
Abstract
Background
Brain-water content (BWC) decreases with maturation of the brain and potentially affects parameters of cerebral oxygenation determined by near-infrared spectroscopy (NIRS). Most commercially available devices do not take these maturational changes into account. The aim of this study was to determine the effect of different assumptions for BWC on parameters of cerebral oxygenation in preterm infants.
Methods
Concentrations of oxy-, deoxy- and total hemoglobin and regional cerebral oxygen saturation (rcStO2) were calculated based on absolute coefficients of absorption and scattering determined by multi-distance Frequency-Domain-NIRS assuming BWCs of 75-95%, which may be encountered in newborn infants depending on gestational and postnatal age.
Results
This range of BWC gave rise to a linear modification of the assessed NIRS parameters with a maximum change of 10%. This may result in an absolute overestimation of rcStO2 by (median (range)) 4 (1–8)%, if the calculation is based on the lowest BWC (75%) in an extremely preterm infant with an anticipated BWC of 95%.
Conclusion
Clinicians wishing to rely on parameters of cerebral oxygenation determined by NIRS should consider that maturational changes in BWC not taken into account by most devices may result in a deviation of cerebral oxygenation readings by up to 8% from the correct value.
Similar content being viewed by others

Background
Near-infrared spectroscopy (NIRS) is a tool to non-invasively evaluate tissue oxygenation in term and preterm infants. As reported previously [1–3], there are several instruments commercially available which use different techniques to measure tissue oxygenation, e.g. in the brain.
NIRS quantifies the interaction of near-infrared photons with biological tissue, which can be described by two different properties: the light absorption and the reduced scattering coefficient (μa and μs’). Since deoxy- and oxyhemoglobin (HHb, O2Hb) are the most relevant chromophores absorbing light of the near-infrared spectrum their concentrations can be calculated from μa. NIRS is able to determine μa by the diffusion approximation or changes in μa by the modified law of Lambert and Beer if the optical path length and geometrical properties are known. An important factor in these calculations is the brain water content (BWC) because water also absorbs near-infrared light, although to a lesser extent than O2Hb and HHb.
As far as the underlying algorithms for the determination of measures of tissue oxygenation are revealed at all, most NIRS devices do not allow adjustment for maturational changes in BWC and their underlying algorithms may assume BWCs as low as 75%.
Considering that due to physiological maturation BWC varies from 75% to 95% [4–6], one has to expect that this maturational change in BWC will have an effect on readings of cerebral oxygenation determined by NIRS, which might be therapeutically relevant in the clinical setting.
We aimed to quantify the impact of different assumptions for brain water content (75% for adults, 85% for term infants and 95% for very preterm infants [6]) in a series of measurements of cerebral oxygenation in preterm infants.
Methods
This prospective observational study was approved by the ethics committee of Tuebingen University Hospital and written informed parental consent was obtained in all infants.
Study population
A convenience sample of 17 preterm infants was studied in the neonatal intensive and high dependency care units of Tuebingen University Children’s Hospital. Patient characteristics are shown in Table 1. Only infants who were hemodynamically stable, i.e. who had normal blood pressure and normal skin colour and capillary refill time without cardiocirculatory support were included. Those with chromosomal or syndromal abnormalities were excluded.
NIRS-Measurements
All measurements were performed with the infant sleeping in a supine position with the head slightly elevated and turned to the contralateral side by less than 30°. The probe was positioned at the right temporo-parietal-region accurately in the middle between the tragus and the sagittal suture to avoid the sagittal sinus and the Sylvian fissure. Care was taken to comb any existing newborn hair apart before placing the optode. The optode was applied to the infants skull held by the hand of the examiner with gentle pressure.
For each measurement, a recording lasting at least 2 minutes was performed at a sampling rate of 1Hz.
NIRS-Device
We employed the ISS Oxiplex TS (ISS Inc., Champaign, IL, USA), a frequency-domain near infrared spectroscope. Each channel is equipped with 8 near-infrared light sources at two different wavelengths (four emitting at 692 nm and four at 834 nm) with emitter-detector distances of 1.5, 2, 2.5 and 3 cm, enabling a tissue penetration of 2–3 cm in depth according to the manufacturer’s specifications. To enable assessment of the path length as measured by a phase-shift, the light intensity is modulated with a frequency of 110 MHz.
Light intensity and phase shift are recorded for each emitter-optode distance using the proprietary software package OxiTS, and the absolute μa and μs’ are calculated based on the slope of the respective regression lines at each wavelength using the diffusion equation for homogeneous, semi-infinite media [1, 2]. Based on μa at two wavelengths, absolute concentrations of HHb and O2Hb and consequently also absolute values for total hemoglobin (tHb) and rcStO2 are calculated.
Calculation of hemoglobin concentrations and hemoglobin oxygen saturation for different water contents
Calculations of O2Hb, HHb, tHb and rcStO2 were performed using the equations given below and assuming BWCs of 95%, 85% and 75% [6].
Data analysis
For each 2-min measurement the median of HHb, O2Hb, tHb and rcStO2 was calculated three times, assuming BWCs of 75, 85 and 95%, respectively. Data are depicted as median (minimum – maximum) of the 17 individual medians for each parameter and each assumption for BWC.
Differences in NIRS-parameters brought about by the different assumptions for BWC were evaluated for normal distribution using a Shapiro-Wilk-test, showing non-normal distribution. Hence data were evaluated for statistical significance using the non-parametric sign-test. Analyses were performed using SPSS for Windows, Version 15.0 (SPSS Inc., Chicago, IL, USA).
Results
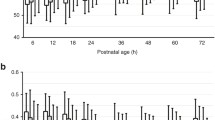
Different assumptions for BWC resulted in relevant changes in calculated concentrations of O2Hb and to a lesser extent of HHb. With the assumption of a higher BWC the computed concentration of O2Hb decreased and the computed concentration of HHb increased. Consequently, the tHb concentration and the rcStO2 decreased as shown in Figure 1. All comparisons between different assumptions for BWC yielded p-values < 0.0001 for all parameters evaluated. The computed values for O2Hb, HHb, tHb and rcStO2 at different BWC are shown in Table 2. Assuming BWC = 75% instead of BWC = 95% resulted in an overestimation of rcStO2 of 4 (1–8)%.In Figure 1 (A-D), oxygenated hemoglobin, deoxygenated hemoglobin, total hemoglobin and regional cerebral oxygen saturation are plotted against assumed BWCs.

(A-D): Calculated changes assuming different brain water contents. O2Hb (A), HHb (B), tHb (C) and rcStO2 (D) calculated assuming different brain water contents of 75, 85 and 95%, respectively.
Discussion
NIRS is increasingly used in neonatal intensive care. Instruments suitable and approved for continuous monitoring in this age group give readings on a measure of cerebral oxygenation based on several assumptions that may not hold true in a given infant – and hence displayed values of cerebral oxygenation may not be appropriate in certain individuals.
Our study addressed the question whether the assumption of different BWCs consistently influences O2Hb, HHb, tHb and rcStO2 readings in a realistic sample of clinically stable preterm infants using computations based on absolute coefficients μa and μs’ determined by multi-distance FD-NIRS and the diffusion equation for homogeneous, semi-infinite media.
A clinically relevant overestimation of “true” rcStO2 by up to 8% may result if BWC is incorrectly assumed to be only 75% in an extremely immature infant with a true BWC of 90-95%. This influence of different BWCs within the physiological range encountered in the neonatal intensive care unit on parameters of cerebral oxygenation is disregarded by most manufacturers of NIRS devices and also neglected by many clinicians who rely on readings of parameters of cerebral oxygenation for guiding cardiovascular therapy.
This systematic overestimation of rcStO2 by 4% (1%-8%), is probably not important in settings where rcStO2 trend monitoring is used e.g., during surgical interventions, and whenever relative changes of cerebral oxygenation in relation to a ‘normal’ baseline are observed to indicate cardiovascular interventions. Neonatal applications of cerebral oxygenation monitoring frequently lack a ‘normal baseline’ as rcStO2 monitoring is used in extremely preterm [7–9] and asphyxiated infants after resuscitation [10]. Furthermore, neonatal cerebral oxygenation monitoring is intended for days rather than just a few hours (e.g., [9]). As indicated in an European collaborative phase 2 trial of rcStO2-monitoring in extremely preterm infants, neonatologists are indeed interested in long-term continuous rcStO2 monitoring and, in the absence of a ‘normal baseline’, do rely on absolute rcStO2 readings [7]. Furthermore, suggested treatment algorithms indicate cardiovascular interventions if absolute cut-off values of rcStO2 are exceeded [8]. Whenever absolute readings of rcStO2 are relied upon for clinical decision making, a systematic over-/underestimation of rcStO2 may be of clinical importance.
For various reasons, including inhomogeneity of the tissue and issues of probe placement (underlying blood vessels, skin, background absorbers, different scattering properties, hair and texture, etc.), the signal-to-noise ratio is poorer and the limits of agreement after repeated repositioning of the NIRS-probe are greater in rcStO2-monitoring than in SaO2-monitoring using pulse oximetry (reviewed in [11]). Bland-Altman bias analyses revealing poor agreement with 95% limits of agreement of up to -17% to +17% have been reported previously [12]. More recently, using the ISS Oxiplex TS which was also used in this study, Arri et al. demonstrated that the test retest variability of rcStO2 measurements was approximately 5% for preterm infants [13], similar to test retest variability of 5% reported by Sorensen using the NIRO 300 [14]. Based on this more recent data, a systematic overestimation of rcStO2 by 4% (1%-8%) due to incorrect assumptions of BWC is considerable. Moreover, this systematic bias will add to the imprecision of the method and, in contrast to random factors, it is a systematic error that will not be overcome by averaging.
Our findings may also be of importance in the interpretation of longitudinal studies: Previously reported longitudinal data suggested that rcStO2 values decrease in preterm infants during the first 6 weeks of life despite stable cerebral blood flow index, which was interpreted as an increase in metabolic rate of oxygen [15]. In this study, rcStO2 was calculated based on the probably incorrect assumption of a constant BWC of 75% throughout the study period. The results of our simulation suggest that incorrect underestimation of BWC early on, may have contributed to the findings and that the postnatal decrease in rcStO2 and the increase in the metabolic rate of oxygen may have been overestimated.
It is obvious that smaller differences between assumed and actual BWC will result in smaller deviations of O2Hb, HHb, tHb, and rcStO2 from reality. In fact, depending on postmenstrual and postnatal age most BWC-values will range between 80% and 90% [6]. Furthermore, our data are only applicable to the wavelengths used herein. Different wavelengths with different ratios between the extinction coefficients for O2Hb, HHb and water will result in different degrees of deviation from reality if BWC is not taken into account. In general, the higher the extinction coefficient of water in relation to that of O2Hb or HHb at a given wavelength, the more relevant will be the impact of the difference between assumed and actual BWC.
Effects of different assumptions of BWC on rcStO2 readings of different devices will depend on the wave lengths used (as outlined above) and on the underlying algorithms for determination of rcStO2. In contrast to the instrument used for our study, unfortunately, many manufacturers of NIRS oximeters did not publish their algorithms and it is unknown how they deal with the water assumption.
We have previously described [16] that introducing a water term into equations describing the relation between the absorption coefficient, μa, and the slope of the decrease in light intensity using multi-distance FD-NIRS resulted in minor changes in StO2-measurements of the neonatal head if a constant BWC of 90% was assumed. However, this introduction of a water term resulted in large changes (absolute change in StO2 of up to 18% or relative change up to 30%) if the water content was assumed to be 70% in StO2-measurements on the adult arm. The present data complement our previous results, accounting for different assumptions for BWC in the range encountered between extremely preterm infants and early childhood. Those different assumptions for BWC will systematically bias results of HHb, O2Hb, tHb and StO2 measurements, overestimating StO2 if too low BWC is assumed. Although the median bias introduced by incorrect assumptions of BWC may be small (Table 2), in the occasional infant overestimation of StO2 may be clinically relevant.
Developmental changes in BWC should be considered in the clinical setting, especially in preterm infants, because a median difference in rcStO2 of 4% and a difference in rcStO2 of up to 8% in individual patients could change therapeutic decisions with potential long-term consequences.
Conclusion
Changing assumptions of BWC resulted in systematic modifications of computed O2Hb and HHb and in consecutive clinically relevant changes in rcStO2 of up to 8%. Disregarding maturational changes in BWC is another factor contributing to inadequate accuracy of absolute measures of cerebral oxygenation by standard NIRS devices. Neonatologists should be aware of the fact that rcStO2 will be overestimated by up to 8% if algorithms for calculating the measure of cerebral oxygenation are based on adult BWC.
Abbreviations
- FD-NIRS:
-
Frequency-Domain Near-Infrared Spectroscopy
- μa:
-
Absorption coefficient
- μs’:
-
Reduced scattering coefficient
- rcStO2:
-
Regional cerebral oxygen saturation
- HHb:
-
Deoxygenated hemoglobin
- O2Hb:
-
Oxygenated hemoglobin
- tHb:
-
Total hemoglobin
- BWC:
-
Brain water content.
References
Fantini S, Franceschini MA, Gratton E: Semi-infinite-geometry boundary-problem for light migration in highly scattering media - a frequency-domain study in the diffusion-approximation. J Opt Soc Am B. 1994, 11 (10): 2128-2138.
Fantini S, Hueber D, Franceschini MA, Gratton E, Rosenfeld W, Stubblefield PG, Maulik D, Stankovic MR: Non-invasive optical monitoring of the newborn piglet brain using continuous-wave and frequency-domain spectroscopy. Phys Med Biol. 1999, 44 (6): 1543-1563.
Greisen G, Leung T, Wolf M: Has the time come to use near-infrared spectroscopy as a routine clinical tool in preterm infants undergoing intensive care?. Philos Transact A Math Phys Eng Sci. 2011, 369 (1955): 4440-4451.
Wolf M, Greisen G: Advances in Near-Infrared Spectroscopy to study the brain of the preterm and term neonate. Clin Perinatol. 2009, 36: 807-834.
Wolf M, Naulaers G, van Bel F, Kleise S, Greisen G: A review of near infrared spectroscopy for term and preterm newborns. J Near Infrared Spectrosc. 2012, 20: 43-55.
Dobbing J, Sands J: Quantitative growth and development of human brain. J Arch Dis Child. 1973, 48 (10): 757-767.
Hyttel-Sorensen S, Austin T, van Bel F, Benders M, Claris O, Dempsey E, Fumagalli M, Greisen G, Grevstad B, Hagmann C, Hellström-Westas L, Lemmers P, Lindschou J, Naulaers G, van Oeveren W, Pellicer A, Pichler G, Roll C, Skoog M, Winkel P, Wolf M, Gluud C: A phase II randomized clinical trial on cerebral near-infrared spectroscopy plus a treatment guideline versus treatment as usual for extremely preterm infants during the first three days of life (SafeBoosC): study protocol for a randomized controlled trial. Trials. 2013, 14: 120-
Pellicer A, Greisen G, Benders M, Claris O, Dempsey E, Fumagalli M, Gluud C, Hagmann C, Hellström-Westas L, Hyttel-Sorensen S, Lemmers P, Naulaers G, Pichler G, Roll C, van Bel F, van Oeveren W, Skoog M, Wolf M, Austin T: The SafeBoosC phase II randomised clinical trial: a treatment guideline for targeted near-infrared-derived cerebral tissue oxygenation versus standard treatment in extremely preterm infants. Neonatology. 2013, 104 (3): 171-178.
van Bel F, Lemmers P, Naulaers G: Monitoring neonatal regional cerebral oxygen saturation in clinical practice: value and pitfalls. Neonatology. 2008, 94 (4): 237-244. Review
Dehaes M, Aggarwal A, Lin PY, Rosa Fortuno C, Fenoglio A, Roche-Labarbe N, Soul JS, Franceschini MA, Grant PE: Cerebral oxygen metabolism in neonatal hypoxic ischemic encephalopathy during and after therapeutic hypothermia. J Cereb Blood Flow Metab. 2014, 34 (1): 87-94.
Greisen G: Is near-infrared spectroscopy living up to its promises?. Semin Fetal Neonatal Med. 2006, 11 (6): 498-502. Review
Dullenkopf A, Kolarova A, Schulz G, Frey B, Baenziger O, Weiss M: Reproducibility of cerebral oxygenation measurement in neonates and infants in the clinical setting using the NIRO 300 oximeter. Pediatr Crit Care Med. 2005, 6 (3): 344-347.
Roche-Labarbe N, Carp SA, Surova A, Patel M, Boas DA, Grant PE, Franceschini MA: Noninvasive optical measures of CBV, StO(2), CBF index, and rCMRO(2) in human premature neonates’ brains in the first six weeks of life. Hum Brain Mapp. 2010, 31 (3): 341-352.
Arri SJ, Muehlemann T, Biallas M, Bucher HU, Wolf M: Precision of cerebral oxygenation and hemoglobin concentration measurements in neonates measured by near-infrared spectroscopy. J Biomed Opt. 2011, 16 (4): 047005-
Sorensen LC, Greisen G: Precision of measurement of cerebral tissue oxygenation index using near-infrared spectroscopy in preterm neonates. J Biomed Opt. 2006, 11 (5): 054005-
Metz AJ, Biallas M, Jenny C, Muehlemann T, Wolf M: The effect of basic assumptions on the tissue oxygen saturation value of near infrared spectroscopy. Adv Exp Med Biol. 2013, 765: 169-175.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2431/14/206/prepub
Acknowledgements
We would like to thank the infants and their families for participating in this research project. This study was supported by AKF-Grant E.03.27025.1 from the Faculty of Medicine Tuebingen, Germany. The funding agent did not have any involvement in (1) the study design; (2) the collection, analysis, and interpretation of data; (3) the writing of the report; and (4) the decision to submit the paper for publication. We acknowledge the support by the Deutsche Forschungsgemeinschaft and the Open Access Publishing Fund of Tuebingen University granting the publication fee. The authors greatly acknowledge Dr. Christoph Schwarz for the support in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AD designed the study and performed all NIRS-measurements, ran the data collection, performed the analysis and drafted the initial manuscript and revised the manuscript; MW advised NIRS aspects of the study and provided important advice for the calculations, reviewed and revised the manuscript making important intellectual contributions; CFP supervised the project as the head of department and reviewed and revised the manuscript making important intellectual contributions; ARF was co-coordinator of the project, supervised data analyses and reviewed and revised the manuscript making important intellectual contributions. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Demel, A., Wolf, M., Poets, C.F. et al. Effect of different assumptions for brain water content on absolute measures of cerebral oxygenation determined by frequency-domain near-infrared spectroscopy in preterm infants: an observational study. BMC Pediatr 14, 206 (2014). https://doi.org/10.1186/1471-2431-14-206
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2431-14-206