
Abstract
Introduction
Globally, eye diseases are considered as one of the major contributors of nonfatal disabling conditions. In Bangladesh, 1.5% of adults are blind and 21.6% have low vision. Therefore, this paper aimed to identify the community-based prevalence and associated risk factors of eye diseases among slum dwellers of Dhaka city.
Methods
The study was carried out in two phases. In the first phase, a survey was conducted using multistage cluster sampling among 1320 households of three purposively selected slums in Dhaka city. From each household, one family member (≥ 18 years old) was randomly interviewed by trained data collectors using a structured questionnaire. After that, each of the participants was requested to take part in the second phase of the study. Following the request, 432 participants out of 1320 participants came into the tertiary care hospitals where they were clinically assessed by ophthalmologist for presence of eye diseases. A number of descriptive and inferential statistics were performed using Stata 13.
Result
The majority of total 432 study participants were female (68.6%), married (82.6%) and Muslim (98.8%). Among them almost all (92.8%) were clinically diagnosed with eye disease. The most prevalent eye diseases were refractive error (63.2%), conjunctivitis (17.1%), visual impairment (16.4%) and cataract (7.2%). Refractive error was found significantly associated with older age, female gender and income generating work. Cataract was found negatively associated with the level of education, however, opposite relationship was found between cataract and visual impairment.
Conclusion
Our study provides epidemiologic data on the prevalence of eye diseases among adult population in low-income urban community of Dhaka city. The high prevalence of refractive error, allergic conjunctivitis, visual impairment, and cataract among this group of people suggests the importance of increasing access to eye care services.
Similar content being viewed by others

Background
Currently, eye diseases are considered as one of the major contributors of nonfatal disabling conditions in both high and low income countries [1]. The global burden of eye diseases was estimated to be 61.4 million DALYs, accounted for 4.0% of total DALYs [2]. Major contributors to the global burden of eye diseases are refractive errors (27.7 million DALYs), cataract (17.7 million DALYs), macular degeneration (9.3 million DALYs), glaucoma (4.7 million DALYs), trachoma (1.3 million DALYs), and vitamin A deficiency (0.6 million DALY) [2]. In addition, WHO estimated that globally 285 million people are visually impaired, of whom 39 million are blind [3]. The two main causes of visual impairment in the world are uncorrected refractive errors (42.0%) and cataract (33.0%) [4]. It is estimated that the South Asian region comprises a third of the world’s 45 million blind and the highest number of DALYs caused by eye diseases [5]. According to the National Blindness and Low Vision Survey of Bangladesh, 1.53% of adults, whose age is at least 30 years, are blind and 21.6% have low vision (presenting visual acuity of less than 6/12 in either one or both eyes) [6]. Cataract (73.4%) and refractive errors (18.9%) were found to be the main causes of visual impairment in Bangladesh [7]. Data from several studies suggest that insufficient food, substandard housing, and limited access to health care, education, water, and sanitation makes poor people more vulnerable to different diseases [8, 9]. Bangladesh Urban Health Survey (2013) reported that slum dwellers suffer from a poorer mental and physical health status than the rest of the population [10]. Therefore, it is imperative to ensure comprehensive eye care services at low or no cost for this vulnerable group of people.
In Bangladesh, few researches have been carried out on visual impairment and blindness, however, there is a paucity of investigations focusing on the prevalence and risk factors of common eye diseases among low-income population of Bangladesh. This paper unveiled the community based prevalence and associated risk factors of eye diseases among slum dwellers of Dhaka city. The findings of this study will provide strong insight to the policy makers and public health professionals about magnitude of different eye diseases, which, in turn will help them to design community-based programs to address the eye care needs of vulnerable slum population.
Methods
This study was carried out in two phases. In the first phase, a survey was conducted using multistage cluster sampling among 1320 households of three purposively selected slums in Dhaka city (Shabujbag slum, Mirpur slum and Mohammadpur slum). These slums were selected due to the presence of well-known tertiary eye care facility within the close proximity. The population size of the slums was taken into account while selecting 520 households from Shabujbag slum and 400 households from Mirpur and Mohammadpur slum each. Then from each household, one family member of at least 18 years age was randomly selected for the interview. Trained data collectors were assigned to collect socio-demographic and eye related information of the respondents using a structured questionnaire (Additional file 1). After that, each of the participants was requested to take part in the second phase of the study and their participation was voluntary. All of the 1320 household participants were given referral cards for free eye check up at any one of the three-selected tertiary eye care facilities (Ad-Din Women’s Medical College and Hospital, BNSB Dhaka Eye Hospital, VARD Eye Hospital). Finally, 432 out of the 1320 participants (33%) came into the tertiary care hospital for free eye examination. The participants were clinically examined by trained opthalmologists. The opthalmologists filled up a form that narrates the results of the clinical examination (Additional file 2).
Before the clinical examination trained data collectors conducted interview with the respondents using a structured questionnaire to cross check the socio-demographic information that was collected before.
Clinical examination
In this study eye diseases were diagnosed clinically by qualified medical professionals (ophthalmologists). All 432 participants who attended the tertiary eye care facilities were examined for the presence of eye diseases after obtaining informed written consent. The eye examination was systematically performed using guideline adopted from “The American Academy of Ophthalmology”, which included refraction test, examination of visual acuity, pupils, extra ocular motility and alignment, intraocular pressure, external examination, slit-lamp examination and fundoscopy [11].
For all eye diseases, we presented data for either eye. Refractive error was assessed using autorefractor and 6/6 vision was considered as emetropia. Participants were considered as having myopia or hypermetropia when spherical equivalent refractive error was less than − 0.50 diopters or more than + 0.50 diopters respectively. Data on visual acuity was reported as the presenting visual acuity obtained through presenting correction. The definitions for visual impairment, low vision and blindness used in this study follow those given in the international statistical classification of diseases, injuries and causes of death, 10th revision (ICD-10) [12] (Table 1).
Statistical analysis
Data was entered using CSPro version 6.0. After cleaning, data was transferred into Stata software (version 13.0 for Windows, 4905 Lakeway Drive, College Station, Texas 77,845 USA) for statistical analysis. Descriptive analysis was performed to estimate the prevalence of different eye diseases and was presented as frequency and percentage. Cross tabulation was performed to see the distribution of eye diseases among study participants across different age, gender, family income, educational level, occupation, and wealth index. Then these variables were tested for associations with different eye diseases in bivariate analysis using the Fisher’s exact test or Chi-square test as appropriate. Variables associated with different eye diseases in bivariate analysis were further tested in stepwise multivariable logistic regression model. A two-tailed P-value less than 0.05 was considered statistically significant.
Findings
Study population
A total of 432 respondents from three urban slums of Dhaka city participated in the study. The results, as shown in Table 2, indicate that the mean age of the study participants was 37.9 years (SD ± 13.30) and just over half of them were from 18 to 40 years of age (54.2%). Majority of the study participants were female (68.6%), married (82.6%) and almost all of them were Muslim (98.8%). On average, family income of our study participants was 13,270 BDT (SD: ± 8715) per month. Nearly half of them received no formal education (43.5%) and almost similar number of respondents were involved in income generating work (37.5%).
Prevalence of eye disease
Out of the 432 participants, 401 (92.8%) were diagnosed with any form of eye diseases. Among them, 237 (59.1%) participants had only one eye disease, 146 (36.4%) had two different eye diseases and 18 (4.5%) of the participants were diagnosed with three different types of eye illnesses. Refractive error, allergic conjunctivitis, visual impairment, and cataract were found as the most prevalent eye diseases in our study (Table 3).
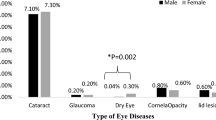
Refractive error had the highest prevalence among all eye illnesses with a frequency of 273 (63.2%) (Table 3). Of these 273 patients, the most prevalent refractive error was presbyopia 144 (33.3%), followed by hypermetropia 15 (3.5%) (Table 4). Conjunctivitis was found as the second most prevalent eye diseases among our study population with a frequency of 74 (17.1%). Among our respondents, 31 (7.2%) were diagnosed as having cataract. Moreover, a total of 71 (16.4%) subjects were classified as having visual impairment (presenting visual acuity< 6/18, including both low vision and blindness) in either eye of which 56 (13.0%) and 53 (12.3%) respondents were visually impaired in right and left eye respectively.
Risk factors
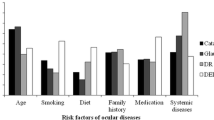
Table 5 presents the summary statistics for associations of different eye diseases (refractive error, visual impairment, and cataract) with socio-demographic variables (age, gender, education, occupation and family income). The prevalence of refractive error and cataract increased significantly with age at 5% level of significance. Subjects having more than 40 years of age were 3.02 times more likely to develop refractive error (p < 0.001) and 26.42 times more likely to develop cataract (p = 0.002). The prevalence of refractive error was also found to be influenced by gender and occupation of the study participants. The result of our study suggested that, at 5% level of significance, women were 2.92 times more likely to develop refractive error (p < 0.001) compared to men. People who were involved in income generating work also had significantly higher prevalence of refractive error (Adjusted OR = 1.70, 95% CI: 1.00–2.88, p = 0.048). The prevalence of cataract was observed to be associated with the study participants’ level of education. People having cataract were less likely to receive any formal education (Adjusted OR = 3.37, 95% CI: 1.28–8.89, p = 0.014). Nevertheless, cataract was found to have positive association with visual impairment (Adjusted OR = 7.33, 95% CI: 2.78–19.29, p < 0.001).
Discussion
To the best of our knowledge, this was the first reported study in Bangladesh providing data on the presence of clinically diagnosed eye diseases in low-income urban population of Dhaka, Bangladesh. The major findings of this study was detection of high prevalence of different eye diseases which would have been undiagnosed in absence of this active screening method.
Refractive error was found as the most prevalent eye disease among our study population (63.2%). This prevalence is higher than that found in the National Blindness and Low Vision Survey of Bangladesh (42.7%) (1999–2000) [7]. It is possible that prevalence of refractive error has increased in Bangladesh during this 14-years period of time as a result of possible cohort effect documented in other studies [13]. However, as there are ample inconsistencies in the methods used in these two studies, further investigation is necessary to decide whether the prevalence of refractive error is higher in low-income urban population than that in nationally representative sample and if so, to find out the potential reasons for such a high prevalence. Conjunctivitis was found as the second most prevalent eye diseases among our study population and most common type of conjunctivitis identified was allergic conjunctivitis (15.0%). Allergic conjunctivitis is one of the most common inflammatory disorders of anterior chamber of the eye, which has been considered the epidemics of the twenty-first century [14]. Comparison with the similar aged population was not possible due to the scarcity of international data, estimating the prevalence of ocular allergies within adult populations. However, our finding is similar to the prevalence of allergic rhino conjunctivitis (2.2–24.2% in children and 4.5–45.1% in adolescents) estimated by the International Study of Asthma and Allergies in Childhood (ISAAC). Phase III of this study involved 1, 93,404 schoolchildren aged 6–7 years from 37 countries and 3, 04,679 adolescents aged 13–14 years from 56 countries [15]. Unlike to refractive error, the prevalence of allergic conjunctivitis was considerably lower among our study population (15.0%) than that in other Asian countries (India, Japan, Thailand, and Singapore) where up to 30% of adults generally suffer from this disease [16].
The overall prevalence of cataract in our study participants was 7.2%. However, this prevalence was 15.2% among the respondents above 40 years of age. The prevalence of visual impairment in our study population (12.96%) was slightly higher than the estimated prevalence of visual impairment (VA < 6/18) in WHO South-East Asian Region (Bangladesh, Democratic Republic of Timor-Leste, Indonesia, Myanmar, Nepal, India excluded) which is 9.8% [17]. This difference could be due to the social, economic and political exclusion experienced by our study population. According to Baker, in 2007, only 7.3% of the slum dwellers in Dhaka city had access to public health care facilities [18]. This also might be due to the fact that, the programs developed and carried out by different organizations (NGOs, donors, government) are frequently unable to reach this underprivileged group of people living in the urban slums [19].
It is well evident that eye diseases impose a detrimental effect on the quality of life of affected individuals [20]. Uncorrected refractive error significantly reduces the self-reported visual ability as well as functional ability like mobility, driving, performing near vision tasks of an individual which ultimately affect his/her quality of life [21]. Patients with allergic conjunctivitis can experience significant impairment in their quality of life since moderate angina and the condition worsens during an acute episode for approximately 46% of the patients [22]. Visual impairment and age-related cataract have potential to act as independent risk factors for increased mortality in older persons [23]. Visual impairment alone also significantly reduce a person’s physical and mental well-being [24], though, the mental impact of visual impairment is much greater than its physical impact [25]. Individuals having visual impairment face difficulty to maintain mobility, suffer from depression and experience compromised self-ranking health status that is similar to a medical condition like stroke [23].
In this study, although we offered free checkup of eye diseases, the low number of participant turnout in the health facilities and a high number of untreated eye conditions indicate that eye health is not a priority in the low-income urban community in Bangladesh. Individuals living in urban slums are already burdened with a miserable set of circumstances along with lack of adequate knowledge about the origin of disease and appropriate measures for cure [26]. The situations further worsen as a result of their restricted access to societal assets like educational institutes, healthcare facilities, safe water source and basic sanitation [27]. Studies suggest an urgent need for health education and access to eye care services for these underprivileged slum populations to ameliorate this situation [28]. A study found that visually impaired persons who received support from friends and family members could adapt to vision loss more effectively, had less depressive symptoms, and higher life satisfaction [29]. Therefore, social support is also vital to improve the eye health status of this slum population.
As reported in other populations, increased age was positively associated with different eye diseases in our study like refractive error and cataract. It is evident that refractive index of the human eye lens is inhomogeneous [30] though the actual underlying principle for this opinion is yet a matter of debate. Refractive index distribution changes significantly with age, where main change is characterized by a decrease in the nuclear refractive index [31]. With increasing age, many types of modifications occur in the crystalline proteins of the human lens like protein denaturation and oxidation, which are responsible for age-related hardening and opacification of the lens nucleus and development of age-related cataract [32].
Our study shows a significantly higher prevalence of refractive error in women as compared to men which is similar to other studies [33]. The association of gender and refractive error has not been well established. This may be because women’s eyes have different axial length and anterior chamber depth than those of men and hence a higher probability of being affected by refractive error [34]. Environmental factor like close work and genetic factor also might be the reason for the divergence in axial length between men and women [35].
In our study cataract was significantly associated with the educational level of study participants. This finding is in accordance with previous studies like Framingham Eye Study [36] and lens opacities case-control study [37]. As well, in an age-adjusted analysis of a survey data carried out in India (Punjab), the prevalence of cataract was significantly higher in the group having no formal education [38]. Low education might have no apparent biological relation with cataract development. Confounding factors such as nutritional deficiency (Protein, vitamin A, niacin, thiamin and riboflavin deficiency) [39], UV-B exposure [40] and lifestyle related factors like smoking [41] might explain this association, therefore, further investigation needs to be carried out. Like previous research findings, cataract was found to be significantly associated with visual impairment in our study after adjusting for other potential confounders. This finding is also supported by data from prior studies that identified cataract as the most important causes of visual impairment globally [4] and in Bangladesh [6].
Previous studies show that awareness and knowledge of common eye diseases in developing countries are significantly less among the group of people having lack of formal education, low socioeconomic status and among female [42]. This means that increasing opportunity for better earning, basic education and raising awareness of eye diseases could lead to an improvement in understanding and acceptance of the importance of early detection and treatment of eye diseases. In this way, it is possible to lessen the cost of eye care, reduce the incidence of visual impairment and thus improve the quality of life.
The strength of this study was its standardized protocol and diagnosis of eye diseases by qualified ophthalmologists. However, the major limitation of our study was the low participation of the study population from household survey to tertiary eye care facilities. Another limitation of this study is potential over estimation of the clinically diagnosed eye diease prevalence due to the selection bias.
Conclusion
Our study provides epidemiologic data on the prevalence of clinically diagnosed eye diseases among the adult population in low-income urban community of Dhaka city. The high prevalence of refractive error, allergic conjunctivitis, cataract, and visual impairment suggests the importance of provision for eye care services to this group of people. In Bangladesh, ophthalmologists provide treatment for different eye illnesses at hospital settings, while BRAC and few other organizations provide eye care at community settings. Basic eye care including screening of the refractive errors can be implemented at the primary level by the community health workers at an affordable cost. There should also be community awareness program to promote the information on importance of early eye care to prevent long term consequences. Large population based longitudinal study is also needed to identify other behavioural, environmental and genetic risk factors that might be unique for Bangladeshi population.
Abbreviations
- BDT:
-
Bangladeshi Taka
- BNSB:
-
Bangladesh National Society for the Blind
- DALY:
-
Disability-Adjusted Life Year
- UV-B:
-
Ultra violet-B
- VARD:
-
Voluntary Association for Rural Development
- WHO:
-
World Health Organization
References
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. https://doi.org/10.1371/journal.pmed.0030442.
Ono K, Hiratsuka Y, Murakami A. Global inequality in eye health: country-level analysis from the global burden of disease study. Am J Public Health. 2010;100(9):1784–8. https://doi.org/10.2105/AJPH.2009.187930.
Morone P, Cuena EC, Kocur I, Banatvala N. Investing in eye health: securing the support of decision-makers. Geneva: World Health Organization; 2012. http://www.who.int/iris/handle/10665/258521
Resnikoff S, Pascolini D, Etya'Ale D, Kocur I, Pararajasegaram R, Pokharel GP, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844–5.
Pizzarello L, Abiose A, Ffytche T, Duerksen R, Thulasiraj R, Taylor H, et al. VISION 2020: the right to sight: a global initiative to eliminate avoidable blindness. Arch Ophthalmol. 2004;122(4):615–20.
Dineen BP, Bourne RRA, Ali SM, Huq DMN, Johnson GJ. Prevalence and causes of blindness and visual impairment in Bangladeshi adults: results of the National Blindness and low vision survey of Bangladesh. Br J Ophthalmol. 2003;87(7):820–8.
Bourne RRA, Dineen BP, Ali SM, Huq DMN, Johnson GJ. Prevalence of refractive error in Bangladeshi adults: results of the National Blindness and low vision survey of Bangladesh. Ophthalmology. 2004;111(6):1150–60.
Cattell V. Poor people, poor places, and poor health: the mediating role of social networks and social capital. Soc Sci Med. 2001;52(10):1501–16.
World Health Organization. Dying for change: poor people's experience of health and ill-health. Geneva: World Health Organization; 2001. http://documents.worldbank.org/curated/en/123521468332446432/pdf/331250ENGLISH0Dying0for0change.pdf
National Institute of Population Research and Training, International Centre for Diarrhoeal Disease Research B. MEASURE Evaluation. In: Bangladesh urban health survey 2013 final report; 2015. https://www.measureevaluation.org/resources/publications/tr-15-117.
American Academy of Ophthalmology. Guideline Summaries. Comprehensive Adult Medical Eye Evaluation. Retrieved from https://www.guidelinecentral.com/shop/comprehensive-adult-medical-eye-evaluation/
International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version for 2016. Retrieved from http://apps.who.int/classifications/icd10/browse/2016/en#/H54
Dayan YB, Levin A, Morad Y, Grotto I, Ben-David R, Goldberg A, et al. The changing prevalence of myopia in young adults: a 13-year series of population-based prevalence surveys. Invest Ophthalmol Vis Sci. 2005;46(8):2760–5.
Kubicka-Trzaska A, Romanowska-Dixon B. Dry eye syndrome and allergic conjunctivitis--epidemics of XXI century--diagnostic problems and management. Przegl Lek. 2009;66(11):967–71.
Rosario N, Bielory L. Epidemiology of allergic conjunctivitis. Curr Opin Allergy Clin Immunol. 2011;11(5):471–6. https://doi.org/10.1097/ACI.0b013e32834a9676.
Thong BY. Allergic conjunctivitis in Asia. Asia Pac Allergy. 2017;7(2):57–64. https://doi.org/10.5415/apallergy.2017.7.2.57.
Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–8. https://doi.org/10.1136/bjophthalmol-2011-300539.
Baker JL. Improving living conditions for the urban poor. Dhaka: the World Bank. Office. 2007; http://siteresources.worldbank.org/BANGLADESHEXTN/Resources/295759-1182963268987/dhakaurbanreport.pdf.
Agarwal S, Taneja S. All slums are not equal: child health conditions among the urban poor. Indian Pediatr. 2005;42(3):233–44.
Broman AT, Munoz B, Rodriguez J, Sanchez R, Quigley HA, Klein R, et al. The impact of visual impairment and eye disease on vision-related quality of life in a Mexican-American population: proyecto VER. Invest Ophthalmol Vis Sci. 2002;43(11):3393–8.
Zebardast N, Swenor BK, van Landingham SW, Massof RW, Munoz B, West SK, et al. Comparing the impact of refractive and nonrefractive vision loss on functioning and disability: the Salisbury eye evaluation. Ophthalmology. 2015;122(6):1102–10. https://doi.org/10.1016/j.ophtha.2015.02.024.
Palmares J, Delgado L, Cidade M, Quadrado MJ, Filipe HP. Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. Eur J Ophthalmol. 2010;20(2):257–64.
Wang JJ, Mitchell P, Simpson JM, Cumming RG, Smith W. Visual impairment, age-related cataract, and mortality. Arch Ophthalmol. 2001;119(8):1186–90.
Scott IU, Smiddy WE, Schiffman J, Feuer WJ, Pappas CJ. Quality of life of low-vision patients and the impact of low-vision services. Am J Ophthalmol. 1999;128(1):54–62.
Chia E-M, Wang JJ, Rochtchina E, Smith W, Cumming RR, Mitchell P. Impact of bilateral visual impairment on health-related quality of life: the Blue Mountains eye study. Invest Ophthalmol Vis Sci. 2004;45(1):71–6.
Hussain A, Ali SM, Kvåle G. Determinants of mortality among children in the urban slums of Dhaka city, Bangladesh. Tropical Med Int Health. 1999;4(11):758–64.
Rashid SF. Strategies to reduce exclusion among populations living in urban slum settlements in Bangladesh. J Health Popul Nutr. 2009;27(4):574.
Noertjojo K, Maberley D, Bassett K, Courtright P. Awareness of eye diseases and risk factors: identifying needs for health education and promotion in Canada. Can J Ophthalmol. 2006;41(5):617–23.
Cimarolli VR, Boerner K. Social support and well-being in adults who are visually impaired. J Vis Impair Blind. 2005;99(9):521.
Navarro R. The optical design of the human eye: a critical review. J Optom. 2009;2(1):3–18.
Moffat BA, Atchison DA, Pope JM. Age-related changes in refractive index distribution and power of the human lens as measured by magnetic resonance micro-imaging in vitro. Vis Res. 2002;42(13):1683–93.
Beebe DC, Holekamp NM, Shui Y-B. Oxidative damage and the prevention of age-related cataracts. Ophthalmic Res. 2010;44(3):155–65. https://doi.org/10.1159/000316481.
Zhao J, Pan X, Sui R, Munoz SR, Sperduto RD, Ellwein LB. Refractive error study in children: results from Shunyi District, China. Am J Ophthalmol. 2000;129(4):427–35.
Wong TY, Foster PJ, Ng TP, Tielsch JM, Johnson GJ, Seah SKL. Variations in ocular biometry in an adult Chinese population in Singapore: the Tanjong Pagar survey. J Vis Impair Blind. 2001;42(1):73–80.
Zhu G, Hewitt AW, Ruddle JB, Kearns LS, Brown SA, MacKinnon JR, et al. Genetic dissection of myopia: evidence for linkage of ocular axial length to chromosome 5q. Ophthalmology. 2008;115(6):1053–7. https://doi.org/10.1016/j.ophtha.2007.08.013.
Kahn HA, Leibowitz HM, Ganley JP, Kini MM, Colton T, Nickerson RS, et al. The Framingham eye study. II Association of ophthalmic pathology with single variables previously measured in the Framingham Heart Study. Am J Epidemiol. 1977;106(1):33–41.
Leske MC, Chylack LT, Wu S-Y. The Lens opacities case-control study. Risk factors for cataract. Arch Ophthalmol. 1991;109(2):244–51.
Chatterjee A, Milton RC, Thyle S. Prevalence and aetiology of cataract in Punjab. Br J Ophthalmol. 1982;66(1):35–42.
Cumming RG, Mitchell P, Smith W. Diet and cataract: the blue mountains eye study. Ophthalmology. 2000;107(3):450–6.
Cruickshanks KJ, Klein BE, Klein R. Ultraviolet light exposure and lens opacities: the beaver dam eye study. Am J Public Health. 1992;82(12):1658–62.
Christen WG, Manson JE, Seddon JM, Glynn RJ, Buring JE, Rosner B, et al. A prospective study of cigarette smoking and risk of cataract in men. JAMA. 1992;268(8):989–93.
Dandona R, Dandona L, John RK, McCarty CA, Rao GN. Awareness of eye diseases in an urban population in southern India. Bull World Health Organ. 2001;79(2):96–102.
Acknowledgements
The authors thank all the personnel of BRAC Health, Nutrition and Population Program (HNPP) for their incredible support in our field management, administrators and staff of Ad-Din Women’s Medical College and Hospital, BNSB Dhaka Eye Hospital and VARD Eye Hospitalfor allowing and supporting us to conduct this research and finally all respondents for sharing their time and experiences and the field researchers for collecting data often in difficult situations.
Funding
This study was funded by the Health, Nutrition and Population Programme, BRAC. This funding organization had no role in the design of the study, in data collection, analysis, and interpretation and in writing the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study will be available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
PG, TR and MS were involved in designing and executing the study. IS conducted data analysis and prepared the draft manuscript. MH and RDG critically reviewed the manuscript and provided intellectual feedback. MS guided the entire study and provided intellectual feedback on the manuscript. All the authors have gone through the final version of the manuscript and approved it for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the ethical review committee (ERC) of the BRAC James P. Grant School of public Health, BRAC University. Informed written consent was taken from the respondent’s prior each interview. The study purpose, risk, and benefits were explained to the respondents. Confidentiality and anonymity were ensured. Participation was voluntary and they could withdraw themselves at any time from the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they had no competing interests in preparing this manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Survey Questionnaire. This questionnaire was used to collect data on participants’ socio-demographic information, household related information, and eye care related information. (DOCX 128 kb)
Additional file 2:
Clinical examination form This form was used to collect data on participants’ eye examination result and clinical diagnosis of eye disease. (DOCX 1713 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sutradhar, I., Gayen, P., Hasan, M. et al. Eye diseases: the neglected health condition among urban slum population of Dhaka, Bangladesh. BMC Ophthalmol 19, 38 (2019). https://doi.org/10.1186/s12886-019-1043-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-019-1043-z