian peri-urban community. Lancet. 2004;363(9403):112–8.
Lin A, Arnold BF, Afreen S, Goto R, Huda TMN, Haque R, et al. Household environmental conditions are associated with enteropathy and impaired growth in rural Bangladesh. The American journal of tropical medicine and hygiene. 2013;89(1):130–7.
Prüss-Üstün A, Bos R, Gore F, Bartram J. Safer water, better health: costs, benefits and sustainability of interventions to protect and promote health: World Health Organization; 2008. Available at https://apps.who.int/iris/bitstream/handle/10665/43840/9789241596435_eng.pdf;jsessionid=42B6FA8EA51E1FAE0FE6B292E79B0D4D?sequence=1. Accessed 8 Sept 2018.
Langford R, Lunn P, Brick CP. Hand-washing, subclinical infections, and growth: a longitudinal evaluation of an intervention in Nepali slums. Am J Hum Biol. 2011;23(5):621–9.
Spears D. How much international variation in child height can sanitation explain?: The World Bank; 2013. Available at https://rpds.princeton.edu/sites/rpds/files/media/spears_how_much_international_variation.pdf. Accessed 15 Sept 2018.
Rah JH, Cronin AA, Badgaiyan B, Aguayo VM, Coates S, Ahmed S. Household sanitation and personal hygiene practices are associated with child stunting in rural India: a cross-sectional analysis of surveys. BMJ Open. 2015;5(2):e005180.
Petri WA, Miller M, Binder HJ, Levine MM, Dillingham R, Guerrant RL. Enteric infections, diarrhea, and their impact on function and development. J Clin Invest. 2008;118(4):1277–90.
Mondal D, Minak J, Alam M, Liu Y, Dai J, Korpe P, et al. Contribution of enteric infection, altered intestinal barrier function, and maternal malnutrition to infant malnutrition in Bangladesh. Clin Infect Dis. 2011;54(2):185–92.
Guerrant RL, Schorling JB, McAuliffe JF, De Souza MA. Diarrhea as a cause and an effect of malnutrition: diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration. Am J Trop Med Hyg. 1992;47(1_Suppl):28–35.
Checkley W, Epstein LD, Gilman RH, Cabrera L, Black RE. Effects of acute diarrhea on linear growth in Peruvian children. Am J Epidemiol. 2003;157(2):166–75.
Checkley W, Buckley G, Gilman RH, Assis AM, Guerrant RL, Morris SS, et al. Multi-country analysis of the effects of diarrhoea on childhood stunting. Int J Epidemiol. 2008;37(4):816–30.
Kossmann J, Nestel P, Herrera M, El-Amin A, Fawzi W. Undernutrition and childhood infections: a prospective study of childhood infections in relation to growth in the Sudan. Acta Paediatr. 2000;89(9):1122–8.
Moore SR, Lima A, Conaway MR, Schorling J, Soares AM, Guerrant RL. Early childhood diarrhoea and helminthiases associate with long-term linear growth faltering. Int J Epidemiol. 2001;30(6):1457–64.
Korpe PS, Petri WA Jr. Environmental enteropathy: critical implications of a poorly understood condition. Trends Mol Med. 2012;18(6):328–36.
Humphrey JH. Child undernutrition, tropical enteropathy, toilets, and handwashing. Lancet. 2009;374(9694):1032–5.
Haghighi P, Wolf PL, Durie P. Tropical sprue and subclinical enteropathy: a vision for the nineties. Crit Rev Clin Lab Sci. 1997;34(4):313–41.
Lunn PG. The impact of infection and nutrition on gut function and growth in childhood. Proc Nutr Soc. 2000;59(1):147–54.
Prendergast A, Kelly P. Enteropathies in the developing world: neglected effects on global health. Am J Trop Med Hyg. 2012;86(5):756–63.
Cumming O, Cairncross S. Can water, sanitation and hygiene help eliminate stunting? Current evidence and policy implications. Matern Child Nutr. 2016;12:91–105.
Bowen A, Agboatwalla M, Luby S, Tobery T, Ayers T, Hoekstra R. Association between intensive handwashing promotion and child development in Karachi, Pakistan: a cluster randomized controlled trial. Arch Pediatr Adolesc Med. 2012;166(11):1037–44.
Clasen T, Boisson S, Routray P, Torondel B, Bell M, Cumming O, et al. Effectiveness of a rural sanitation programme on diarrhoea, soil-transmitted helminth infection, and child malnutrition in Odisha, India: a cluster-randomised trial. Lancet Glob Health. 2014;2(11):e645–e53.
Luby SP, Rahman M, Arnold BF, Unicomb L, Ashraf S, Winch PJ, et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Bangladesh: a cluster randomised controlled trial. Lancet Glob Health. 2018;6(3):e302–e15.
Muhoozi GK, Atukunda P, Diep LM, Mwadime R, Kaaya AN, Skaare AB, et al. Nutrition, hygiene, and stimulation education to improve growth, cognitive, language, and motor development among infants in Uganda: a cluster-randomized trial. Matern Child Nutr. 2018;14(2):e12527.
Patil SR, Arnold BF, Salvatore AL, Briceno B, Ganguly S, Colford JM Jr, et al. The effect of India's total sanitation campaign on defecation behaviors and child health in rural Madhya Pradesh: a cluster randomized controlled trial. PLoS Med. 2014;11(8):e1001709.
Fenn B, Bulti AT, Nduna T, Duffield A, Watson F. An evaluation of an operations research project to reduce childhood stunting in a food-insecure area in Ethiopia. Public Health Nutr. 2012;15(9):1746–54.
Marshak A, Young H, Radday A. Water, livestock, and malnutrition: Findings from an impact assessment of “community resilience to acute malnutrition” programming in the Dar Sila Region of Eastern Chad, 2012–2015. Feinstein International Center, Friedman School of Nutrition Science and Policy at Tufts University, Boston. 2016. Available at https://www.alnap.org/help-library/water-livestock-and-malnutrition-findings-from-an-impact-assessment-of-%E2%80%9Ccommunity. Accessed 15 Sept 2018.
Pickering AJ, Djebbari H, Lopez C, Coulibaly M, Alzua ML. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: a cluster-randomised controlled trial. Lancet Glob Health. 2015;3(11):e701–e11.
The Joanna Briggs Institute (JBI). The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews: Checklist for Randomized Controlled Trials. Available at http://joannabriggs.org/assets/docs/critical-appraisal-tools/JBI_RCTs_Appraisal_tool2017.pdf. Accessed 15 Sept 2018.
The Cochrane Collaboration’s tool for assessing riskof bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928 Available at https://www.bmj.com/content/bmj/343/bmj.d5928.full.pdf.
Dangour AD, Watson L, Cumming O, Boisson S, Che Y, Velleman Y, et al. Interventions to improve water quality and supply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database Syst Rev. 2013;(8, 8):CD009382.
Gera T, Shah D, Sachdev HS. Impact of water, sanitation and hygiene interventions on growth, non-diarrheal morbidity and mortality in children residing in low-and middle-income countries: a systematic review. Indian Pediatr. 2018;55:381–93.
Daniels DL, Cousens SN, Makoae LN, Feachem R. A study of the association between improved sanitation facilities and children's height in Lesotho. Eur J Clin Nutr. 1991;45(1):23–32.
Hammer J, Spears D. Village sanitation and children's human capital: evidence from a randomized experiment by the Maharashtra government: The World Bank; 2013. Available at http://riceinstitute.org/wordpress/wp-content/uploads/downloads/2013/02/Hammer-and-Spears-2013.pdf. Accessed 15 Sept 2018.
Mackinnon E, Ayah R, Taylor R, Owor M, Ssempebwa J, Olago lD, et al. 21st century research in urban WASH and health in sub-Saharan Africa: methods and outcomes in transition. 2018:1-22. Available at https://www.tandfonline.com/doi/pdf/10.1080/09603123.2018.1550193?needAccess=true. Accessed 15 Sept 2018.
Humphrey JH, Mbuya MN, Ntozini R, Moulton LH, Stoltzfus RJ, Tavengwa NV, et al. Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: a cluster-randomised trial. Lancet Glob Health. 2019;7(1):e132–e47.
Ravi S, Singh R. Nutrition in India: Targeting the First 1,000 Days of a Child's Life. POLICY BRIEF.2016. Available at https://www.brookings.edu/wp-content/uploads/2016/10/20161023_policybrief_2.pdf. Accessed 15 Sept 2018.
Lutter CK, Lutter R. Fetal and early childhood undernutrition, mortality, and lifelong health. Science. 2012;337(6101):1495–9.
World Health Organization (WHO). Preventing diarrhoea through better water, sanitation and hygiene: exposures and impacts in low-and middle-income countries: World Health Organization; 2014. Available at https://apps.who.int/iris/bitstream/handle/10665/150112/9789241564823_eng.pdf?sequence=1. Accessed 15 Sept 2018.
Bartram J, Cairncross S. Hygiene, sanitation, and water: forgotten foundations of health. PLoS Med. 2010;7(11):e1000367.
Acknowledgments
The authors would like to thank Dr. Mekuriaw Alemayehu, a faculty member of the University of Gondar for his participation throughout the review process.
List of articles included in the review
Aluza, 2015 (unpublished)
Alzua ML, Pickering AJ, Djebbari H, Lopez C, Cardenas JC, Lopera MA, et al. Impact Evaluation of Community-led Total Sanitation (CLTS) In Rural Mali. A final report from from a cluster randomized controlled trial (registration at clinicaltrials.gov NCT01900912), 2015. Available at http://www.cedlas-er.org/sites/default/files/cer_evaluation_files/mali-clts-impact-evaluation-2014.pdf. Accessed on 08 August 2018.
Arnold 2009 (published)
Arnold B, Arana B, Mäusezahl D, Hubbard A, Colford Jr JM. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. International Journal of Epidemiology. 2009;38(6):1651-61.
Arnold 2018 (Correspondence)
Arnold BF, Null C, Luby SP, Colford JM. Implications of WASH Benefits trials for water and sanitation. The lancet . Vol 6 June 2018. https://doi.org/10.1016/S2214-109X(18)30229-8
Bowen 2012 (Published)
Bowen A, Agboatwalla M, Luby S, Tobery T, Ayers T, Hoekstra R. Association between intensive handwashing promotion and child development in Karachi, Pakistan: a cluster randomized controlled trial. Archives of pediatrics & adolescent medicine. 2012;166(11):1037-44.
Clasen 2014 (Published)
Clasen T, Boisson S, Routray P, Torondel B, Bell M, Cumming O, et al. Effectiveness of a rural sanitation programme on diarrhoea, soil-transmitted helminth infection, and child malnutrition in Odisha, India: a cluster-randomised trial. The Lancet Global Health. 2014;2(11):e645-e53.
Langford 2011 (Published)
Langford R, Lunn P, Brick CP. Hand-washing, subclinical infections, and growth: A longitudinal evaluation of an intervention in Nepali slums. American Journal of Human Biology. 2011;23(5):621-9.
Marshak 2015 (Unpublished)
Anastasia Marshak, Helen Young, and Anne Radday. Water, Livestock, and Malnutrition: Findings from an Impact Assessment of “Community Resilience to Acute Malnutrition” Programming in the Dar Sila Region of Eastern Chad, 2012–2015. Feinstein International Center, 2016. Available at https://www.alnap.org/help-library/water-livestock-and-malnutrition-findings-from-an-impact-assessment-of-%E2%80%9Ccommunity. Accessed on 07 August 2018.
McGuigan 2011 (Published)
McGuigan KG, Samaiyar P, du Preez M, Conroy RM. High compliance randomized controlled field trial of solar disinfection of drinking water and its impact on childhood diarrhea in rural Cambodia. Environmental science & technology. 2011;45(18):7862-7.
Muhoozi 2018 (Published)
Muhoozi GK, Atukunda P, Diep LM, Mwadime R, Kaaya AN, Skaare AB, et al. Nutrition, hygiene, and stimulation education to improve growth, cognitive, language, and motor development among infants in Uganda: A cluster-randomized trial. Maternal & child nutrition. 2018;14(2):e12527.
Patil 2014 (Published)
Patil SR, Arnold BF, Salvatore AL, Briceno B, Ganguly S, Colford Jr JM, et al. The effect of India's total sanitation campaign on defecation behaviors and child health in rural Madhya Pradesh: a cluster randomized controlled trial. PLoS medicine. 2014;11(8):e1001709.
Pickering 2015 (Published)
Pickering AJ, Djebbari H, Lopez C, Coulibaly M, Alzua ML. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: a cluster-randomised controlled trial. The Lancet Global Health. 2015;3(11):e701-e11.
Shafique 2013 (Unpublished)
Shafique S. Prevention of linear growth faltering and reversal of stunting among low birth weight infants in rural Bangladesh: a 2x2 factorial cluster randomized trial. PhD dissertation, 2013. Available at https://tspace.library.utoronto.ca/bitstream/1807/68990/1/Shafique_Sohana_201311_PhD_thesis.pdf. Accessed on 07 August 2018.
Funding
The authors of this study didn’t receive funds from any funding institution.
Author information
Authors and Affiliations
Contributions
Both the authors actively participated during conception of the review, development of the protocol, review and synthesis of articles, and writing various parts of the report. ZG prepared the manuscript. Both the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for systematic reviews.
Consent for publication
This manuscript does not contain any individual person’s data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
JBI critical appraisal checklist for randomized controlled trials. (DOCX 31 kb)
Additional file 2:
Data extraction format. (DOCX 35 kb)
Additional file 3:
Criteria for judging risk of bias in the ‘Risk of bias’ assessment tool. (DOCX 59 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gizaw, Z., Worku, A. Effects of single and combined water, sanitation and hygiene (WASH) interventions on nutritional status of children: a systematic review and meta-analysis. Ital J Pediatr 45, 77 (2019). https://doi.org/10.1186/s13052-019-0666-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-019-0666-2