
Abstract
Background
The association between the TERT rs2736100 single nucleotide polymorphism (SNP) and cancer risk has been studied by many researchers, but the results remain inconclusive. To further explore this association, we performed a meta-analysis.
Methods
A computerized search of PubMed and Embase database for publications on the TERT rs2736100 polymorphism and cancer risk was performed and the genotype data were analyzed in a meta-analysis. Odds ratios (ORs) with 95% confidence intervals (CIs) were estimated to assess the association. Sensitivity analysis, test of heterogeneity, cumulative meta-analysis and assessment of bias were performed in our meta-analysis.
Results
A significant association between the TERT rs2736100 polymorphism and cancer susceptibility was revealed by the results of the meta-analysis of the 25 case-control studies (GG versus TT: OR = 1.72, 95% CI: 1.58, 1.88; GT versus TT: OR = 1.38, 95% CI: 1.29, 1.47; dominant model-TG + GG versus TT: OR = 1.47, 95% CI: 1.37, 1.58; recessive model-GG versus TT + TG: OR = 1.37, 95% CI 1.31, 1.43; additive model-2GG + TG versus 2TT + TG: OR = 1.30, 95% CI: 1.25, 1.36). Moreover, increased cancer risk in all genetic models was found after stratification of the SNP data by cancer type, ethnicity and source of controls.
Conclusions
In all genetic models, the association between the TERT rs2736100 polymorphism and cancer risk was significant. This meta-analysis suggests that the TERT rs2736100 polymorphism may be a risk factor for cancer. Further functional studies between this polymorphism and cancer risk are warranted.
Similar content being viewed by others


Background
Cancer is a multifactorial disease, which is the result of complex interactions between inherited and environmental factors. Lung cancer is the most common malignancy and the leading cause of cancer deaths for women and men worldwide [1–3]. There are two main histologic subgroups of lung cancer: small-cell lung carcinoma (SCLC) and non-small-cell lung carcinoma (NSCLC); the latter includes the common types, which are squamous cell carcinoma (SCC) and adenocarcinoma (ADC). Gliomas of astrocytic, oligodendroglial, and ependymal origin are derived from glial cells and account for Fax~80% of malignant primary brain tumors (PBTs), which are the most common histologic type of brain tumors [4]. There is a dose-response relationship between ionizing radiation and the risk of developing an intracranial tumor [5], whereas familial aggregation of gliomas [6] is a result of a combination of low-risk variants.
Telomeres are special nucleoprotein structures located at the ends of eukaryotic chromosomes and are essential for protecting chromosomal termini against degradation, end to-end fusion and rearrangement [7]. Telomeres are composed of repetitive DNA (TTAGGG repeats) bound to abundant specialized proteins. The length of telomere repeats as well as the integrity of telomere-binding proteins are essential for telomere maintenance [8]. Telomerase recognizes the 3' hydroxyl (3' OH) at the end of the G-strand overhang and adds telomeric repeat sequences onto chromosome ends. Telomerase expression can prevent telomere erosion in most eukaryotic organisms. Functional telomerase is composed of the TERT (telomerase reverse transcriptase) protein and the telomerase RNA component (TERC) that acts as a template for DNA synthesis. In contrast to TERC, which is expressed rather ubiquitously, TERT expression is low in most normal human somatic tissues and is physiologically restricted to primary germ line cells, tissue stem cells and activated lymphocytes [9–14], leading researchers to consider TERT as the limiting factor for telomerase activity. The TERT gene product contains three distinct structural domains: the RNA-binding domain (TRBD), the reverse transcriptase domain and the carboxy-terminal extension (CTE), which represents the putative thumb domain of TERT [15]. Tumor cells can prevent telomere loss through the abnormal upregulation of telomerase [16], and telomerase has been found to be reactivated in the majority of cancers, including those of the lung [7]. Activation of telomerase induced by the catalytic component TERT is a pivotal step during cellular immortalization and malignant transformation of human cells [17].
In the past decade, many investigators have explored factors contributing to inherited susceptibility to cancer [18]. The sequence variants in the TERT and cleft lip and palate transmembrane 1 like (CLPTM1L) gene regions are associated with susceptibility to many types of cancer [19]. The rs2736100 polymorphism is localized to intron 2 of the TERT gene. McKay et al. [20] published the first study indicating that the TERT rs2736100 polymorphism may contribute to an increased risk of lung cancer. Since then, several research groups have reported associations between this SNP and cancer risk, but with inconclusive results [21–31]. Consequently, we performed a meta-analysis to more precisely characterize this association.
Methods
Study eligibility and identification
Eligible studies were identified by searching PubMed, Embase, CNKI, and the Chinese Biomedicine Database (the last search update was performed on November 15, 2011), using the following search terms (TERT OR "telomerase reverse transcriptase") AND polymorphism and using the limits, Humans, English, Cancer. The related reference articles were searched to identify other relevant publications. Unpublished data and further information were also obtained from the authors. The case-control studies were selected if data were available on the role of the TERT rs2736100 polymorphism in cancer risk.
In our meta-analysis, the following inclusion criteria were used for selecting the studies: (1) articles about the TERT rs2736100 polymorphism and cancer risk, (2) case-control design, and (3) sufficient genotype data for estimating an odds ratio (OR) with a 95% confidence interval (CI). Articles that were not about cancer research, contained duplicated previous research, or did not include usable genotype data were excluded.
Data extraction
Two investigators independently extracted the data from all eligible publications using the selection criteria listed above. Any disagreement was resolved by discussion. We extracted the following information from each study when available: the first author's name, year of publication, country, patient ethnicity (composed of either European or Asian), cancer type, source of control groups (population- or hospital-based controls or mixed (composed of both population- and hospital-based controls)), genotyping method and number of cases and controls with the TT, TG, and GG genotypes.
Data synthesis
All statistical analyses were performed using the STATA software (version 11; Stata Corporation, College Station, Texas). Two-sided P values less than 0.05 were considered statistically significant. We first assessed Hardy-Weinberg equilibrium in the control groups of each study. The OR and 95% CI in each case-control study were employed to assess the strength of the associations between the TERT rs2736100 polymorphisms and cancer risk. The OR and the 95% CI in each comparison were assessed in a codominant model (GG versus TT; GT versus TT), a dominant model (GG + GT versus TT), a recessive model (GG versus GT + TT) and an additive model (2GG + TG versus 2TT + TG). Subgroup analyses were performed based on cancer type, the source of controls and ethnicity. The chi-square test-based Q-statistic was calculated to test the heterogeneity between studies. If the result of this heterogeneity test was P < 0.05, then the pooled ORs were analyzed using the random effects model (the DerSimonian and Laird method) [32]. Otherwise, if the result of this heterogeneity test was P > 0.05, indicating that the between-study heterogeneity was not significant, then the fixed-effects model was selected (the Mantel-Haenszel method) [33]. The I 2 (I 2 = 100% × (Q-df)/Q) statistic was then used to quantitatively estimate heterogeneity, with I 2 <25%, 25-75% and >75% representing low, moderate or high degrees of inconsistency, respectively [34, 35]. The significance of the combined OR was determined using the Z test (P < 0.05 was considered statistically significant). Additionally, sensitivity analyses were performed after sequential removal of each study. Cumulative meta-analyses were performed through an assortment of all eligible cancer studies with case sample size. Finally, the Begg's funnel plot and Egger's test were performed to analyze the publication bias statistically (P < 0.05 was considered a significant publication bias) [36].
Results
Eligible studies
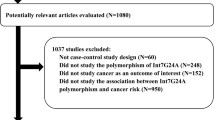
In total, 11 articles including 25 case-control studies in English with 23032 cases and 38274 controls met the inclusion criteria. The characteristics of the studies are listed in Table 1. In our meta-analysis, most of the cancer types were lung cancer and glioma. Among the 25 studies, 14 focused only on lung cancer, 9 focused only on glioma and 2 focused on other cancers. The 25 studies collected in this meta-analysis included 15 studies of Asians and 10 studies of Europeans, 17 studies of population-based controls, 6 studies of hospital-based controls and 2 study of population-based and hospital-based controls. Figure 1 shows the study selection procedure. The main results of this meta-analysis were listed in Table 2.

The study inclusion and exclusion procedures.
Evidence synthesis
There was wide variation in the TERT rs2736100 polymorphism among the controls across different ethnicities. For European populations, the G allele frequency was 51.0% (95% CI = 49.6-52.4), which was significantly (P <0.001) higher than that in the Asian populations (39.6%, 95% CI = 38.4-40.8) (Figure 2).

Frequencies of the variant alleles among controls stratified by ethnicity.
As shown in Table 2, for the TERT rs2736100 polymorphism, all studies combined (23032 cases and 38274 controls) were pooled into the meta-analysis, and a significantly increased cancer risk was found for all genetic models based on the studies (GG versus TT: OR = 1.72, 95% CI: 1.58, 1.88; GT versus TT: OR = 1.38, 95% CI: 1.29, 1.47; dominant model-TG + GG versus TT: OR = 1.47, 95% CI: 1.37, 1.58; recessive model-GG versus TT + TG: OR = 1.37, 95% CI 1.31, 1.43; additive model-2GG + TG versus 2TT + TG: OR = 1.30, 95% CI: 1.25, 1.36). Figure 3 shows the overall meta-analysis of the TERT rs2736100 polymorphism and cancer risk in the recessive model.

Overall meta-analysis of the TERT rs2736100 polymorphism and cancer risk in the recessive model.
Subgroup analysis
Specific data for the TERT rs2736100 polymorphism were stratified by cancer type: the lung cancer subgroup, the glioma subgroup and the other cancers subgroup. The pooled odds ratios for the lung cancer, glioma, the other cancers were 1.39 (95% CI 1.32, 1.47), 1.34 (95% CI 1.24, 1.44) and 1.22 (95% CI 0.99, 1.51), respectively, when we use a recessive genetic model. The meta-analysis results for the other genetic models are listed in Table 2.
In the stratified analysis by source of controls, significantly increased risks were also found. The pooled odds ratios were 1.38 (95% CI 1.29, 1.47) in the population-based controls subgroup and 1.33 (95% CI 1.25, 1.41) in the hospital-based controls subgroups in a recessive genetic model. The meta-analysis results for the other genetic models are listed in Table 2.
We stratified the studies by the ethnicity of the participants into two subgroups, Asian and European, and the pooled odds ratios were 1.40 (95% CI 1.33, 1.47) and1.31 (95% CI 1.22, 1.41), respectively, in a recessive genetic model. The meta-analysis results for the other genetic models are listed in Table 2.
Among the 25 studies, many investigators also have established an association between the TERT rs2736100 polymorphism and risk of lung adenocarcinoma (Table 3). As shown in Table 4, a significant association was observed between the TERT rs2736100 polymorphism and adenocarcinoma susceptibility in all genetic models (GG versus TT: OR = 1.85, 95% CI: 1.72, 1.98; GT versus TT: OR = 1.44, 95% CI: 1.31, 1.59; dominant model-TG + GG versus TT: OR = 1.56, 95% CI 1.42, 1.71; recessive model-GG versus TT + TG: OR = 1.50, 95% CI: 1.41, 1.60; additive model-2GG + TG versus 2TT + TG: OR = 1.36, 95% CI: 1.31, 1.41).
Sensitivity analysis
Sensitivity analyses were performed after sequential removal of each eligible study. When we investigated the TERT rs2736100 polymorphism and cancer susceptibility, the results suggested that the significance of the pooled ORs was not influenced by any single study in a recessive genetic model. Sensitivity analyses indicated that the independent study contributing the most to heterogeneity was conducted by Kohno et al. [23] (Figure 4). The heterogeneity was effectively decreased by exclusion of that study: OR = 1.37 (95% CI: 1.31, 1.43; P heterogeneity = 0.062; I 2 = 32.3%) and 1.35 (95% CI: 1.29, 1.41; P heterogeneity = 0.174; I 2 = 21.2%) before and after removal, respectively.

Influence analysis for GG versus GT/TT in the overall meta-analysis. This figure shows the influence of individual studies on the summary OR. The middle vertical axis indicates the overall OR and the two vertical axes indicate the 95% CI. Open circles indicate the pooled OR when the study indicated on the left is omitted from the meta-analysis. The lines indicate the 95% CI values when the study indicated is omitted from the meta-analysis.
Test of heterogeneity
Significant heterogeneity existed in four genetic models (GG versus TT, GT versus TT, TG + GG versus TT, 2GG + TG versus 2TT + TG) of the TERT rs2736100 polymorphism (Table 2). However, stratification based on the source of controls reduced the heterogeneity in the hospital-based controls subgroups (GG versus TT: P heterogeneity = 0.949, I 2 = 0.0%; GT versus TT: P heterogeneity = 0.892, I 2 = 0.0%; TG + GG versus TT: P heterogeneity = 0.963, I 2 = 0.0%; 2GG + TG versus 2TT + TG; P heterogeneity = 0.960, I 2 = 0.0%). When patients were stratified based on ethnicity, heterogeneity disappeared in the European (GT versus TT: P heterogeneity = 0.266, I 2 = 19.2%; TG + GG versus TT: P heterogeneity = 0.077, I 2 = 42.1%). In the analysis of the cancer type subgroups, heterogeneity disappeared in the glioma (GT versus TT: P heterogeneity = 0.138, I 2 = 35.0%).
Cumulative meta-analysis
Cumulative meta-analyses were also conducted using the eligible studies sorted by case sample size (Figure 5). There is no obvious change in the 95% confidence intervals with increasing sample size.

Results of the cumulative meta-analysis of associations between the TERT rs2736100 polymorphism and cancer risk in the recessive model. The studies were sorted based on case sample size (small to large).
Assessment of bias
The Begg's funnel plot and Egger's test were performed to assess the publication bias (Figure 6). The results did not show any evidence of publication bias (t = 1.03, P = 0.313 for GG versus GT + TT), and the 95% confidence interval (95% CI: -0.49, 1.47) included zero, indicating no publication bias. Additionally, in all genetic models, the results did not show evidence of publication bias.

Funnel plot of the TERT rs2736100 polymorphism and cancer risk data for publication bias.
Discussion
It is well known that single nucleotide polymorphisms (SNPs) are the most common sources of human genetic variation, which may contribute to an individual's susceptibility to cancer [37]. Thus genetic susceptibility to cancer has been extensively studied in the scientific community. A single nucleotide polymorphism (SNP) rs2736100 located in intron 2 of TERT, has been hypothesised to be associated with the risk of cancer development by many researchers, however, the results are conflicting and heterogeneous. Here, we analyzed pooled data from case-control studies to determine the role of TERT rs2736100 polymorphism in cancer susceptibility. In the meta-analysis conducted on 23032 cases and 38274 controls, TERT rs2736100 polymorphism was found to be associated with a significantly increased cancer risk. In the subgroup analyses by cancer type, ethnicity and source of controls, increased cancer risk in all genetic models was also found.
A number of well-designed genome-wide association studies (GWAS) have implicated variants at the 5p15.33 locus (containing the TERT gene) in cancer risk at several different sites; lung cancer, basal cell carcinoma and pancreatic cancer show strong associations, while bladder, prostate and cervical cancer as well as glioma show risk alleles in this region [38]. The biology of TERT makes it a compelling candidate gene for factors that influence cancer risk [39] and the TERT gene has been recognized as one of the most common tumor markers. The TERT gene is located on the short (p) arm of chromosome 5 at position 15.33 which is the reverse transcriptase component of telomerase and the expression of the functional TERT protein is a prerequisite for acquisition of telomerase activity. Telomerase is a ribonucleoprotein enzyme that synthesizes the TTAGGG telomeric repeat sequences that are essential for genomic stability [40, 41]. Activation of telomerase has been implicated in human cell immortalization and cancer cell pathogenesis and telomerase reexpression is a key factor in cancer cell biology, enabling malignant cells to proliferate indefinitely [7]. The commonly observed high expression of telomerase in lung cancer suggests that TERT may have an important role in lung tumorigenesis [7, 42–44]. Telomerase activity is present in most glioma samples while absent in normal brain tissues [45]. TERT expression also correlates with glioma grade and prognosis [46, 47]. Moreover, the reduction in telomerase activity may inhibit glioma cell growth [48].
Telomerase and the control of telomere length are intimately linked to the process of tumourigenesis in humans [38]. The association between TERT polymorphisms (rs401681 and rs2736098) and shorter telomere length has been recently reported [19]. The type of alteration (short vs. long telomere length) linked to a poorer survival might depend on the tumor type [49]. However, the functional significance of the SNP rs2736100 was not clear. TERT rs2736100 polymorphism may contribute directly to disease predisposition by modifying the function of TERT or is in highly linkage disequilibrium (LD) with other nearby biologically plausible and disease-causing mutations.
Adenocarcinoma is the most common histologic type of lung cancer and the relative proportion of ADC has steadily risen. The strongest risk association was observed between the TERT rs2736100 polymorphism and adenocarcinoma in all genetic models. TERT gene amplification occurred in 57% of NSCLCs, but was more common among ADCs (75%). TERT gene amplification is responsible for TERT mRNA overexpression in a majority of ADCs, while epigenetic factors at the transcriptional or post-transcriptional levels significantly affect TERT expression in NSCLC cells [50]. The re-expression of TERT may indicate progression from bronchiolo-alveolar carcinoma to adenocarcinoma [7, 51].
There are some limitations of this meta-analysis that should be discussed. First, misclassifications of the histologic type of the cancers reported may influence the results. Second, the lack of detailed information, such as age and sex of the patients, in some studies limited further stratification, and a more accurate OR would be corrected for age, sex and other factors that are associated with cancer risk. Third, in our meta-analysis, the origins of heterogeneity may include many factors, such as the differences in control characteristics and diverse genotyping methods. In addition, the small sample size (<100 cases and controls) studies appear to overestimate the true association because of deficiencies in statistical power.
Based on the limitations of the present study listed above, detailed studies are warranted to confirm our findings. Nevertheless, our meta-analysis has some advantages. First, the well-designed search and selection method significantly increased the statistical power of this meta-analysis. Second, the distribution of genotypes in the controls was consistent with Hardy-Weinberg equilibrium (P > 0.01) in all studies. Third, the results did not show any evidence of publication bias.
Conclusions
The overall results of this meta-analysis have shown that the TERT rs2736100 polymorphism is associated with cancer risk. Further functional studies between this polymorphism and cancer risk are warranted.
References
Howe HL, Wingo PA, Thun MJ, Ries LA, Rosenberg HM, Feigal EG, Edwards BK: Annual report to the nation on the status of cancer (1973 through 1998), featuring cancers with recent increasing trends. J Natl Cancer Inst. 2001, 93: 824-842.
Singh GK, Miller BA, Hankey BF: Changing area socioeconomic patterns in U.S. cancer mortality, 1950-1998: Part II--Lung and colorectal cancers. J Natl Cancer Inst. 2002, 94: 916-925.
Parkin DM, Bray F, Ferlay J, Pisani P: Global cancer statistics, 2002. CA Cancer J Clin. 2005, 55: 74-108.
Liu Y, Shete S, Hosking F, Robertson L, Houlston R, Bondy M: Genetic advances in glioma: susceptibility genes and networks. Curr Opin Genet Dev. 2010, 20: 239-244.
Karlsson P, Holmberg E, Lundell M, Mattsson A, Holm LE, Wallgren A: Intracranial tumors after exposure to ionizing radiation during infancy: a pooled analysis of two Swedish cohorts of 28,008 infants with skin hemangioma. Radiat Res. 1998, 150: 357-364.
Malmer B, Henriksson R, Gronberg H: Different aetiology of familial low-grade and high-grade glioma? A nationwide cohort study of familial glioma. Neuroepidemiology. 2002, 21: 279-286.
Lantuejoul S, Salon C, Soria JC, Brambilla E: Telomerase expression in lung preneoplasia and neoplasia. Int J Cancer. 2007, 120: 1835-1841.
Donate LE, Blasco MA: Telomeres in cancer and ageing. Philos Trans R Soc Lond B Biol Sci. 2011, 366: 76-84.
Kim NW, Piatyszek MA, Prowse KR, Harley CB, West MD, Ho PL, Coviello GM, Wright WE, Weinrich SL, Shay JW: Specific association of human telomerase activity with immortal cells and cancer. Science. 1994, 266: 2011-2015.
Broccoli D, Young JW, de Lange T: Telomerase activity in normal and malignant hematopoietic cells. Proc Natl Acad Sci USA. 1995, 92: 9082-9086.
Counter CM, Gupta J, Harley CB, Leber B, Bacchetti S: Telomerase activity in normal leukocytes and in hematologic malignancies. Blood. 1995, 85: 2315-2320. Counter CM, Gupta J, Harley CB, Leber B, Bacchetti S, 1995. Telomerase activity in normal leukocytes and in hematologic malignancies. Blood 85, 2315-2320
Wright WE, Piatyszek MA, Rainey WE, Byrd W, Shay JW: Telomerase activity in human germline and embryonic tissues and cells. Dev Genet. 1996, 18: 173-179.
Weng NP, Levine BL, June CH, Hodes RJ: Regulated expression of telomerase activity in human T lymphocyte development and activation. J Exp Med. 1996, 183: 2471-2479.
Weng NP, Granger L, Hodes RJ: Telomere lengthening and telomerase activation during human B cell differentiation. Proc Natl Acad Sci USA. 1997, 94: 10827-10832.
Gillis AJ, Schuller AP, Skordalakes E: Structure of the Tribolium castaneum telomerase catalytic subunit TERT. Nature. 2008, 455: 633-637.
Blasco MA: Telomeres and human disease: ageing, cancer and beyond. Nat Rev Genet. 2005, 6: 611-622.
Zhang A, Zheng C, Lindvall C, Hou M, Ekedahl J, Lewensohn R, Yan Z, Yang X, Henriksson M, Blennow E, Nordenskjold M, Zetterberg A, Bjorkholm M, Gruber A, Xu D: Frequent amplification of the telomerase reverse transcriptase gene in human tumors. Cancer Res. 2000, 60: 6230-6235.
Liu Y, Shete S, Hosking FJ, Robertson LB, Bondy ML, Houlston RS: New insights into susceptibility to glioma. Arch Neurol. 2010, 67: 275-278.
Rafnar T, Sulem P, Stacey SN, Geller F, Gudmundsson J, Sigurdsson A, Jakobsdottir M, Helgadottir H, Thorlacius S, Aben KK, Blondal T, Thorgeirsson TE, Thorleifsson G, Kristjansson K, Thorisdottir K, Ragnarsson R, Sigurgeirsson B, Skuladottir H, Gudbjartsson T, Isaksson HJ, Einarsson GV, Benediktsdottir KR, Agnarsson BA, Olafsson K, Salvarsdottir A, Bjarnason H, Asgeirsdottir M, Kristinsson KT, Matthiasdottir S, Sveinsdottir SG, Polidoro S, Hoiom V, Botella-Estrada R, Hemminki K, Rudnai P, Bishop DT, Campagna M, Kellen E, Zeegers MP, de Verdier P, Ferrer A, Isla D, Vidal MJ, Andres R, Saez B, Juberias P, Banzo J, Navarrete S, Tres A, Kan D, Lindblom A, Gurzau E, Koppova K, de Vegt F, Schalken JA, van der Heijden HF, Smit HJ, Termeer RA, Oosterwijk E, van Hooij O, Nagore E, Porru S, Steineck G, Hansson J, Buntinx F, Catalona WJ, Matullo G, Vineis P, Kiltie AE, Mayordomo JI, Kumar R, Kiemeney LA, Frigge ML, Jonsson T, Saemundsson H, Barkardottir RB, Jonsson E, Jonsson S, Olafsson JH, Gulcher JR, Masson G, Gudbjartsson DF, Kong A, Thorsteinsdottir U, Stefansson K: Sequence variants at the TERT-CLPTM1L locus associate with many cancer types. Nat Genet. 2009, 41: 221-227.
McKay JD, Hung RJ, Gaborieau V, Boffetta P, Chabrier A, Byrnes G, Zaridze D, Mukeria A, Szeszenia-Dabrowska N, Lissowska J, Rudnai P, Fabianova E, Mates D, Bencko V, Foretova L, Janout V, McLaughlin J, Shepherd F, Montpetit A, Narod S, Krokan HE, Skorpen F, Elvestad MB, Vatten L, Njolstad I, Axelsson T, Chen C, Goodman G, Barnett M, Loomis MM, Lubinski J, Matyjasik J, Lener M, Oszutowska D, Field J, Liloglou T, Xinarianos G, Cassidy A, Vineis P, Clavel-Chapelon F, Palli D, Tumino R, Krogh V, Panico S, Gonzalez CA, Ramon Quiros J, Martinez C, Navarro C, Ardanaz E, Larranaga N, Kham KT, Key T, Bueno-de-Mesquita HB, Peeters PH, Trichopoulou A, Linseisen J, Boeing H, Hallmans G, Overvad K, Tjonneland A, Kumle M, Riboli E, Zelenika D, Boland A, Delepine M, Foglio M, Lechner D, Matsuda F, Blanche H, Gut I, Heath S, Lathrop M, Brennan P: Lung cancer susceptibility locus at 5p15.33. Nat Genet. 2008, 40: 1404-1406.
Jin G, Xu L, Shu Y, Tian T, Liang J, Xu Y, Wang F, Chen J, Dai J, Hu Z, Shen H: Common genetic variants on 5p15.33 contribute to risk of lung adenocarcinoma in a Chinese population. Carcinogenesis. 2009, 30: 987-990.
Wang Y, Broderick P, Matakidou A, Eisen T, Houlston RS: Role of 5p15.33 (TERT-CLPTM1L), 6p21.33 and 15q25.1 (CHRNA5-CHRNA3) variation and lung cancer risk in never-smokers. Carcinogenesis. 2010, 31: 234-238.
Kohno T, Kunitoh H, Shimada Y, Shiraishi K, Ishii Y, Goto K, Ohe Y, Nishiwaki Y, Kuchiba A, Yamamoto S, Hirose H, Oka A, Yanagitani N, Saito R, Inoko H, Yokota J: Individuals susceptible to lung adenocarcinoma defined by combined HLA-DQA1 and TERT genotypes. Carcinogenesis. 2010, 31: 834-841.
Hsiung CA, Lan Q, Hong YC, Chen CJ, Hosgood HD, Chang IS, Chatterjee N, Brennan P, Wu C, Zheng W, Chang GC, Wu T, Park JY, Hsiao CF, Kim YH, Shen H, Seow A, Yeager M, Tsai YH, Kim YT, Chow WH, Guo H, Wang WC, Sung SW, Hu Z, Chen KY, Kim JH, Chen Y, Huang L, Lee KM, Lo YL, Gao YT, Liu L, Huang MS, Jung TH, Jin G, Caporaso N, Yu D, Kim CH, Su WC, Shu XO, Xu P, Kim IS, Chen YM, Ma H, Shen M, Cha SI, Tan W, Chang CH, Sung JS, Zhang M, Yang TY, Park KH, Yuenger J, Wang CL, Ryu JS, Xiang Y, Deng Q, Hutchinson A, Kim JS, Cai Q, Landi MT, Yu CJ, Tucker M, Hung JY, Lin CC, Perng RP, Boffetta P, Chen CY, Chen KC, Yang SY, Hu CY, Chang CK, Fraumeni JF, Chanock S, Yang PC, Rothman N, Lin D: The 5p15.33 locus is associated with risk of lung adenocarcinoma in never-smoking females in Asia. PLoS Genet. 2010, 6:
Miki D, Kubo M, Takahashi A, Yoon KA, Kim J, Lee GK, Zo JI, Lee JS, Hosono N, Morizono T, Tsunoda T, Kamatani N, Chayama K, Takahashi T, Inazawa J, Nakamura Y, Daigo Y: Variation in TP63 is associated with lung adenocarcinoma susceptibility in Japanese and Korean populations. Nat Genet. 2010, 42: 893-896.
Hu Z, Wu C, Shi Y, Guo H, Zhao X, Yin Z, Yang L, Dai J, Hu L, Tan W, Li Z, Deng Q, Wang J, Wu W, Jin G, Jiang Y, Yu D, Zhou G, Chen H, Guan P, Chen Y, Shu Y, Xu L, Liu X, Liu L, Xu P, Han B, Bai C, Zhao Y, Zhang H, Yan Y, Ma H, Chen J, Chu M, Lu F, Zhang Z, Chen F, Wang X, Jin L, Lu J, Zhou B, Lu D, Wu T, Lin D, Shen H: A genome-wide association study identifies two new lung cancer susceptibility loci at 13q12.12 and 22q12.2 in Han Chinese. Nat Genet. 2011, 43: 792-796.
Shete S, Hosking FJ, Robertson LB, Dobbins SE, Sanson M, Malmer B, Simon M, Marie Y, Boisselier B, Delattre JY, Hoang-Xuan K, El Hallani S, Idbaih A, Zelenika D, Andersson U, Henriksson R, Bergenheim AT, Feychting M, Lonn S, Ahlbom A, Schramm J, Linnebank M, Hemminki K, Kumar R, Hepworth SJ, Price A, Armstrong G, Liu Y, Gu X, Yu R, Lau C, Schoemaker M, Muir K, Swerdlow A, Lathrop M, Bondy M, Houlston RS: Genome-wide association study identifies five susceptibility loci for glioma. Nat Genet. 2009, 41: 899-904.
Wrensch M, Jenkins RB, Chang JS, Yeh RF, Xiao Y, Decker PA, Ballman KV, Berger M, Buckner JC, Chang S, Giannini C, Halder C, Kollmeyer TM, Kosel ML, LaChance DH, McCoy L, O'Neill BP, Patoka J, Pico AR, Prados M, Quesenberry C, Rice T, Rynearson AL, Smirnov I, Tihan T, Wiemels J, Yang P, Wiencke JK: Variants in the CDKN2B and RTEL1 regions are associated with high-grade glioma susceptibility. Nat Genet. 2009, 41: 905-908.
Schoemaker MJ, Robertson L, Wigertz A, Jones ME, Hosking FJ, Feychting M, Lonn S, McKinney PA, Hepworth SJ, Muir KR, Auvinen A, Salminen T, Kiuru A, Johansen C, Houlston RS, Swerdlow AJ: Interaction between 5 genetic variants and allergy in glioma risk. Am J Epidemiol. 2010, 171: 1165-1173.
Chen H, Chen Y, Zhao Y, Fan W, Zhou K, Liu Y, Zhou L, Mao Y, Wei Q, Xu J, Lu D: Association of sequence variants on chromosomes 20, 11, and 5 (20q13.33, 11q23.3, and 5p15.33) with glioma susceptibility in a Chinese population. Am J Epidemiol. 2011, 173: 915-922.
Gago-Dominguez M, Jiang X, Conti DV, Castelao JE, Stern MC, Cortessis VK, Pike MC, Xiang YB, Gao YT, Yuan JM, Van Den Berg DJ: Genetic variations on chromosomes 5p15 and 15q25 and bladder cancer risk: findings from the Los Angeles-Shanghai bladder case control study. Carcinogenesis. 2011, 32: 197-202.
DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials. 1986, 7: 177-188.
Mantel N, Haenszel W: Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959, 22: 719-748.
Higgins JP, Thompson SG: Quantifying heterogeneity in a meta-analysis. Stat Med. 2002, 21: 1539-1558.
Higgins JP, Thompson SG, Deeks JJ, Altman DG: Measuring inconsistency in meta-analyses. BMJ. 2003, 327: 557-560.
Egger M, Davey Smith G, Schneider M, Minder C: Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997, 315: 629-634.
Wu GY, Hasenberg T, Magdeburg R, Bonninghoff R, Sturm JW, Keese M: Association between EGF, TGF-beta1, VEGF gene polymorphism and colorectal cancer. World J Surg. 2009, 33: 124-129.
Baird DM: Variation at the TERT locus and predisposition for cancer. Expert Rev Mol Med. 2010, 12: e16-
Broderick P, Wang Y, Vijayakrishnan J, Matakidou A, Spitz MR, Eisen T, Amos CI, Houlston RS: Deciphering the impact of common genetic variation on lung cancer risk: a genome-wide association study. Cancer Res. 2009, 69: 6633-6641.
Harley CB, Kim NW, Prowse KR, Weinrich SL, Hirsch KS, West MD, Bacchetti S, Hirte HW, Counter CM, Greider CW, et al: Telomerase, cell immortality, and cancer. Cold Spring Harb Symp Quant Biol. 1994, 59: 307-315.
Artandi SE, DePinho RA: A critical role for telomeres in suppressing and facilitating carcinogenesis. Curr Opin Genet Dev. 2000, 10: 39-46.
Mavrogiannou E, Strati A, Stathopoulou A, Tsaroucha EG, Kaklamanis L, Lianidou ES: Real-time RT-PCR quantification of human telomerase reverse transcriptase splice variants in tumor cell lines and non-small cell lung cancer. Clin Chem. 2007, 53: 53-61.
Wu TC, Lin P, Hsu CP, Huang YJ, Chen CY, Chung WC, Lee H, Ko JL: Loss of telomerase activity may be a potential favorable prognostic marker in lung carcinomas. Lung Cancer. 2003, 41: 163-169.
Feldser DM, Hackett JA, Greider CW: Telomere dysfunction and the initiation of genome instability. Nat Rev Cancer. 2003, 3: 623-627.
Shervington A, Cruickshanks N, Wright H, Atkinson-Dell R, Lea R, Roberts G, Shervington L: Glioma: what is the role of c-Myc, hsp90 and telomerase?. Mol Cell Biochem. 2006, 283: 1-9.
Wager M, Menei P, Guilhot J, Levillain P, Michalak S, Bataille B, Blanc JL, Lapierre F, Rigoard P, Milin S, Duthe F, Bonneau D, Larsen CJ, Karayan-Tapon L: Prognostic molecular markers with no impact on decision-making: the paradox of gliomas based on a prospective study. Br J Cancer. 2008, 98: 1830-1838.
Wang L, Wei Q, Wang LE, Aldape KD, Cao Y, Okcu MF, Hess KR, El-Zein R, Gilbert MR, Woo SY, Prabhu SS, Fuller GN, Bondy ML: Survival prediction in patients with glioblastoma multiforme by human telomerase genetic variation. J Clin Oncol. 2006, 24: 1627-1632.
Falchetti ML, Fiorenzo P, Mongiardi MP, Petrucci G, Montano N, Maira G, Pierconti F, Larocca LM, Levi A, Pallini R: Telomerase inhibition impairs tumor growth in glioblastoma xenografts. Neurol Res. 2006, 28: 532-537.
Svenson U, Roos G: Telomere length as a biological marker in malignancy. Biochim Biophys Acta. 2009, 1792: 317-323.
Zhu CQ, Cutz JC, Liu N, Lau D, Shepherd FA, Squire JA, Tsao MS: Amplification of telomerase (hTERT) gene is a poor prognostic marker in non-small-cell lung cancer. Br J Cancer. 2006, 94: 1452-1459.
Aviel-Ronen S, Coe BP, Lau SK, DA Cunha Santos G, Zhu CQ, Strumpf D, Jurisica I, Lam WL, Tsao MS: Genomic markers for malignant progression in pulmonary adenocarcinoma with bronchioloalveolar features. Proc Natl Acad Sci USA. 2008, 105: 10155-10160.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/12/7/prepub
Acknowledgements
We thank Dr. Meilin Wang for the scientific design. This work is supported by the National Natural Science Foundation of China (grant 30901534); and Jiangsu Province's Natural Science Foundation (Proj. no. BK2009444); and the Grant for the 135 Key Medical Project of Jiangsu Province, (No. XK201117).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
PZ participated in collection of data and manuscript preparation. GJ and LZ performed the statistical analysis. PZ and AG participated in study design and critically revised the manuscript. PZ and AL participated in study design and manuscript preparation. All authors read and approved the final manuscript.
Peng Zou, Aihua Gu contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Zou, P., Gu, A., Ji, G. et al. The TERT rs2736100 Polymorphism and Cancer Risk: A Meta-analysis Based on 25 Case-Control Studies. BMC Cancer 12, 7 (2012). https://doi.org/10.1186/1471-2407-12-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-12-7