
Abstract
Background
This study aimed to evaluate the prevalence of tooth wear among preschool children in Jakarta, Indonesia, and examine the risk factors associated with its occurrence.
Methods
An epidemiological survey was conducted with a cross-sectional study design. The participants were recruited via cluster sampling. Tooth wear was clinically assessed by one examiner using the Basic Erosive Wear Examination (BEWE) criteria. The children’s caries experience was also recorded. The parents of the participating children completed a self-administered questionnaire to answer demographic questions about the children and gather information about the children’s diet and oral health behaviors as well as the parents’ dental health-related knowledge. The data were analyzed using the Chi-square test and binary logistic regression.
Results
A total of 752 five-year-old children were invited to participate, with 691 (92%) enrolling in the study. Tooth wear occurred in 23% (161/691, BEWE > 0) of the participants, in which 78% (125/161) had at least one moderate tooth wear status (BEWE = 2). The consumption of citrus drinks, fruit juice, and vitamin C supplement drinks, together with the child’s caries experience, the father’s education level, and the family’s socioeconomic status, were significantly associated with tooth wear.
Conclusions
The five-year-old preschool children in Jakarta had a relatively low prevalence of tooth wear. Those consuming more acidic drinks, those with a higher socioeconomic status, and those with an absence of caries experience had a higher risk of tooth wear.
Similar content being viewed by others


Background
Tooth wear is described as the irreversible loss of dental hard tissue due to the chemical influence of extrinsic acid (including acid from diet and medications) and intrinsic acid (including acid from gastroesophageal reflux and vomiting) without bacterial involvement [1, 2]. This leads to the loss of the chemically softened oral tissue by abrasive forces [3]. It is a multifactorial condition involving an interplay of various chemical, biological, and behavioral factors. The potential for tooth wear depends on chemical factors including pH, titratable acidity, mineral content, and the calcium-chelating properties of the dental tissue. Biological factors, such as saliva, acquired pellicle, tooth structure, and tooth position in relation to the soft tissues and the tongue, are correlated with the pathogenesis of tooth wear. Furthermore, behavioral factors, including eating and drinking habits, and excessive oral hygiene are predisposing factors for tooth wear [4].
The prevalence of tooth wear varies widely worldwide, suggesting the effect of the diverse diet habit among different countries or regions on tooth wear. An epidemiological survey performed in Greece reported that 98.4%, of preschool children presented with tooth wear [5]. Similarly, tooth wear was present in 75% of Australian preschool children [6]. Moreover, roughly half (45%) of preschool children in Germany had tooth wear [7]. These results improved among Asian children. Tooth wear was prevalent in 18% of five-year-old children in Hong Kong [8], while in China, the prevalence of tooth wear was reported in 15% of children in Shanghai and only 6% in Guangxi and Hubei [9, 10]. Although the prevalence of tooth wear was found to be relatively low in several Asian places compared to Western countries, limited information is available regarding the situation in Indonesia.
Primary tooth enamel is thinner and softer compared to that of permanent teeth, and morphological differences exist between primary and permanent teeth. Therefore, the process of tooth wear can be faster in primary teeth. Even short-term exposure to acids may lead to advanced lesions progressing to the dentine in primary teeth [2]. Tooth wear may lead to tooth sensitivity, altered occlusion, compromised aesthetics, and, in severe cases, pulp exposure [1]. Moreover, the presence of early tooth wear damage to primary teeth can compromise dentition for the child’s entire lifetime. Tooth wear in primary dentition is considered a predictor of the increased risk of tooth wear in permanent dentition [10].
The dental treatment of tooth wear can be complex, expensive, and challenging; thus, early diagnosis is important. An epidemiological examination of young children with the tooth wear-induced loss of tooth structure should be performed to monitor the prevalence and severity, and preventive measures should be planned and provided as early as possible. The World Health Organization recommends the reporting of preschool children’s oral health status starting at the age of five. However, data regarding the prevalence of tooth wear among five-year-old preschoolers in Indonesia are scarce. Therefore, the aims of the present study were to evaluate the prevalence of tooth wear in five-year-old preschoolers in Jakarta, Indonesia, and identify the risk factors for tooth wear in this patient population.
Methods
This study was conducted in Jakarta, Indonesia, between January and May 2017. The reporting of the present study is in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [11].
Sample size estimation and selection of children
No study has reported on the prevalence of tooth wear in deciduous teeth in Indonesia. The prevalence of tooth wear varies widely between countries. There is high heterogeneity between studies, which is influenced by methodological and diagnosis factors [12]. For the purposes of this study, we estimated that tooth wear occurs in 20% of the population. The margin of error for the estimate was set at 3%. With a two-sided 95% confidence interval (CI), the required sample size was 683 children. With an estimated response rate of 90%, a total of 758 children aged 5 years were invited to join this study. A cluster sampling method was used to recruit the participants. Jakarta has six districts. The number of kindergartens chosen in each district was based on the proportion of the population living in the district. The government provided a list of kindergartens, which were randomly selected by personal computer for each district for inclusion in the study. All five-year-old children attending the selected kindergartens were invited to take part in the study. Written informed consent was provided by the parents of the participating children.
Questionnaire survey
The parents or guardians of each child were asked to complete an onsite and self-administered questionnaire that was adapted from questions used in a previous study [13] (attached as Additional file 1). The questionnaire included demographic information (sex of the child, education level of the parents, and socioeconomic status of the family), information about the child’s oral health–related behaviors (intake frequency of soft drinks, citrus drinks, fruit juice, and vitamin C supplement drinks, as well as usage of chewing gum, tooth-brushing practices, and history of dental visits), information about the presence of digestive disorders in the child, and information about the parents’ dental knowledge. There were 21 multiple-choice questions regarding the causes and prevention of dental diseases in order to assess the parents’ dental knowledge. Each correct answer was allotted one point, and no score was given for an incorrect or “I don’t know” answer. Thus, the total dental knowledge score ranged from 0 to 21. Based on the total scores, the level of knowledge was then categorized into three groups using three equal intervals: low (0–7), moderate (8–14), and high (15–21).
Clinical examination
A trained and calibrated dentist performed all the clinical examinations using a ball-end Community Periodontal Index probe and a disposable dental mirror attached to an intraoral light-emitting diode light. Duplicate examinations were conducted in 10% of the children at each school visit. A kappa statistic was used to test intra-examiner reproducibility. Tooth wear status was evaluated using the Basic Erosive Wear Examination (BEWE) criteria [14], which were used to examine the buccal, lingual, and occlusal/incisal surfaces of all primary teeth. The severity of tooth wear was recorded at 4 levels: 1) score of 0 = no tooth wear; 2) score of 1 = initial loss of surface texture; 3) score of 2 = distinct defect with hard tissue loss of less than 50% of the surface area (often involving the dentin); and 4) score of 3 = hard tissue loss of greater than 50% of the surface area (often involving the dentin). The surface with the highest BEWE score in a sextant was recorded to represent the entire sextant. Because of its sensitivity and specificity, the BEWE does not affect the diagnosis of dental caries. In addition, after the BEWE examination was conducted, we used the Decayed, Missing, and Filled Teeth (DMF-T) index to evaluate the dental caries experience of the primary teeth, which was assessed according to the World Health Organization criteria [15].
Statistical analysis
Two investigators entered the data from the clinical examinations and questionnaires into an Excel spreadsheet. Data cleaning was performed before the analysis. A descriptive analysis was performed to establish the prevalence of tooth wear among the participants. The children were divided into two groups: those with tooth wear (BEWE score > 0) and those without tooth wear (BEWE score = 0). The relationships between the presence of tooth wear and all the independent variables (demographic information, the child’s oral health–related behaviors, the presence of a digestive disorder in the child, and the parents’ dental knowledge) were assessed using Chi-square analysis. Next, all the variables were evaluated using a logistic regression model to determine the risk factors for tooth wear in the participants. The variables that were not statistically significant were removed via backward stepwise regression. The final model only included statistically significant variables. The level of statistical significance for all the tests was set at 0.05.
Results
Overall, 752 children from 33 kindergartens were invited to participate in the study; of these, 61 children were excluded because they did not provide a complete consent form or questionnaire or did not receive an oral examination due to uncooperative behavior. Accordingly, 691 children (370 boys and 321 girls) were included in the present study (a 91% response rate). Among the participants, 195 were in East Jakarta, 61 were in Central Jakarta, 157 were in West Jakarta, 147 were in South Jakarta, 113 were in North Jakarta, and 18 were in the Thousand Islands. The kappa value for the evaluation of tooth wear was 0.94. The prevalence of DMF-T was 82.5%, with a mean index of 7.20 (SD = 5.94).
Tooth wear status
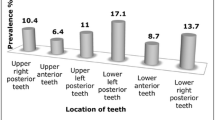
In total, 161 children (95 boys and 66 girls) were found to have at least one tooth wear lesion. In the present study, the prevalence of tooth wear was 23%, with a mean index of 0.29 (SD = 0.61). Among the children with tooth wear, the majority (78%) presented with a distinct defect consisting of hard tissue loss of less than 50% of the surface area (BEWE score = 2), while none of the children had severe tooth wear (BEWE score = 3) (Table 1). The mandibular anterior sextant showed the highest prevalence of tooth wear (19%), with a statistically significant difference compared to other sextants. This was followed by the maxillary anterior sextant (6%) (Table 2). Tooth wear was not prevalent in the posterior teeth of the young children.
Risk factors related to tooth wear
The results of the Chi-square test showed that the intake frequency of citrus drinks, fruit juice, and vitamin C supplement drinks, in addition to caries experience, were significantly related to the incidence of tooth wear (Table 3). The results of the logistic regression analysis are provided in Table 4. The final model obtained by backward stepwise binary regression was the same as that obtained from the forward stepwise procedure. The children with a higher intake frequency of citrus drinks (OR = 2.41, p < 0.001), fruit juice (OR = 2.01, p = 0.001), and vitamin C supplement drinks (OR = 2.21, p = 0.017) had a higher incidence of tooth wear. Moreover, the children from high socioeconomic backgrounds (OR = 1.66, p = 0.012) or with fathers with a lower education level had a high risk of tooth wear. In addition, the children with caries experience had a lower incidence of tooth wear (OR = 0.52, p = 0.004).
Discussion
Approximately 600 million people live in Southeast Asia, which comprises 9% of the world’s population. As the fourth most populated country in the world, Indonesia has the largest population in Southeast Asia [16]. Surprisingly, in spite of its large population, a search revealed that no epidemiological study has reported on the oral health status of five-year-old children in Indonesia [17]. The present study is the first oral health survey of Indonesian preschool children to report on the tooth wear status of primary teeth.
Various diagnostic criteria are readily available for the evaluation of tooth wear, including the BEWE criteria [14], the Smith and Knight tooth wear index [18], and the simplified scoring criteria for tooth wear index [19]. However, there is no consensus regarding a standardized instrument for use in epidemiological surveys. Introduced in 2007, the BEWE index is used to identify tooth wear at the patient level, and this has been adopted in epidemiological surveys worldwide [13, 17]. In the present study, we assessed tooth wear using the BEWE index because it is a validated and simple instrument that is less time-consuming, and more practical compared to other measures, especially when used in young children. In addition, the use of a widely adopted instrument allows our results to be compared with findings from other places, which increases the impact of the present study.
The survey results demonstrated a 23% prevalence of tooth wear in Jakarta preschool children, which was much lower than that of children from Western countries (98.4, 75, and 45.4% in Greece, Australia, and Germany, respectively [5,6,7]). However, the prevalence was slightly higher than that of Chinese preschoolers, which was reported by previous studies to be 14.9, 5.7, and 15.1% [8,9,10]. The prevalence of tooth wear in the anterior teeth was higher than in the posterior teeth, which is consistent with results from other studies [8, 20]. This may be because early eruption, together with the location of the anterior teeth, can result in a longer contact time between acidic drinks and the anterior teeth when compared with the posterior teeth.
In the studied population, the higher intake frequency of citrus drinks, fruit juice, and vitamin C supplement drinks was related to a higher likelihood of tooth wear, which is consistent with previous reports [21, 22] suggesting a dose–response relationship between the consumption of acidic drinks and tooth wear. One study reported that not only the intake frequency of acidic drinks but also the length of time taken to consume these drinks were risk factors for tooth wear [23], as the increased contact time between acidic beverages and teeth can result in a pronounced and prolonged drop in the pH value of the oral cavity. Some studies suggested that tooth wear was associated with drinking methods, a finding that is considered to be related to the contact time [24]. The drinking method was not a risk factor for tooth wear in the present study. However, only one question applied to the methods used for drinking, which may not have provided sufficient information to assess the contact time between acidic drinks and teeth. Follow-up questions regarding the details of the children’s drinking behaviors should be developed to collect more information.
This study identified a significant relationship between high socioeconomic status and the prevalence of tooth wear, in accordance with another study exhibiting similar results [20]. Although it has been debated whether families with a high socioeconomic status typically have healthier dietary habits, such habits increase their children’s chances of consuming more acidic drinks, such as the citrus drinks and fruit juice that we identified as risk factors for tooth wear in this study. Furthermore, the different dietary habits of various countries and regions should also be carefully considered, as diet can influence the occurrence of tooth wear [25]. Conversely, the children whose fathers had a lower education level had a higher risk of tooth wear. In Indonesia, the male is the dominant member of the family. Perhaps the fathers’ lower education level may have led to unhealthy dietary habits in the children with tooth wear; however, this connection was not straightforward, and the results conflicted with those reported by other studies [8, 20]. This cross-sectional study has limitations in that it may not be possible to find or verify causal relationships between various factors. It must be taken into consideration that tooth wear is a cumulative effect of multifactorial processes, which warrants the need for long-term future studies.
Some studies either did not identify a significant relationship between the incidence of tooth wear and dental caries [26] or found a simultaneous relationship [8]. In the present study, the children with dental caries had a lower risk of tooth wear. Our findings were similar to those of a previous study that observed an inverse relationship between the incidence of tooth wear and dental caries [27]. However, previous findings from published data are equivocal, with some studies reporting a statistically significant association between tooth wear and dental caries [28, 29], while others do not [30, 31]. Since the number of caries-free children was small in the present study, the results observed here should be interpreted with caution. More studies are, therefore, needed to clarify this association.
Our study has some limitations, which must be addressed. First, the study findings were restricted to children in Jakarta, random errors due to the cluster sampling may have occurred, and the results may not be generalized to all children in Indonesia. Future studies should be performed in other populations in Indonesia and also with different age groups, as conducted in other countries, to gain a better understanding of tooth wear [32]. A longitudinal study should be carried out in the future for better elucidation of the risk factors for tooth wear [33]. Second, it would have been ideal to provide a reexamination for duplicates after 1 week; however, this was not possible because the kindergartens refused a second visit.
Conversely, this study has several significant strengths. First, a large sample size (691 children) was used. Moreover, a high response rate (91%) was achieved by cluster sampling, and intra-examiner agreement was very high (0.94). Second, this study is the first report on tooth wear in Indonesian preschool children and helps to fill an information gap in the literature. This study identified a lower prevalence of tooth wear in Indonesian compared to European preschool children [5, 7]. However, the Indonesian children had a higher prevalence of tooth wear compared to those in other Asian countries [8,9,10]. Tooth wear correlated with the children’s dietary behaviors; therefore, educational programs designed to decrease the consumption of acidic drinks should be adopted. In addition, this study showed that children from high socioeconomic backgrounds demonstrated a higher risk of tooth wear. Hence, strategies or programs to treat tooth wear should be prioritized in such high-risk children. Furthermore there is evidence that in Indonesia there have been dietary changes in the direction of Western food preferences, which may lead to risks for tooth wear [34]. As the world’s fourth most populous country, the burden of such disease may cause significant negative impacts.
Conclusion
The prevalence of tooth wear in five-year-old Jakarta preschoolers was relatively low. The findings suggest that higher risk of tooth wear may be associated with the following elements: a higher intake of citrus drinks, fruit juice, and vitamin C supplement drinks; the father’s lower education level; a higher socioeconomic background; and absence of dental caries.
Availability of data and materials
The raw data is available from the authors for any author who wishes to collaborate with us.
Abbreviations
- BEWE:
-
Basic Erosive Wear Examination
- CI:
-
Confidence Interval
- OR:
-
Odds Ratio
References
Linnett V, Seow WK. Dental erosion in children: a literature review. Pediatr Dent. 2001;23:37–43.
Taji S, Seow WK. A literature review of dental erosion in children. Aust Dent J. 2010;55:358–67.
Carvalho TS, Lussi A, Jaeggi T, et al. Erosive tooth wear in children. Monogr Oral Sci. 2014;25:262–78.
Lussi A, Jaeggi T. Erosion-diagnosis and risk factors. Clin Oral Investig. 2008;12:5–13.
Gatou T, Mamai-Homata E. Tooth wear in the deciduous dentition of 5-7-year-old children: risk factors. Clin Oral Investig. 2012;16:923–33.
Taji SS, Seow WK, Townsend GC, et al. A controlled study of dental erosion in 2- to 4-year-old twins. Int J Paediatr Dent. 2010;20:400–9.
Tschammler C, Muller-Pflanz C, Attin T, et al. Prevalence and risk factors of erosive tooth wear in 3-6 year old German kindergarten children-a comparison between 2004/05 and 2014/15. J Dent. 2016;52:45–9.
Duangthip D, Chen KJ, Gao SS, et al. Erosive tooth wear among preschool children in Hong Kong. Int J Paediatr Dent. 2019;29:185–92.
Luo Y, Zeng XJ, Du MQ, et al. The prevalence of dental erosion in preschool children in China. J Dent. 2005;33:115–21.
Tao DY, Hao G, Lu HX, et al. Dental erosion among children aged 3-6 years and its associated indicators. J Public Health Dent. 2015;75:291–7.
Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–7.
Salas MM, Nascimento GG, Huysmans MC, Demarco FF. Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis. J Dent. 2015;43(1):42–50.
Zhang S, Chau AM, Lo EC, et al. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Health. 2014;14:7.
Bartlett D, Ganss C, Lussi A. Basic erosive wear examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008;12:S65–8.
World Health Organisation. Oral health surveys: basic methods. 5th ed. Geneva, Switzerland: World Health Organization; 2013.
Chongsuvivatwong V, Phua KH, Yap MT, et al. Health and health-care systems in Southeast Asia: diversity and transitions. Lancet. 2011;377:429–37.
Duangthip D, Gao SS, Lo ECM, et al. Early childhood caries among 5- to 6-year-old children in Southeast Asia. Int Dent J. 2017;67:98–106.
Smith BG, Knight JK. An index for measuring the wear of teeth. Br Dent J. 1984;156:435–8.
Bardsley PF, Taylor S, Milosevic A. Epidemiological studies of tooth wear and dental erosion in 14-year-old children in north West England. Part 1: the relationship with water fluoridation and social deprivation. Br Dent J. 2004;197:413–6.
Mantonanaki M, Koletsi-Kounari H, Mamai-Homata E, et al. Dental erosion prevalence and associated risk indicators among preschool children in Athens, Greece. Clin Oral Investig. 2013;17:585–93.
Al-Dlaigan YH, Al-Meedania LA, Anil S. The influence of frequently consumed beverages and snacks on dental erosion among preschool children in Saudi Arabia. Nutr J. 2017;16:80.
Okunseri C, Okunseri E, Gonzalez C, et al. Erosive tooth wear and consumption of beverages among children in the United States. Caries Res. 2011;45:130–5.
Sovik JB, Skudutyte-Rysstad R, Tveit AB, et al. Sour sweets and acidic beverage consumption are risk indicators for dental erosion. Caries Res. 2015;49:243–50.
Johansson AK, Lingstrom P, Imfeld T, et al. Influence of drinking method on tooth-surface pH in relation to dental erosion. Eur J Oral Sci. 2004;112:484–9.
Salas MM, Nascimento GG, Vargas-Ferreira F, Tarquinio SB, Huysmans MC, Demarco FF. Diet influenced tooth erosion prevalence in children and adolescents: results of a meta-analysis and meta-regression. J Dent. 2015;43(8):865–75.
Ab Halim N, Esa R, Chew HP. General and erosive tooth wear of 16-year-old adolescents in Kuantan, Malaysia: prevalence and association with dental caries. BMC Oral Health. 2018;18:11.
Honorio HM, Rios D, Santos CF, et al. Effects of erosive, cariogenic or combined erosive/cariogenic challenges on human enamel: an in situ/ex vivo study. Caries Res. 2008;42:454–9.
Alaraudanjoki V, Laitala ML, Tjäderhane L, Pesonen P, Lussi A, Anttonen V3. Association of erosive tooth wear and dental caries in Northern Finland Birth Cohort 1966 - an epidemiological cross-sectional study. BMC Oral Health. 2016. 4;17(1):6.
Mulic A, Tveit AB, Skaare AB. Prevalence and severity of dental erosive wear among a group of Norwegian 18-year-olds. Acta Odontol Scand. 2013;71(3–4):475–81.
Truin GJ, Van Rijkom HM, Mulder J, Van’t Hof MA. Caries trends 1996–2002 among 6- and 12-year-old children and erosive wear prevalence among 12-year-old children in the Hague. Caries Res. 2005;39:2–8.
Auad SM, Waterhouse PJ, Nunn JH, Moynihan PJ. Dental caries and its association with sociodemographics, erosion, and diet in schoolchildren from Southeast Brazil. Pediatr Dent. 2009;31:229–35.
Wei Z, Du Y, Zhang J, Tai B, Du M, Jiang H. Prevalence and indicators of tooth wear among Chinese adults. PLoS One. 2016. 1;11(9):e0162181.
Zhang J, Du Y, Wei Z, Tai B, Jiang H, Du M. The prevalence and risk indicators of tooth wear in 12- and 15-year-old adolescents in Central China. BMC Oral Health. 2015. 9;15(1):120.
Colozza D, Avendano M. Urbanisation, dietary change and traditional food practices in Indonesia: A longitudinal analysis. Soc Sci Med. 2019. 5;233:103–112.
Funding
This research was supported by grants from Universitas Indonesia. Financial support included for the data collection and presentation of results.
Author information
Authors and Affiliations
Contributions
DAM planned and assisted with the survey. AP contributed to the acquisition of data. FS and DAM supervised the study. CHC, SZ, and FS contributed to the conception of the study. SG, DAM, and AR contributed to the statistical analysis and data interpretation. CHC, SG, and DAM revised the manuscript critically for important intellectual content and contributed to the drafting and finalizing of the manuscript. AR dealt with local bureaucracy, obtained study permits, acted as a liaison to obtain ethical clearance, and supervised the study. All authors have approved the final version and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was obtained from the Ethics Review Board, Faculty of Dentistry, Universitas Indonesia (Protocol Number: 090670716). This research was conducted in full accordance with the World Medical Association Declaration of Helsinki. The principal investigator is responsible for ensuring the confidentiality of the study documents and protecting the anonymity of all respondents. All participants provided informed consent. Parental written consent was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Oral health questionnaire. (PDF 210 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Maharani, D.A., Pratiwi, A.N., Setiawati, F. et al. Tooth wear among five-year-old children in Jakarta, Indonesia. BMC Oral Health 19, 192 (2019). https://doi.org/10.1186/s12903-019-0883-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-019-0883-5