
Abstract
Background
Palliative medicine is assuming an increasingly important role in patient care. The Education for Physicians in End-of-life Care (EPEC) Project is an ambitious program to increase core palliative care skills for all physicians. It is not intended to transmit specialty level competencies in palliative care.
Method
The EPEC Curriculum was developed to be a comprehensive syllabus including trainer notes, multiple approaches to teaching the material, slides, and videos of clinical encounters to trigger discussion are provided. The content was developed through a combination of expert opinion, participant feedback and selected literature review. Content development was guided by the goal of teaching core competencies not included in the training of generalist and non-palliative medicine specialist physicians.
Results
Whole patient assessment forms the basis for good symptom control. Approaches to the medical management of pain, depression, anxiety, breathlessness (dyspnea), nausea/vomiting, constipation, fatigue/weakness and the symptoms common during the last hours of life are described.
Conclusion
While some physicians will have specialist palliative care services upon which to call, most in the world will need to provide the initial approaches to symptom control at the end-of-life.
Similar content being viewed by others

Background
A wide range of symptoms produce considerable suffering in patients at the end of their lives. This monograph aims to summarize the core competencies in symptom control needed by any physician, no matter his or her specialty. Many of the approaches will apply much earlier in the course of the illness, not just at the end of life.
The monograph does not purport to summarize specialist knowledge. While some practitioners will have specialist palliative care services upon which to call, most in the world will need to provide the initial approaches to symptom control at the end-of-life. This is not a fringe activity, but a core competency for physicians. After an overview of the approaches to whole patient assessment, we summarize the management of several of the more common symptoms that occur at the end-of-life.
However, to focus on symptom control skills alone will miss the mark. To be effective in end-of-life care, physicians must also have a broad conceptualization of end-of-life care and the legal issues that support it [1] and they must be competent in communication, decision-making and relation-building skills [2]. While we hope each pearl can improve a physician's practice, the complete Education for Physicians on End-of-life Care (EPEC) Curriculum should be mastered in order to be fully effective. [3]
Methods
To increase physician knowledge of new developments in palliation and their level of clinical competence in end-of-life care, the Institute for Ethics at the American Medical Association, with support from the Robert Wood Johnson Foundation, embarked on the Education for Physicians on End-of-life Care (EPEC) Project. The overall goal of the EPEC Project is to teach physicians how to provide better care to terminally ill patients. The overall method is to use a "train-the-trainer" dissemination model. The central hypothesis is that a core curriculum designed, written and taught by physicians using state of the art clinical knowledge and education theory, can be effective in reaching a second tier of physicians by having the newly trained physicians return to their work settings and seek to engage and educate a growing number of their peers using and adapting the provided educational materials. The project aims to improve end-of-life care through a ripple effect as the trainers educate a growing number of physicians.
A key tool of the EPEC Project was the development of the EPEC Curriculum. It sets out the core competencies that all physicians should have in palliative care. It was not intended to define or describe the specialty skills of a palliative medicine physician. Two Advisory Boards of 24 expert physicians in ethics, hospice, and palliative care initially recommended the curricular content and format. A team of experts with considerable clinical and research experience and expertise in physician education then developed the curriculum. Finally, it was modified based on the opinions of the first 280 physicians and other health care professionals trained to teach end-of-life care using the EPEC Curriculum (EPEC Trainers). The final EPEC Curriculum represents a synthesis of the ideas of many experts and clinicians. The information in the present manuscript is extracted from this curriculum
Results
Whole Patient Assessment
Management strategies to relieve suffering in end-of-life care begin with a comprehensive assessment of the whole patient, and his or her family. This approach to assessment may be quite distinct from familiar history taking and physical examination techniques. Whole patient assessment examines a range of issues that may cause suffering. It forms the basis for setting goals of care rather than seeking problem-based solutions. The assessment process itself can be a therapeutic tool. It acknowledges the patient as a person, and conveys compassion. [4–6]
During the assessment, ask about each of the possible symptoms and the patient's functional activities, rather than about organ systems or anatomy. Because symptoms are inherently subjective, patient self-report is the gold standard for assessment [7]. Validated symptom assessment tools may assist the clinician to gain consistent insight into the patient's perception of a symptom (eg, its severity, etc). When considering diagnostic tests, assess their potential to assist relief of suffering rather than diagnosis for its own sake.
Most people with an advanced life-threatening illness experience situational and possibly pathological changes in their affect and cognitive function, and a range of emotions and fears. Fear of loss of control and dignity, abandonment, being a burden, and physical suffering can be so strong that patients desire hastened death. Screening questions to assess for depression, anxiety and cognitive impairment, and inquiries about coping responses and fears, are all important since these issues can be redressed [8, 9].
While the physician may not have the skills of a social worker, he or she should be able to make an initial assessment of the patient's social and practical needs. Unresolved relationships or financial, legal, or practical matters may be sources of distress [10]. Because 30% of families spend their life savings and/or lose a source of income in order to care for the patient, it is important to know about financial status and health insurance coverage [11]. The need for practical help must be addressed; even the best of care plans may fail if the chores of day-to-day living are not attended to [12].
Every person has a spiritual dimension to his or her life. Whether it is understood in frankly religious terms, or in terms of personal meaning and the mystery of life, studies suggest that patients welcome inquiry about their spiritual issues [13, 14]. While a chaplain or skilled pastor usually administers spiritual care, the physician must consider the possibility that spiritual pain also manifests itself as physical, mental, or social distress.
Equipped with a full assessment of the nature and context of the issues that are causing suffering for the patient and family, the physician can then address each issue in turn. The following addresses some of the most common physical issues and some touches on some of the related family or social issues they raise.
Pain
Pain occurs frequently in end-of-life care. It can be acute or chronic [15].
Pain can be nociceptive or neuropathic in origin. The patient's description, physical findings, and the results of laboratory tests and imaging studies will usually be sufficient for a provisional diagnosis [16]. Nociceptive pain involves direct stimulation of intact mechanical, chemical, or thermal nociceptors, and transmission of electrical signals along normally functioning nerves. Patients may describe this as sharp, aching, and/or throbbing pain that is easily localized. Visceral nociceptive pain (eg, cardiac, lung, GI, GU) results from stimulation of the autonomic nervous system and may be difficult to describe or localize.
Neuropathic pain is presumed to result from disordered function of the peripheral or central nervous system due to any of many potential causes. Patients tend to describe neuropathic pain with words like burning, tingling, numbness, shooting, stabbing, or electric-like feelings.
Management
Effective pain management requires a clear understanding of the etiology and neuropathophysiology of each pain, and the pharmacology of analgesics. Nociceptive pain generally responds well to opioids and/or coanalgesics. Although neuropathic pain may respond well to opioids, adjuvant analgesics (tricyclic antidepressants, anticonvulsants, antiarrhythmics, etc) are often required in combination with opioids to achieve adequate relief.
Although research is not yet conclusive, unmanaged pain itself may lead to changes in the nervous system that could reduce its responsiveness to treatment. [17–19] Equally important, unrelieved pain can have a devastating psychological effect on the individual and family [20]. As there is no reason to delay the use of analgesics, [16] initiate analgesic interventions while completing investigations and providing therapies directed against the cause of the pain (eg, radiation for a neoplasm).
Placebos have no role to play in the assessment or management of pain outside of clinical trials [21]. Neither is there rationale for concerns that appropriate doses of analgesics will "mask" signs that will prevent accurate diagnosis and treatment [22–24].
Frequently, pharmacological and non-pharmacological interventions and an interdisciplinary plan that includes other health care professionals (nurses, social workers, pharmacists, chaplains, physiotherapists, occupational therapists, child life specialists, etc) are required to manage pain effectively. Plans must be tailored to the expectations and needs of each individual patient and family. Flexibility and ongoing education of the patient, family, and all caregivers, ongoing assessment of treatment outcomes, and regular review of the plan of care are all essential [15, 16]. When a plan does not control a patient's pain in a timely manner, ask for help from colleagues with more expertise.
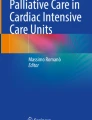
WHO 3-Step Model to Guide Analgesic Dosing
In 1986, the World Health Organization (WHO) developed a 3-step conceptual model to guide the management of cancer pain (see Figure 1) [25]. It provides a simple, well-tested model to guide the initial selection, administration, and titration of analgesics to manage the pain associated with any serious illness. When initiating or titrating analgesics, it is not necessary to traverse each step of the model sequentially; a patient with severe pain (7–10/10 on a numerical or visual analogue scale – NAS or VAS) may need to have step 3 opioids from the outset.

Figure 1
Step 1 Analgesics
Acetaminophen and the non-steroidal anti-inflammatory drugs (NSAIDs, including ASA) have an important role in symptom management. However, all have a ceiling effect to their analgesia (See table 1) [25]. All step 1 analgesics have a risk of adverse effects that are potentially life-threatening.
The mechanism of action of acetaminophen is still unknown (although it is known that it does not have a peripheral anti-inflammatory effect). Typically, it is used alone or combined with other analgesics (as a coanalgesic for additive or synergistic analgesic effects). Patients who may think more is better should be cautioned that toxicity can ensue at > 4 gm acetaminophen/24 hr, particularly in patients with hepatic compromise.
NSAIDs work, at least in part, by inhibiting cyclo-oxygenase, the enzyme that converts arachidonic acid to prostaglandins. They act directly at neuro-synaptic junctions and by reducing inflammation. They can be used alone, or as coanalgesics. Extended-release NSAIDs, or those with long half-lives (eg, piroxicam), are likely to enhance adherence. Intravenous formulations are also available (eg, ketorolac). Care must be taken to anticipate the potentially adverse effects of NSAIDs (eg, gastropathy, nephropathy and inhibition of platelet aggregation) that are independent of the route of administration. The newer agents specific to the isoenzyme cyclo-oxygenase 2 may have fewer adverse effects, but are less potent and more expensive than other possible choices. There is no reason not to start with the least expensive agent for a clinical trial before moving to more expensive agents.
Step 2 and 3 Analgesics
Step 2 and 3 analgesics include the pure agonist opioids, eg, codeine, fentanyl, hydrocodone, hydromorphone, morphine, and oxycodone. Those suggested for step 2 dosing combine a pure agonist opioid with either acetaminophen or aspirin to limit the amount of opioid that can be used [25].
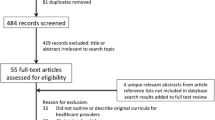
All of these opioids except fentanyl follow first-order kinetics. They reach their peak plasma concentration (Cmax) approximately 60 to 90 minutes after oral (including enteral feeding tube) or rectal administration, 30 minutes after subcutaneous or intramuscular injection, and 6 minutes after intravenous injection (see Figure 2). Dosed once every half-life, steady state plasma concentrations are achieved within 4–5 half-lives. Analgesia appears to track with plasma concentration. They are eliminated from the body at a fixed rate irrespective of the dose. The liver first conjugates them, then the kidney excretes 90% to 95% of the metabolites. Except for the demethylation of codeine (methylmorphine) to its active metabolite, their metabolic pathways do not become saturated.

Figure 2
Based on these pharmacological principles, if an immediate-acting oral opioid is selected and the pain is continuous, or nearly so, give the medication q 4h on a routine schedule (not "as needed"). The best possible pain control for the dose will be achieved within 24 hours, once steady state has been reached.
To control any extra or "breakthrough" pain, provide the patient with "as needed" rescue doses of the same immediate-acting opioid. Each rescue dose should be about 10–20% of the total 24 hour dose, offered q 1h prn PO or PR, q 30 min prn SC or IM, or q 10–15 min prn IV.
If pain remains uncontrolled after 24 hours, increase the routine dose by an amount at least equal to the total dose of rescue medication used during the previous 24 hours. If pain is mild or moderate, an increase of 25% to 50% in the total daily dose should be expected. If pain is severe or uncontrolled, an increase of 50% to 100% should be expected. In fact, if pain is severe and uncontrolled after 1 or 2 doses (eg, crescendo pain), do not wait for 24 hours to pass before increasing the routine dose. There is no maximum dose for a pure agonist opioid. Follow the patient closely and titrate the analgesics until the pain is relieved or adverse effects are encountered.
Increasingly, 12–24 hours sustained-release formulations of the opioids are becoming widely available for routine usage, either as tablets or granules. They must be ingested whole, not crushed or chewed. A fentanyl transdermal patch is also available that can deliver medication for up to 72 hours. Use of these preparations is likely to improve patient adherence. Extended-release formulations are not indicated for rescue dosing. For this purpose, use a concurrent dose of an immediate-release formulation of the same opioid.
Methadone, although the least expensive oral opioid, has a long and variable half-life (days). Only those with additional training should use it for pain control.
Not all opioid analgesics that are commonly available are recommended for acute or chronic dosing. Meperidine is poorly absorbed orally and has a short half-life of approximately 2–3 hours. Its principal metabolite, normeperidine, has no analgesic properties of its own, has a longer half-life of about 6 hours, is renally excreted, and produces significant adverse effects when it accumulates. Propoxyphene is typically administered at doses that produce relatively little analgesia. The mixed opioid agonist-antagonists such as pentazocine, butorphanol, nalbuphine, and dezocine are not recommended as routine analgesics. Their dosing is limited by a ceiling effect, and they have a high risk of adverse effects. They must not be used if the patient is already taking a pure agonist opioid, as competition for the opioid receptors may cause a withdrawal syndrome.
If patients have good pain control on stable doses of an opioid, and are not experiencing adverse effects (especially drowsiness), it is safe to drive a car. Patients in pain may have much poorer reaction times and may be a much greater risk.
If a patient is unable to ingest an oral analgesic an alternate route of administration or an alternate opioid may be preferable. Intramuscular injections are not recommended. Intermittent subcutaneous doses are just as effective, and much less painful.
When changing routes of administration or opioids, an equianalgesic table is a useful guide for initial dose selection. Significant first-pass metabolism necessitates larger oral or rectal doses to produce analgesia equivalent to parenteral doses of the same opioid. Equivalence dosing recommendations represent consensus from limited available evidence, so they are guides only. Individual patients may require doses to be adjusted by more than a factor of 2 to achieve effective analgesia without adverse effects (See Table 2) [26].
Opioids have common and uncommon adverse effects (Table 3). While several may be a problem initially, pharmacological tolerance typically develops to all of the adverse effects except constipation within days. Always caution patients and families to anticipate nausea and drowsiness for the first few days until tolerance develops. Provide antiemetics as needed. Prophylactic routine stimulant laxatives should be prescribed.
Many physicians misperceive that respiratory depression is a significant risk when prescribing opioids for pain. In fact, it is rare: pain is a potent stimulus to breath, somnolence always develops first, and pharmacological tolerance to respiratory depression develops quickly.
The cost of opioid analgesics varies considerably. Adequate analgesia can be achieved for the majority of patients with the least expensive opioids such as immediate-release preparations of morphine.
Addiction
It is a prevalent myth that the administration of opioid analgesics for pain management causes addiction [27]. Confusion about the differences between addiction, tolerance, and physical dependence is in part responsible.
The hallmark of opioid addiction is psychological dependence manifested by a behavioral syndrome of continued, compulsive drug use, despite harm [28]. Care must be taken to differentiate a true addiction (substance use disorder) from pseudo addiction due to under treatment of pain or other aberrant drug-related behaviors [29].
Pharmacological tolerance to analgesics (ie, the reduced effectiveness of a given dose of medication over time), is not evidence of addiction, [30] and is rarely significant clinically. After an initial titration period, doses may remain stable for long periods (months to years) if the pain stimulus remains unchanged. An increasing need for more analgesics more likely reflects progression of the symptom and underlying disease. On the other hand, tolerance to opioid adverse effects is commonly observed, and is favorable [31].
Physical dependence, evidenced by the development of a withdrawal syndrome when a medication is suddenly withdrawn, is not evidence of addition [30]. Similar outcomes occur in the presence of exogenous hormones and other medications that act through cellular receptors (eg, estrogens, beta-blockers, alpha-2 agonists, caffeine, etc.). Some patients will experience less pain, either spontaneously, or with changes in their underlying disease. If the pain stimulus decreases or disappears, opioid doses usually can be reduced in decrements of 50% or more every 2 to 3 days, and finally stopped without causing a withdrawal syndrome [32].
Depression
It is a myth that persistent feelings of helplessness and hopelessness are inevitable and permanent consequences of advanced life-threatening illness [33]. Most patients with a serious illness experience periods of intense situational sadness and anxiety accompanied by depressive symptoms. These feelings are usually present for a relatively short period (days to weeks), and then resolve. However, in a variable number of patients, these feelings persist.
The earlier depression is diagnosed, the more responsive to treatment it may be [34]. The most reliable symptoms of major depression in patients with advanced illness are persistent dysphoria, anhedonia, feelings of helplessness, hopelessness, and worthlessness, and loss of self-esteem [35]. The somatic symptoms of depression (such as changes in weight) are unreliable as they may reflect the underlying illness [36]. The screening question, "Do you feel depressed most of the time?" is a highly sensitive and specific question in this population [37]. Thoughts of suicide and requests to hasten death may be a marker of undiagnosed depression.
Treatment for depression may help patients feel better and have the energy and interest to achieve their final goals before they die. Approaches that combine supportive counseling and psychotherapy with antidepressant medication work best. Other members of the health care team can provide invaluable assistance to support the depressed patient, and his or her family.
When reversal of depression is an immediate short-term goal, a rapid-acting psychostimulant (such as methylphenidate) is the best choice [38]. If a response in 2 to 4 weeks is acceptable, an atypical antidepressant or selective serotonin reuptake inhibitor (SSRI) may be an appropriate choice [39]. Tricyclic antidepressants have limited usefulness due to their long time to achieve therapeutic levels and risk of anticholinergic adverse effects [40]. If the diagnosis is unclear, or the expected therapeutic response delayed, consult with a colleague with expertise.
Anxiety
Patients facing a life-threatening illness commonly experience anxiety over their fears and uncertainties about their future [41]. Compassionate exploration of the specific issues that are causing or exacerbating anxiety may be complex. Issues of grief and loss may be important contributors. Differentiate between primary anxiety and delirium, depression, bipolar disorder, and medication side effects. Look for insomnia and other reversible causes of anxiety due to alcohol, caffeine, or medications [42]. Input from family, friends and other members of the interdisciplinary team may be invaluable.
Like depression, the management of anxiety often requires a combination of supportive therapy and medications. Concerns about finances, family conflicts, future disability, dependency, and existential concerns will not resolve with medication. When it appears that pharmacological therapy will be beneficial, benzodiazepines are generally the medication class of choice [43]. Intermediate half-life agents (eg, lorazepam or clonazepam) are commonly used. Benzodiazepines may worsen short-term memory, particularly in the elderly, or cause confusion in patients with preexisting cognitive impairment. A few patients will experience a paradoxical reaction to benzodiazepines, and their anxiety will get worse. When discontinuing benzodiazepines, taper them slowly to prevent rebound anxiety.
Breathlessness (Dyspnea)
Breathlessness may be one of the most distressing symptoms for patients, families, and caregivers. Believing the patient's self report is the best way to assess it. Where possible, the underlying cause should be treated to at least provide symptomatic relief when the burden of the therapy does not outweigh the benefit.
There are 3 widely used medical approaches for the symptomatic relief of breathlessness: oxygen, opioids, and anxiolytics. Nonpharmacological interventions may also contribute significantly to the patient's and family's sense of well-being, and their ability to cope.
The majority of patients who report breathlessness are not hypoxemic. Measures of hypoxemia (eg, pulse oximetry, blood gas determination) do not correlate with the patient's self-report [44–47]. This is not to say that such measurements may not be useful in understanding pathophysiology. However, the measurements frequently do not correlate with symptom relief. In addition, such measurements may be uncomfortable, frightening and/or expensive, and divert the focus away from the symptom.
While oxygen will not reverse the cause of the breathlessness, a therapeutic trial of supplemental oxygen by nasal prongs may be beneficial. This may have a placebo effect [47]. In addition, its effectiveness may be explained by the observation that cool air moving across the patient's face (eg, from compressed air by nasal prongs, or from a fan) may provide equal relief due to the stimulation of the V2 branch of the fifth cranial nerve [48].
Opioids may provide significant relief of the sense of breathlessness without having a measurable impact on their respiratory rate or blood gas concentrations [49]. Through both central and peripheral effects, doses lower than those used to relieve pain may be effective in opioid naïve patients. In some patients, subjective relief may also be associated with a measurable increase in exercise tolerance and mobility [50, 51].
Concerns that opioid usage to manage symptoms will cause respiratory depression or hasten death (ie, an unintended effect), or cause addiction are not relevant. Opioid treatment for dyspnea is consistent with good medical practice, ethical when the intent is to relieve suffering, widely accepted when standard dosing guidelines are followed, and very unlikely to be associated with abuse behaviors [52]. As with pain treatment, pharmacological tolerance is not a clinically significant issue.
Some patients who are breathless and anxious may also need treatment for their anxiety. Benzodiazepine medications may be combined safely with opioids [53].
Nausea/Vomiting
A thorough assessment of the etiology and pathophysiology of nausea and vomiting is crucial as different causes will require very different interventions. Two organ systems – the gastric lining of the GI tract, and the area postrema (the chemoreceptor trigger zone), the vestibular apparatus, and the cortex of the brain are important contributors [54].
The neurotransmitters dopamine, histamine, acetylcholine, and serotonin are important mediators of this symptom complex. All four can be demonstrated in the area postrema. Although all are present in the lining of the GI tract, serotonin is particularly important. Acetylcholine and histamine are important in the vestibular apparatus. Nausea and vomiting that is mediated by the cortex is more complex and not associated with specific neurotransmitters (eg, the anticipatory nausea associated with chemotherapy).
Dopamine-mediated nausea is probably the most frequently targeted for initial symptom management, even when the precise mechanism of nausea is not known. Dopamine antagonist medications used to control nausea include the phenothiazines (eg, prochlorperazine) or butyrophenone neuroleptics (eg, haloperidol). Both have the potential to cause drowsiness and extrapyramidal symptoms, particularly in young women [55].
Commonly used antihistamines (eg, diphenhydramine, hydroxyzine) also have anticholinergic properties. They may do "double duty" as a single agent and cover both etiologies of nausea [56].
Opioids and anesthetics can trigger acetylcholine-mediated nausea in the vestibular apparatus. A pure anticholinergic medication may be added to other antiemetics in empirical therapy, particularly when the vestibular apparatus is implicated (eg scopolamine) [57].
Serotonin antagonists have been very effective in treating chemotherapy-associated nausea (eg, ondansetron) [58]. They have been reported to be useful for refractory nausea of diverse types but are typically tried only when other medications have failed. They are expensive and should be promptly stopped if they are not effective after a short therapeutic trial.
A "sluggish" or dyskinetic gut that does not empty properly (due to carcinomatosis, opioid therapy, other medications, diabetes mellitus etc.) may be a source of nausea and vomiting in patients with advanced disease [59]. Constipation, a large liver producing a "squashed stomach," ascites, or peritoneal disease may be causing pseudo-obstruction. Medications with prokinetic effects (eg, metoclopramide) or stimulant laxatives (eg, senna, bisacodyl) may be effective at moving gut contents forward, and relieving the associated nausea [60].
Hyperacidity, with or without gastroesophageal reflux and/or gastric or duodenal erosions, may produce nausea, heartburn, acidity, or bitter taste that may be associated with vomiting. Antacids, H2 receptor antagonists, or proton pump inhibitors may relieve the hyperacidity and/or reflux. Cytoprotective agents (eg, misoprostol) may be effective in treating the nausea associated with mucosal erosion secondary to NSAIDs.
Heterogeneous groups of medications that have unclear mechanisms of action, but uncontested benefits in some patients include glucocorticoids (eg, dexamethasone), cannabinoids (eg, tetrahydrocannabinol), and benzodiazepines (eg, lorazepam) [61–63].
With complete obstruction, accumulation of intraluminal fluid from epithelial sources is principally responsible for the symptoms of bloating, crampy abdominal pain, nausea, and vomiting. Octreotide, a synthetic analog of somatostatin, selectively inhibits secretion of fluids and electrolytes into the gut lumen and may relieve these symptoms [64–66].
Refractory cases of nausea and vomiting often require combinations of medications from different classes.
Constipation
Constipation is "the discomfort associated with reduced frequency of bowel movements" [67]. If left unmanaged, it can lead to abdominal pain, bloating, nausea and vomiting, overflow incontinence, tenesmus, fecal impaction, or even bowel obstruction.
As there is a wide range of "normal" in bowel habits, begin by assessing what the patient considers normal bowel function. Tailor examination, investigation, and treatment to the presentation, stage, and context of the person and illness. For most patients near the end of life, correction of the underlying pathophysiological cause of constipation is often not possible or appropriate. Constipation should be expected during opioid treatment and prophylactic measures always be initiated from the outset as the condition is easier to prevent than treat [68]. Opioids cause constipation, but they are not the only medication to do so. Other medications that may cause or exacerbate the problem are those with anticholinergic adverse effects (eg, tricyclic antidepressants) and calcium-channel blockers (eg verapamil).
As a general measure, have the patient toilet regularly at the same time each day. Take advantage of the gastrocolic reflex that occurs after eating – the strongest peristalsis occurs in the early morning [69].
Cathartic medications fall into several classes [70]. For patients with advanced illness, poor mobility, and decreased oral intake, a stimulant laxative (eg, prune juice, senna, casanthranol, or bisacodyl) is appropriate front-line therapy [71]. Osmotic laxatives (eg, magnesium salts, lactulose, sorbitol) may be added. Detergent laxatives (eg, docusate) at conventional doses are only stool softeners, and are rarely effective when used alone for patients at the end-of-life. Prokinetic agents (eg, metoclopramide) added to the regimen may assist the occasional patient whose constipation is refractory. A lubricant stimulant (eg, mineral oil) may assist a patient to defecate if the rectal vault is full. Large-volume enemas that work by distending the colon to induce peristalsis and soften are not well tolerated by debilitated patients.
A frequent mistake is the failure to dose-escalate a particular cathartic. This leads to the sense that "nothing works" when, in fact, nothing has been tried to its maximal therapeutic dose. Habituation in patients at the end-of-life is rarely an important clinical concern.
Fatigue/Weakness
Fatigue/weakness is the most frequent distressing symptom associated with advanced illness and end-of-life care. Patients and families frequently focus on the symptom rather than its underlying cause. Many believe that a person's strength is under his or her control, and feel that the patient is "giving up," "not fighting," or "not eating enough."
Physicians can play an instrumental role by educating patients and families about the nature of the symptom, and by giving the patient "permission" to rest. They can help decrease the pressure from family or others exhorting the patient to be more alert, energetic, and conversant. Assistance from other team members may be instrumental.
There are many general approaches to the management of fatigue [69]. Help patients and families to adapt activities of daily living to promote energy conservation. Physiotherapy and occupational therapy can help with assessment, teaching, and assistive devices. Discontinue routine medications that are no longer appropriate near the end of life that may be making the fatigue worse (eg, antihypertensives, cardiac medications, diuretics, etc.).
While fatigue/weakness is not easily treated pharmacologically, some patients respond to glucocorticoids (eg, dexamethasone) [70–72]. While they can be continued until death, the effect may wane after 4 to 6 weeks. As long-term adverse effects are not a factor for patients who are at the end of their lives, there is no need to taper the dose if it remains effective. The psychostimulants (eg, methylphenidate) may also be effective [73].
Symptom Management During The Last Hours Of Life
There are a variety of physiological changes that occur in the last hours and days of life. Each can be alarming if it is not understood. The most common are summarized here.
Weakness and Fatigue
Weakness and fatigue usually increase as the patient approaches death. The patients may become almost completely still, and this need not be resisted. Most treatment to alleviate it can be discontinued. Joints may become uncomfortable if they are not moved [77]. Continuous pressure on the same area of skin, particularly over bony prominences, will increase the risk of skin ischemia, and pain [78]. As the patient approaches death, provide adequate support and cushioning on the bed to lessen the need for uncomfortable turning.
Cessation of Intake
Most patients completely lose their appetite and stop drinking [79, 80]. This may heighten onlookers' distress. However, most experts feel that dehydration in the last hours of living does not cause distress and may stimulate the release of endorphins and anaesthetic compounds that promote the patient's sense of well being [81–83]. Low blood pressure or weak pulse is part of the dying process and not an indication of dehydration. Patients who are not able to be upright do not get light-headed or dizzy. Meticulous oral, nasal, and conjunctival hygiene help to allay concerns overt patient thirst [84].
Patients with peripheral edema or ascites have excess body water and salt and are not dehydrated, though their intravascular volume may be contracted due to hypoalbuminemia. Parenteral fluids, delivered either intravenously or subcutaneously by hypodermoclysis, are sometimes considered, particularly when the goal is to reverse delirium [85]. However, parenteral fluids may have adverse effects that are not commonly considered. Intravenous lines can be cumbersome and particularly uncomfortable when the patient is cachectic, or has no discernible veins. Excess parenteral fluids can lead to fluid overload with consequent peripheral or pulmonary edema, worsened breathlessness, cough, and orotracheobronchial secretions, particularly if there is significant hypoalbuminemia.
Loss of Ability to Swallow
Once the patient is unable to swallow, cease oral intake. Warn families and professional caregivers of the risk of aspiration. Scopolamine or glycopyrrolate will effectively reduce the production of saliva and other secretions [37, 38]. They will minimize or eliminate the gurgling from mucous buildup in the pharynx and trachea and may be used prophylactically in the unconscious dying patient. Anecdote suggests that the earlier treatment is initiated, the better it works, as larger amounts of secretions in the upper aerodigestive tract are more difficult to eliminate. However, premature use in the patient who is still alert may lead to unacceptable drying of oral and pharyngeal mucosa. While atropine may be equally effective, it has an increased risk of producing undesired cardiac and/or CNS excitation [86].
If excessive fluid accumulates in the back of the throat and upper airways, it may be cleared by repositioning or postural drainage. Oropharyngeal suctioning is likely to be ineffective as secretions are usually beyond the reach of the catheter. Continued efforts to suction may only stimulate an otherwise peaceful patient, and distress family members who are watching.
Neurological Changes
The neurological changes associated with the dying process are the result of multiple concurrent irreversible factors. These changes may manifest themselves in 2 different patterns that have been described as the "two roads to death" (See figure 3) [87]. Most patients follow the "usual road" that presents as decreasing level of consciousness and leads to coma and death.

Figure 3
Terminal Delirium
An agitated delirium may be the first sign to herald the "difficult road to death." These patients frequently present with confusion, restlessness, and/or agitation, with or without day-night reversal [88]. To the family and professional caregivers who do not understand it, agitated terminal delirium can be very distressing. Although previous care may have been excellent, if the delirium goes misdiagnosed or unmanaged, family members will likely remember a horrible death "in terrible pain" with cognitive impairment "because of the drugs."
It may be appropriate to evaluate and try to reverse treatable contributing factors. However, if the patient is in the last hours of his or her life with other concurrent signs of the dying process, the condition is by definition irreversible. Management appropriately focuses on the management of the symptoms associated with the terminal delirium in order to settle the patient and the family [89].
When moaning, groaning, and grimacing accompany the agitation and restlessness, they are frequently interpreted as physical pain (90). However, uncontrollable pain rarely develops or worsens during the last hours of life. Look for tension in the forehead, particularly for furrowing of the brow, as a clue that pain may be present.
While a trial of opioids may be beneficial in the unconscious patient who is difficult to assess, physicians must remember that opioids may accumulate and add to delirium when renal clearance is poor [91, 92]. If the trial of increased opioids does not relieve the agitation, or makes the delirium worse by increasing agitation or precipitating myoclonic jerks or seizures (rare), then pursue alternate therapies directed at suppressing the symptoms associated with delirium.
Benzodiazepines are used widely to treat terminal delirium as they are anxiolytics, amnestics, skeletal muscle relaxants, and antiepileptics [93]. Pre-dissolved oral lorazepam can be administered against the buccal mucosa and dose escalated to effect. Infusional benzodiazepines may be a rapidly effective alternative.
Benzodiazepines may paradoxically excite some patients [94]. These patients require neuroleptic medications to control their delirium. Haloperidol given intravenously, subcutaneously, or rectally may be effective [95]. A more sedating alternative is chlorpromazine given intravenously or rectally [96]. Barbiturates or propofol have been suggested as alternatives for the patient who is particularly difficult to control [97, 98].
Family Suffering Over Physiological Changes
Changes in breathing patterns are frequent and can be distressing to the onlooker. Warn family members and caregivers about the breathing patterns that they may observe.
Loss of sphincter control in the last hours of life may lead to incontinence of urine and/or stool. Cleaning and skin care are important. A urinary catheter may minimize the need for frequent changing and cleaning, prevent skin breakdown, and reduce the demand on caregivers. However, it is not always necessary if urine flow is minimal and can be managed with absorbent pads or surfaces. If diarrhea is considerable and relentless, a rectal tube may be similarly effective.
Eyes that remain open can be distressing to onlookers unless the condition is understood. Advanced wasting leads to loss of the retro-orbital fat pad, and the orbit falls posteriorly within the orbital socket [99]. As eyelids are of insufficient length to both extend the additional distance backward and cover the conjunctiva, they may not be able to fully appose. Maintain moisture by using ophthalmic lubricants, artificial tears, or physiological saline [100].
Conclusions
A host of physical symptoms are common in patients with advanced life-threatening illness. If assessed, many can be relieved. We have summarized the management of only a few. The interested physician will want to seek additional advice from some of the many sources of information available. Symptom control is an essential, but not a complete, part of the core competencies of physicians in end-of-life care [3].
References
Field MJ, Cassel CK, Eds: Approaching death: improving care at the end of life. Washington, DC: National Academy Press;. 1997
von Gunten CF, Ferris FD, Emanuel LL: Ensuring competency in end-of-life care: communication and relational skills. JAMA. 2000, 284 (23): 3051-3057. 10.1001/jama.284.23.3051.
Emanuel LL, von Gunten CF, Ferris FD, eds: The EPEC Curriculum: Education for Physicians on End-of-life Care. The EPEC Project. 2000, [http://www.EPEC.net]
Ingham JM, Portenoy RK: Symptom assessment. Hematology/Oncology Clinics of North America. 1996, 10 (1): 21-39.
Storey P, Knight CF: Unipac 3 assessment and treatment of pain in the terminally ill. Reston, VA: American Academy of Hospice and Palliative Medicine;. 1997, 7-18.
Vachon MLS: The emotional problems of the patient. In: Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks GWC, MacDonald N, eds. 1998, Oxford, England: Oxford University Press, 882-907. 2
Ingham J, Portenoy RK: The measurement of pain and other symptoms. In: Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks GWC, MacDonald N, eds. 1998, Oxford, England: Oxford University Press, 203-219. 2
Singer PA, Martin DK, Kelner M: Quality end-of-life care: patient's perspectives. JAMA. 1999, 281: 163-168. 10.1001/jama.281.2.163.
Vachon ML, Kristjanson L, Higginson I: Psychosocial issues in palliative care: the patient, the family, and the process and outcome of care. J Pain Symptom Management. 1995, 10: 142-150. 10.1016/0885-3924(94)00076-W.
Vachon ML: Psychosocial needs of patients and families. J Palliative Care. 1998, 14: 49-56.
Covinsky KE, Goldman L, Cook EF, Oye R, Desbiens N, Reding D, et al: The impact of serious illness on patients' families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994, 272: 1839-1844. 10.1001/jama.272.23.1839.
Emanuel EJ, Fairclough DL, Slutsman J, Alpert H, Baldwin D, Emanuel LL: Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999, 341: 956-63. 10.1056/NEJM199909233411306.
Storey P, Knight CF: Unipac 2: alleviating psychological and spiritual pain in the terminally ill. Reston, VA: American Academy of Hospice and Palliative Medicine. 1997, 23-28.
Ehman JW, Ott BB, Short TH, Ciampa RC, Hansen-Flaschen J: Do patients want physicians to inquire about their spiritual or religious beliefs if they become gravely ill?. Arch Intern Med. 1999, 159: 1803-1806. 10.1001/archinte.159.15.1803.
Bonica JJ: Definitions and taxonomy of pain. The Management of Pain. Edited by: JJ Bonica. 1990, Lea & Febiger, Philadelphia, 1: 18-20. 2
Portenoy RK: Cancer pain: pathophysiology and syndromes. Lancet. 1992, 339: 1026-1031. 10.1016/0140-6736(92)90545-E.
Zimmerman M, Herdegen T: Plasticity of the nervous system at the systematic, cellular, and molecular levels: a mechanism of chronic pain and hyperalgesia. Prog Brain Res. 1996, 110: 233-259.
Pockett S: Spinal chord synaptic plasticity and chronic pain. Anesth Analg. 1995, 80: 173-179.
McQuay HJ, Diskenson AH: Implications of nervous system plasticity for pain management. Anaesthesia. 1990, 45: 101-102.
Merskey H: Psychological medicine, pain, and musculoskeletal disorders. Rheum Dis Clin North Am. 1996, 22: 623-637.
McCaffery M, Ferrell BR, Pasero CL: When the physician prescribes a placebo. Am J Nurs. 1998, 98: 52-53.
Silen W: Cope's early diagnosis of the acute abdomen. Oxford University Press, New York. 1983, 5-7.
Wittman EH, Walker AP, Condon RE: Peritonitis and intraabdominal infection. In: Principles of Surgery. Edited by: Schwartz SI. 1994, McGraw-Hill, Inc. New York, 1476-6
Stern DH: Perioperative anesthesia. In: Surgery: a problem-solving approach. Edited by: Davis JH Sheldon GF. 1995, Mosby Chicago, 982-2
Jacox A, Carr DB, Payne R, et al: Management of cancer pain. Clinical practice guideline no. 9. AHCPR Publication No. 94-0592. Rockville, MD: Agency for Health Care Policy and Research, U.S. Department of Health and Human Services, Public Health Service,. 1994
Levy MH: Pharmacologic treatment of cancer pain. N Engl J Med. 1996, 335: 1124-1132. 10.1056/NEJM199610103351507.
Porter J, Jick H: Addiction rare in patients treated with narcotics. N Engl J Med. 1980, 302: 123.
Coyle N, Adelhardt J: Pain and addiction: an urgent need for change in nursing education. J Pain Symptom Management. 1992, 7: 439-440. 10.1016/0885-3924(92)90128-5.
Weissman DE, Haddox JD: Opioid pseudoaddiction – an iatrogenic syndrome. Pain. 1989, 36: 363-366. 10.1016/0304-3959(89)90097-3.
O'Brien CP: Drug addiction and drug abuse. In: Goodman & Gilman's The Pharmacological Basis of Therapeutics. Edited by: JG Hardman, LE Limbird. 1996, McGraw-Hill. New York, 559-560. 9
Portenoy RK: Tolerance to opioid analgesics: clinical aspects. Cancer Surv. 1994, 21: 49-65.
Portenoy RK, Frager G: Pain Management: Pharmacological approaches. In: Palliative Care and Rehabilitation of Cancer Patients. Edited by: CF von Gunten Kluwer. 1999, Academic Publishers. Boston, 1-29.
Breitbart W, Chochinov HM, Passik S: Psychiatric aspects of palliative care. In: Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks GWC, MacDonald N. 1998, Oxford, England: Oxford University Press;, 933-954. 2
Depression Guideline Panel. Depression in Primary Care: Detection, Diagnosis, and Treatment. Quick Reference Guide for Clinicians, Number 5. Rockville, MD: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; AHCPR publication No. 93-0552. April 1993
Breitbart W, Bruera E, Chochinov H, Lynch M: Neuropsychiatric syndromes and psychological symptoms in patients with advanced cancer. J Pain Symptom Management. 1995, 10: 131-141. 10.1016/0885-3924(94)00075-V.
McDaniel JS, Musselman DL, Porter MR, Reed DA, Nemeroff CB: Depression in patients with cancer. Diagnosis, biology, and treatment. Arch Gen Psychiatry. 1995, 52: 89-99.
Chochinov HM, Wilson KG, Enns M, Lander S: Are you depressed? Screening for depression in the terminally ill. Am J Psychiatry. 1997, 154: 674-676.
Woods SW, Tesar GE, Murray GB, Cassem NH: Psychostimulant treatment of depressive disorders secondary to medical illness. J Clin Psychiatry. 1986, 47: 12-15.
Salzman C: Practical considerations for the treatment of depression in elderly and very elderly long-term care patients. J Clin Psychiatry. 1999, 60 (Suppl 20): 30-3.
Evans DL, Staab J, Ward H, Leserman J, Perkins DO, Golden RN, et al: Depression in the medically ill: management considerations. Depress Anxiety. 1996, 4: 199-208. 10.1002/(SICI)1520-6394(1996)4:4<199::AID-DA6>3.3.CO;2-N.
Aass N, Fossa SD, Dahl AA, Moe TJ: Prevalence of anxiety and depression in cancer patients seen at the Norwegian Radium Hospital. Eur J Cancer. 1997, 33: 1597-1604. 10.1016/S0959-8049(97)00054-3.
Storey P, Knight CF: UNIPAC Four: Management of Selected Nonpain Symptoms in the Terminally Ill. Hospice/Palliative Care Training for Physicians: A Self-study Program. Gainesville, FL: American Academy of Hospice and Palliative Medicine;. 1996
Breitbart W, Jacobsen PB: Psychiatric symptom management in terminal care. Clin Geriatric Med. 1996, 12: 329-347.
Fainsinger R, miller MJ, Bruera E, Hanson J, Maceachern T: Symptom control during the last week of life on a palliative care unit. J Palliative Care. 1991, 7: 5-11.
Ripamonti C, Bruera E: Dyspnea: pathophysiology and assessment. J Pain Symptom Management. 1997, 13: 220-232. 10.1016/S0885-3924(96)00327-2.
Acheson A, MacCormack D: Dyspnea and the cancer patient – an overview. Cancer Oncol Nurs J. 1997, 7: 209-213.
Booth S, Kelly MJ, Cox NP, Adams L, Guz A: Does oxygen help dyspnea in patients with cancer?. Am J Respir Crit Care Med. 1996, 153: 1515-1518.
Shaiova LA: Management of dyspnea in patients with advanced cancer. Principles and Practice of Supportive Oncology Updates. 1999, 2 (3): 1-9.
Bruera E, MacEachern T, Ripamonti C, Hanson J: Subcutaneous morphine for dyspnea in cancer patients. Ann Intern Med. 1993, 119: 906-907.
Tobin M: Dyspnea: Pathphysiologic basis, clinical presentation, and management. Arch Intern Med. 1990, 150: 1604-1613. 10.1001/archinte.150.8.1604.
Light RW, Stansbury DW, Webster JS: Effect of 30 mg of morphine alone or with promethazine or prochlorperazine on the exercise capacity of patients with COPD. Chest. 1996, 109: 975-981.
Dudgeon D: Dyspnea: ethical concerns. J Palliative Care. 1994, 10: 48-51.
Ajemian I: Palliative management of dyspnea. J Palliative Care. 1991, 7: 44-45.
Mannix KA: Palliation of nausea and vomiting. In: Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks GWC, MacDonald N, eds. 1998, Oxford, England: Oxford University Press., 489-497. 2
Fallon BG: Nausea and vomiting unrelated to cancer treatment. In: Supportive Oncology. Edited by: Berger AM, Portenoy RK, Weissman DE. 1998, Lippincott-Raven. New York, 179-189.
Peggs JF, et al: Antihistamines: the old and the new. Am Fam Physician. 1995, 52: 593-600.
Clissold SP, et al: Transdermal hyscine (scopolamine). A preliminary review of its pharmacodynamic properties and therapeutic efficacy. Drugs:. 1985, 29: 189-207.
Pereira J, Bruera E: Successful management of intractable nausea with ondansetron: a case study. J Palliative Care. 1996, 12: 47-50.
Baines MJ: ABC of palliative care: nausea, vomiting, and intestinal obstruction. British Medical J. 1997, 315: 1148-1150.
Ripamonti C, Rodriguez C: Gastrointestinal motility disorders in patients with advanced cancer. In: Topics in Palliative Care Volume 1. Edited by: RK Portenoy and E Bruera. 1997, Oxford University Press, 61-93.
Twycross RB, Lack SA: Therapeutics in Terminal Cancer Churchill Livingstone. New York. 1990, 57-79.
Flynn J, Hanif N: Nabilone for the management of intractable nausea and vomiting in terminally staged AIDS. J Palliative Care. 1992, 8: 46-47.
Pisters KMW, Kris MG: Treatment-related nausea and vomiting. In: Principles and Practice of Supportive Oncology. 1998, Lippincott-Raven Press, 165-177.
Khoo D, Hall E, Motson R, Riley J, Denman K, Waxman J: Palliation of malignant intestinal obstruction using octreotide. Eur J Cancer. 1994, 30A: 28-30.
Mercadante S: Bowel obstruction in home-care cancer patients: 4 years experience. Support Care Cancer. 1995, 3: 190-193.
Mercandante S: Scopolamine butylbromide plus octreotide in unresponsive bowel obstruction. J Pain Symptom Management. 1998, 16: 278-280. 10.1016/S0885-3924(98)00101-8.
Fallon M, O'Neill B: ABC of palliative care. Constipation and diarrhoea. British Medical J. 1997, 315: 1293-1296.
Portenoy RK: Constipation in the cancer patient; causes and management. Med Clin North Am. 1987, 71: 303-311.
Sykes N: Pallaition of abdominal symptoms. In: Palliative Care and Rehabilitation of Cancer Patients. Kluwer Academic Publishers. New York. 1999, 43-57.
Derby S, Portenoy RK: Assessment and management of opioid-induced constipation. In: Topics in Palliative Care. Edited by: RK Portenoy and E Bruera. 1997, Oxford University Press. New York, 95-112.
Mercadante S: Diarrhea, malabsorption, and constipation. In: Principles and Practice of Supportive Oncology. 1998, Lippincott-Raven Press., 203-204.
Cella D, Peterman A, Passik S, Jacobsen P, Breitbart W: Progress toward guidelines for the management of fatigue. Oncology. 1998, 12: 369-377.
Miaskowski C, Portenoy RK: Update on the assessment and management of cancer-related fatigue. Principles & Practice of Supportive Oncology Updates. 1998, 1 (2): 1-10.
Bruera E, Roca E, Cedaro L, Carraro S, Chacon R: Action of oral methylprednisolone in terminal cancer patients: a prospective randomized double-blind study. Cancer Treat Rep. 1985, 69: 751-754.
Tannock I, Gospodarowicz M, Meakine W, et al: Treatment of metastatic prostatic cancer with low-dose prednisone: evaluation of pain and quality of life as pragmatic indices of response. J Clin Oncol. 1989, 7: 590-597.
Wilwerding MB, Loprinzi CL, Mailliard JA, Fallon O, Miser AW, van Haelst C, et al: A randomized, crossover evaluation of methylphenidate in cancer patients receiving strong narcotics. Support Care Cancer. 1995, 3: 135-138.
Fulton CL, Else R: Physiotherapy. In: Oxford Textbook of Palliative Medicine. Edited by: Doyle H, Hanks GWC, MacDonald N. 1998, Oxford University Press, Oxford, England, 821-2. 2
Walker P: The pathophysiology and management of pressure ulcers. In: Topics in Palliative Care, Volume 3. Edited by: Portenoy RK and Bruera E. 1998, Oxford University Press, New York, NY, 253-70.
Bruera E, Fainsinger RL: Clinical management of cachexia and anorexia. In: Oxford Textbook of Palliative Medicine. 1998, Oxford University Press, Oxford, England, 548-2
Billings JA: Comfort measures for the terminally ill: Is dehydration painful?. J Am Geriatr Soc. 1985, 33: 808-10.
Ellershaw JE, Sutcliffe JM, Saunders CM: Dehydration and the dying patient. J Pain Sympt Manage. 1995, 10: 192-7. 10.1016/0885-3924(94)00123-3.
Musgrave CF, Bartal N, Opstad J: The sensation of thirst in dying patients receiving IV hydration. J Pall Care. 1995, 11: 17-21.
Musgrave DR: Terminal dehydration: to give or not to give intravenous fluids?. Cancer Nursing. 1990, 13: 62-6.
Lethen W: Mouth and skin problems. In: The management of terminal malignant disease. Edited by: Saunders C and Sykes N. 1993, Edward Arnold, Boston, MA, 139-42. 3
Bruera E, Legris MA, Kuehn N, Miller MJ: Hypodermoclysis for the administration of fluids and narcotic analgesics in patients with advanced cancer. J Pain Sympt Manage. 1990, 5: 218-20. 10.1016/0885-3924(90)90014-B.
Twycross RB, Lack SA: Therapeutics in terminal cancer, Churchill Livingstone. 1990, 134-6. 3
Freemon FR: Delirium and organic psychosis. In: Organic Mental Disease. SP Medical and Scientific Books, Jamaica, NY. 1981, 81-94.
Ingham J, Breitbart W: Epidemiology and clinical features of delirium. In: Topics in Palliative Care, Volume 1. Edited by: Portenoy and Bruera E. 1997, Oxford University Press, New York, NY, 7-19.
Fainsinger RL, Tapper M, Bruera E: A perspective on the management of delirium in terminally ill patients on a palliative care unit. J Pall Care. 1993, 9: 4-8.
Shuster JL: Delirium, confusion, and agitation at the end of life. J Pall Med. 1998, 1: 177-86.
Zaw-tun N, Bruera E: Active metabolites of morphine. J Pall Care. 1992, 8: 48-50.
Maddocks I, Somogyi A, Abbot F, Hayball P, Parker D: Attenuation of morphine-induced delirium in palliative care by substitution with infusion of oxycodone. J Pain Sympt Manage. 1996, 12: 182-9. 10.1016/0885-3924(96)00050-4.
Twycross R, Lichter I: The terminal phase. In : Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks GWC, MacDonald N. 1998, Oxford University Press, Oxford, England, 987-8. 2
Feldman MD: Paradoxical effects of benzodiazepines. NC Med J. 1986, 47: 311-2.
Liu MC, Caraceni AT, Ingham JM: Altered mental status in patients with cancer: a delirium update. Principles & Practice of Supportive Oncology Updates. 1999, 2.
McIver B, Walsh D, Nelson K: The use of chlorpromazine for symptom control in dying cancer patients. J Pain Sympt Manage. 1994, 9: 341-5. 10.1016/0885-3924(94)90193-7.
Truog RD, Berde CB, Mitchell C, Grier HE: Barbiturates in the care of the terminally ill. N Engl J Med. 1992, 337: 1678-81.
Moyle J: The use of propofol in palliative medicine. J Pain Sympt Manage. 1995, 10: 643-6. 10.1016/0885-3924(95)00125-5.
Gray H: Anatomy of the human body. Edited by: Clemente CD. 1985, Lea & Febiger, Philadelphia, PA, 1303-13. 29
Smeltzer SC, Bare BG, Eds: Brunner and Suddarth's Textbook of Medical Surgical Nursing. 1992, J.B. Lippincott Company, Philadelphia, PA, 1657-1702. 7
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-684X/1/5/prepub
Acknowledgments
This work was initially supported by the American Medical Association and then Northwestern University with a generous grant from the Robert Wood Johnson Foundation. Thanks to the numerous experts who contributed to the EPEC Project (3). Thanks to EPEC Staff for their help in the project: Katie DiPrima, Damon Marquis, Jeanne Martinez, Kathryn Meshenberg, Nicholas Molodyko, Kathryn Rouse, Patrick Ryan, Shannon Smith, Rhonda Taira and Patricia Watson,.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing Interests
None declared
Authors' Contributions
LE conceived of the EPEC Program. FF, CvG and LE participated in the preparation of the current manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Ferris, F.D., von Gunten, C.F. & Emanuel, L.L. Ensuring competency in end-of-life care: controlling symptoms. BMC Palliat Care 1, 5 (2002). https://doi.org/10.1186/1472-684X-1-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-684X-1-5