
Abstract
Background
An increased prevalence of coeliac disease in patients with primary biliary cirrhosis has been recently reported. However, in other studies the association has not been confirmed. There have been no formal attempts to systematically evaluate patients with autoimmune cholangitis for coeliac disease.
Methods
Sera from 62 patients with primary biliary cirrhosis, 17 with autoimmune cholangitis and 100 blood donors were screened for anti-gliadin, anti-endomysial, anti-reticulin, and IgA class antibodies to guinea pig liver-derived tissue transglutaminase. Eighteen untreated coeliacs served as methodological controls. Analyses were performed by using the χ2 and Fischer's exact tests.
Results
Anti-gliadin antibodies were detected in 21% of patients with primary biliary cirrhosis, 35% of patients with autoimmune cholangitis, and 3% of controls (p < 0.001). IgA class gliadin antibodies positivity was more pronounced in patients with Scheuer's stage III-IV disease (p < 0.05). Anti-transglutaminase antibodies were detected in 10% and in 18% of patients with primary biliary cirrhosis and autoimmune cholangitis respectively (p < 0.001). Anti-reticulin and anti-endomysial antibodies were negative in all patients. Duodenal biopsies were performed in 59% and 71% of patients with primary biliary cirrhosis and autoimmune cholangitis respectively, tested positive for at least one antibody class. No histological features of coeliac disease were found.
Conclusions
We were unable to demonstrate an increased risk of coeliac disease in patients with primary biliary cirrhosis and autoimmune cholangitis. Our results confirm the previously reported high prevalence of false-positive anti-gliadin and guinea pig liver-derived anti-tissue transglutaminase antibodies in patients with chronic liver disease.
Similar content being viewed by others


Background
Since the initial description of four patients with coeliac disease (CD) and primary biliary cirrhosis (PBC) [1], there have been several subsequent reports demonstrating an association of these two diseases [2–7]. Recently, a number of epidemiological studies reported an increased, up to 7%, prevalence of CD in patients with PBC and an increased prevalence, up to 3%, of PBC in patients with CD [8, 9]. Screening for one disease when the other is identified has therefore been suggested. However, in other studies this association was found less pronounced or has not been confirmed [10–13]. Autoimmune cholangitis (AIC) was first reported as an overlap syndrome of autoimmune hepatitis and PBC, but is considered by most as a discrete entity of antimitochondrial antibody (AMA)-negative PBC with autoimmune characters [14]. Apart from a case report [15], no relation of adult CD to autoimmune cholangitis has so far been described. However, there have been no formal attempts to systematically evaluate patients with AIC for CD, presumably because AIC represents a rare form of chronic cholestatic liver disease.
Although a definite diagnosis of CD still requires histopathologic examination of the small intestinal mucosa, the screening methods for large number of individuals are based on non-invasive serological tests, namely, anti-gliadin (AGA, IgG and IgA class), anti-reticulin (ARA R1-type, IgA class) and anti-endomysial (EMA, IgA class) antibodies [16–18]. The combined use of serum IgG-AGA (good sensitivity) and IgA-EMA (good specificity) has resulted in a reliable screening test for diagnosis of CD [19]. However, anti-gliadin antibodies (AGAs) are not suitable for CD screening in patients with chronic liver diseases including PBC, as an unacceptably high percentage of false-positives was reported in several studies [11, 20, 21]. In this respect, a previous study revealed that the serum IgA-EMA assay is the optimum test for predicting CD in patients with chronic liver disease [11]. Although IgA class antibodies to guinea pig liver-derived tissue transglutaminase (IgA-tTG) have been shown to be highly specific and sensitive for the diagnosis of CD [22–26], it was recently reported that in patients with chronic liver disease there was a high frequency of false-positives which disappeared when human tTG was used as the antigen in the ELISA system [27]. In the present study we evaluated AGAs, IgA-ARA, IgA-EMA and guinea pig liver-derived IgA-tTG in 62 patients with PBC and 17 patients with AIC. Intestinal biopsies have been subsequently performed in the majority of patients tested positive for at least one antibody class.
Methods
Materials
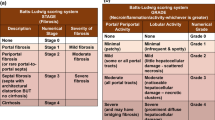
Serum samples from 62 patients with PBC (53 women and nine men; mean age, 59 years; range, 32–85 years) and 17 patients with AIC (16 women and one man; mean age, 62 years; range, 52–77 years) were used in the study. The samples were collected prospectively over a 2 yr. period (1999–2000) and stored in aliquots at -20°C. Diagnosis of PBC was based on standard laboratory findings, compatible liver histology and the presence of AMA in titer > 1:80. Class 2 AMA antibodies (M2) detected by ELISA were positive in all patients. According to Scheuer's classification [28], 34 patients (54%) had stage I-II and 28 (46%) stage III-IV disease. The mean follow-up period from the time of diagnosis was 5.2 years (range, 1–9.4 years).
The diagnosis of AIC has been made on cholestatic patients with a liver biopsy compatible with PBC, without AMA or M2 positivity. ANA were positive (titers ≥ 1:160) in all 17 patients. Anti-smooth muscle antibodies were positive (titer ≥ 1:80) in 9 patients. According to Scheuer's classification, 10 patients (58%) had stage I-II and 7 (42%) stage III-IV disease. The mean follow-up after diagnosis was 6.6 years (range, 1–7.8 years).
Ultrasound, computed tomography and endoscopic retrograde cholangiography ruled out the possibility of biliary obstruction, when the latter was suspected. No patient had a family history of CD, or IgA deficiency. One PBC patient was HbsAg positive and one PBC patient and two AIC patients were anti-HCV positive. One hundred Cretan adults selected at random from blood donors served as controls. Eighteen serum samples from symptomatic, biopsy-proven, AMA negative adults with CD were included in the study as methodological controls. Total IgA was measured in all CD patients and healthy controls to exclude IgA deficiency.
Methods
Two operators unaware of the clinical parameters performed the immunological tests. All PBC, AIC, CD and control sera were screened for AGAs, IgA-ARA, IgA-EMA and IgA-tTG. IgA- and IgG-AGA were screened by a commercial ELISA at a dilution of 1:50 (Alphadia SA/NV, Belgium). Values greater than 50 U/mL were considered positive. Results were considered doubtful and repeated for values between 45 and 50 U/mL. For IgA-ARA R1-type, sera were tested by an indirect immunofluorescence (IIF) test at a 1:10 and 1:40 dilution, using rat liver, kidney and stomach as substrates (Sanofi Diagnostics Pasteur, France). Sera were screened for IgA-EMA by IIF, using both monkey oesophagus (Biosystems, Barcelona, Spain) and human umbilical cord (Eurospital SpA, Trieste, Italy) as substrates. Titers of ≥ 1:5 were considered positive. To avoid false-negative results, IgA-EMA were also evaluated at a 1:50 dilution. IgA-tTG were tested by a commercially available guinea-pig liver-derived tTG ELISA kit at a dilution of 1:101, according to manufacturers' instructions (QUANTA Lite™ tTG ELISA, INOVA Diagnostics, San Diego, USA). The samples were classified as negative (<20 Units), weakly positive (20–30 Units) and strongly positive (>30 Units). Small intestinal biopsies were performed at endoscopy using endoscopic forceps. Four biopsy specimens from opposite sites of the distal duodenum were obtained and evaluated by one observer specialized in gastrointestinal tract pathology with regard to the villi/crypts ratio and the number of intraepithelial lymphocytes (IELs) per 100 surface epithelial cells. Small bowel biopsies from the patients with PBC and AIC were evaluated blindly with those obtained from the 18 patients with untreated CD. When biopsy specimen revealed features of CD [29], namely, a lowering of the villous height to crypt depth ratio (normal, 3–5:1) and/or an increase in IELs (normal, 10–30 per 100 epithelial cells) a more detailed histological classification was applied [30].
Test results were compared using a 2 × 2 contingency table and chi-squared statistics. When appropriate, Fisher's exact test was used. P values below 0.05 were considered significant.
Results
IgA class anti-gliadin antibodies and IgA class antibodies to tissue transglutaminase were detected with a significantly increased frequency in patients with both PBC and AIC as compared to healthy blood donors (Table 1). In contrast, none of the PBC and AIC patients was tested positive for anti-reticulin or anti-endomysial antibodies. Controls were tested negative for anti-reticulin, anti-endomysial and IgA class anti-tissue transglutaminase antibodies.
PBC patients (Table 2)
Both anti-gliadin antibodies were detected in 13 out of 62 patients with PBC (21% vs. 3% in controls, p < 0.001). IgA-AGA were tested positive in 12 patients (19%, p < 0.001), of whom 5 had stage I-II disease, and 7 had stage II-IV disease. IgA-AGA positivity was significantly more pronounced in patients with stage III-IV disease (25% vs 14%, p < 0.05). IgA-tTG were detected in 6 patients (10%), 3 of whom had stage I-II disease and another 3 stage III-IV disease, while tested negative in all controls (p < 0.001). Serology was negative in the two patients with a superimposed viral hepatitis infection.
AIC patients (Table 3)
IgA-AGA were tested positive in 6 patients with AIC (35% vs. 3% in controls, p < 0.001), two with stage I-II disease and four with stage III-IV disease. IgA-AGA positivity was significantly more pronounced in patients with stage III-IV disease (57% vs 20%, p < 0.05). IgA-tTG were detected in 3 patients with AIC (18%), two patients with stage I-II disease and one patient with stage III-IV disease, while tested negative in all controls (p < 0.001). Serology was negative in two AIC patients with superimposed hepatitis C.
CD patients
All 18 patients with coeliac disease were tested positive for IgA-ARA, IgA-EMA and IgA-tTG, whereas 16 of them had also both IgA and IgG anti-gliadin antibodies.
Healthy blood donors
None of the 100 tested sera were found to be IgA-EMA or IgA-tTG positive. However AGAs were present in 3 individuals (IgA-AGA in one and IgG-AGA in two).
Duodenal biopsies
Overall, biopsies were performed in 10 out of 17 PBC patients (59%) and 5 out of 7 AIC patients (71%) tested IgA-AGA and/or IgG-AGA and/or IgA-tTG positive. Five patients died shortly after testing positive and four patients refused any further investigation. None of the biopsied PBC and AIC patients had features suggestive of CD. Small bowel biopsies of our 18 patients with CD revealed partial villous atrophy (Marsh IIIa) in three, subtotal villous atrophy (Marsh IIIb) in eleven and total villous atrophy (Marsh IIIc) in four.
Discussion
In contrast to recent reports from Wales [8], Scandinavia [9], Northern Ireland [31], and Canada [32], the present study has not been able to demonstrate an increased risk of coeliac disease in this group of 62 Cretan patients with primary biliary cirrhosis. Our results are consistent with data from Sweden [11] and Italy [12, 13], suggesting that if there is no clinical suspicion of CD, screening with anti-endomysial antibodies should not be performed routinely in all patients with PBC.
A possible explanation relevant to these controversies could be the methodological differences in detecting and defining CD, like the different serological tests used for screening (AGAs and/or IgA-EMA), the degree of intestinal damage, or the spectrum of clinical presentation of CD in patients studied. Patients with malabsorption, diarrhoea, weight loss, and total villous atrophy represent perhaps only 30–40% of the entire spectrum of gluten-sensitised individuals [19]. However, studies supporting the association between PBC and CD have included mainly symptomatic or complicated cases. In Kingham's et al study [8], CD in patients with PBC was sought by investigating features suggestive of malabsorption, a family history of CD, the presence of AGAs, or the finding of otherwise unexplained haematinic deficiency. In Sorensen's et al paper [9], it is not clear whether all patients with CD were systematically evaluated for PBC. PBC was found in patients hospitalised for CD, which presumably excluded patients with subclinical or silent disease. Furthermore, no information was available for patients treated as outpatients.
The inconsistencies between studies may also be attributed to the ethnic variability of CD prevalence in the different populations. The prevalence of CD in Greece is currently unknown, because of the lack of official epidemiological data, but it is probably low. A crude estimation concerning of the prevalence of CD in Greece is provided from an endoscopic study from Athens, reporting one new case of unsuspected CD per 520 endoscopies [33]. When we retrospectively looked for, only 23 adult patients with symptomatic gluten-sensitive enteropathy were found over a 9 year period in a specialized University Unit, which is the main reference center for the total population of the island of Crete (approximately 500 000 people).
We do recognize the fact that the size of the studied samples is not large enough to permit us to refute the presence of an association between CD and PBC safely. However, our inability to confirm this association is in agreement with recent data from large Italian series [13], consisted of 336 patients with CD and 65 cases with PBC. In this study, which can be assumed to be representative of the Mediterranean population, only one case of PBC among patients with CD was identified and no case of CD in the group of PBC.
Patients with autoimmune cholangitis were not included in the studies aiming to estimate the risk of CD in patients with PBC. In our small series, no case of CD was found among the 17 patients with autoimmune cholangitis and thus an association could not be established.
A possible limitation of our study may be the relatively low percentage of duodenal biopsies performed in patients with primary biliary cirrhosis tested positive for at least one antibody class. However, this was also the case in studies supporting the association. Our patients were screened for IgA-EMA by indirect immunofluorescence (IIF) test, using both monkey esophagus and human umbilical cord as substrates which have been shown to be highly sensitive and specific indicators of untreated coeliac disease [16, 17]. Thus missing a case of CD in our patients with PBC seems rather unlikely. It was previously reported that the development of IgA-EMA depends on the severity of intestinal histopathology of CD and a subgroup of asymptomatic coeliacs negative for AGAs or IgA-EMA will be under-diagnosed, especially those with minor tissue damage [30]. However, none of the studies supporting or failing to demonstrate the association have focused on this aspect.
In our series, 21% of PBC and 35% of AIC patients were tested positive for AGAs. Furthermore, IgA-AGA positivity was significantly more pronounced in patients with Scheuer's stage III-IV disease. Floreani et al [20] reported that IgA-AGA were found in 3.4%, whereas both IgA and IgG-AGA in 6.8% of PBC patients. Likewise, Sjoberg et al [11] reported that the occurrence of false-positive AGAs in PBC patients was as high as 16%. We therefore believe, as previously suggested [11, 20, 21], that the presence of AGAs in PBC and AIC seems to be secondary to liver damage per se and represent a marker of non-specific immune reactivity. Finally, our results confirm the previously reported low specificity of guinea pig liver-derived tTG ELISA in patients with chronic liver disease [27]. We were unable to compare our results with those obtained by a human recombinant tTG ELISA as the latter is not currently commercially available in our country.
Conclusions
We confirmed the previously reported high prevalence of false-positive anti-gliadin and guinea pig liver-derived anti-tissue transglutaminase antibodies in patients with chronic liver disease. We were unable to confirm observations suggesting an over-representation of coeliac disease in patients with primary biliary cirrhosis. Our findings support the idea that in areas of low prevalence of CD, in the absence of clinical suspicion, screening all patients with PBC for coeliac disease should not be performed routinely.
References
Logan RF, Ferguson A, Finlayson ND, Weir DG: Primary biliary cirrhosis and coeliac disease: An association?. Lancet. 1978, 1: 230-233. 10.1016/S0140-6736(78)90480-4.
Iliffe GD, Owen DA: An association between primary biliary cirrhosis and jejunal villous atrophy resembling celiac disease. Dig Dis Sci. 1979, 24: 802-806.
Olsson R, Kagevi I, Rydeberg L: On the concurrence of primary biliary cirrhosis and intestinal villous atrophy. Scand J Gastroenterol. 1982, 17: 625-628.
Shanahan F, O' Regan PFB, Crowe JP: Primary biliary cirrhosis associated with coeliac disease. Ir Med J. 1983, 76: 282-
Schrijver G, van Berge Henegouwen GP, Bronkhost FB: Gluten-sensitive coeliac disease and primary biliary cirrhosis syndrome. Neth J Med. 1984, 27: 218-221.
Behr W, Barnert J: Adult celiac disease and primary biliary cirrhosis. Am J Gastroenterol. 1986, 81: 796-799.
Lohr M, Lotterer E, Hahn EG, Fleig WF: Primary biliary cirrhosis associated with coeliac disease. Eur J Gastroenterol Hepatol. 1994, 6: 263-267.
Kingham JPC, Parker DR: The association between primary biliary cirrhosis and coeliac disease: a study of relative prevalences. Gut. 1998, 42: 120-122.
Sorensen HT, Thulstrup AM, Blomqvist P, Norgaard B, Fonager A, Ekbom A: Risk of primary biliary cirrhosis in patients with coeliac disease: Danish and Swedish cohort data. Gut. 1999, 44: 736-738.
Fidler HM, Butler P, Burroughs AK, McIntyre N, Bunn C, McMarrow M, Walmsley R, Dooley J: Co-screening for primary biliary cirrhosis and coeliac disease. Primary biliary cirrhosis and coeliac disease: a study of relative prevalences. Gut. 1998, 43: 300-302.
Sjoberg K, Lindgren S, Erikson S: Frequent occurrence of non-specific gliadin antibodies in chronic liver disease. Endomysial but not gliadin antibodies predict coeliac disease in patients with chronic liver disease. Scand J Gastroenterol. 1997, 32: 1162-1167.
Volta U, De Franceshi L, Molinaro N, Cassani F, Muratori L, Lenzi M, Bianchi FB, Czaja AJ: Frequency and significance of anti-gliadin and anti-endomysial antibodies in autoimmune hepatitis. Dig Dis Sci. 1998, 43: 2190-2195. 10.1023/A:1026650118759.
Bardella MT, Quatrini M, Zuin M, Podda M, Cesarini L, Velio P, Bianchi P, Conte D: Screening patients with celiac disease for primary biliary cirrhosis and vice versa. Am J Gastroenterol. 1997, 92: 1524-1526.
Heathcote J: Autoimmune cholangitis. Gut. 1997, 40: 440-442.
Gogos CA, Nikolopoulou V, Zolota V, Siampi V, Vagenakis A: Autoimmune cholangitis in a patient with celiac disease: a case report and review of the literature. J Hepatol. 1999, 30: 321-324. 10.1016/S0168-8278(99)80079-8.
Maki M: The humoral immune system in coeliac disease. Baillieres Clin Gastroenterol. 1995, 9: 231-249.
Unsworth DJ: Serological diagnosis of gluten sensitive enteropathy. J Clin Pathol. 1996, 49: 704-711.
Maki M, Collin P: Coeliac disease. Lancet. 1997, 349: 1755-1759. 10.1016/S0140-6736(96)70237-4.
Fasano A, Catassi C: Current approaches to diagnosis and treatment of celiac disease: An evolving spectrum. Gastroenterology. 2001, 120: 636-51.
Floreani A, Chiarimonte M, Venturini R, Plebani M, Martin A, Giacomini A, Naccarato R: Antigliadin antibody classes in chronic liver diseases. Ital J Gastronetrol. 1992, 24: 457-460.
Lindgren S, Sjoberg K, Erikson S: Unsuspected coeliac disease in chronic 'cryptogenic' liver disease. Scand J Gastroenterol. 1994, 29: 661-4.
Dieterich W, Ehnis T, Bauer M, Donner P, Volta U, Rieken EO, Schuppan D: Identification of tissue transglutaminase as the autoantigen of celiac disease. Nat Med. 1997, 3: 797-801.
Dieterich W, Laag E, Schopper H, Volta U, Ferguson A, Gillet H, Rieken EO, Schuppan D: Autoantibodies to tissue transglutaminase as predictors of celiac disease. Gastroenterology. 1998, 115: 1317-1321.
Sulkanen S, Haltunen T, Laurila K, Kolho KL, Korponay IR-Szabo, Sarnesto A, Savilahti E, Collin P, Maki M: Tissue transglutaminase Enzyme-Linked Immunoabsorbent Assay in detecting celiac disease. Gastroenterology. 1998, 115: 1322-1328.
Lock RJ, Pitcher MCL, Unsworth DJ: IgA anti-tissue transglutaminase as a diagnostic marker of gluten sensitive enteropathy. J Clin Pathol. 1999, 52: 274-277.
Biagi F, Ellis HJ, Yiannakou JY, Brusco G, Swift GL, Smith PM, Corazza GR, Ciclitira PJ: Tissue transglutaminase antibodies in celiac disease. Am J Gastroenterol. 1999, 94: 2187-2192. 10.1016/S0002-9270(99)00348-2.
Carroccio A, Giannitrapani L, Soresi M, Not T, Iacono G, Di Rosa C, Panfili E, Notarbatolo A, Montalto G: Guinea pig transglutaminase immunolinked assay does not predict coeliac disease in patients with chronic liver disease. Gut. 2001, 49: 506-511. 10.1136/gut.49.4.506.
Scheuer PJ: Primary biliary cirrhosis: Chronic non-suppurative destructive cholangitis. Am J Pathol. 1965, 46: 387-
American Gastroenterological Association Medical Position Statement: Celiac Sprue. Gastroenterology. 2001, 120: 1522-1525.
Rostami K, Kerckhaert J, Tiemessen R, von Blomberg ME, Meijer JWR, Mulder CJJ: Sensitivity of antiendomysium and antigliadin antibodies in untreated celiac disease: Disappointing in clinical practice. Am J Gastroenterol. 1999, 94: 888-894. 10.1016/S0002-9270(99)00038-6.
Dickey W, McMillan SA, Callender ME: High prevalence of celiac sprue among patients with primary biliary cirrhosis. J Clin Gastroenterol. 1997, 25: 328-329. 10.1097/00004836-199707000-00006.
Gillett HR, Cauch-Dudek K, Jenny E, Heathcote EJ, Freeman HJ: Prevalence of IgA antibodies to endomysium and tissue transglutaminase in primary biliary cirrhosis. Can J Gastroenterol. 2000, 14: 665-666.
Rokkas T, Karameris A: The usefulness of endoscopy in diagnosing celiac disease in Greece. Gastrointest Endosc. 2000, 52: 451-10.1067/mge.2000.107287.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-230X/2/5/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
none declared
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Chatzicostas, C., Roussomoustakaki, M., Drygiannakis, D. et al. Primary biliary cirrhosis and autoimmune cholangitis are not associated with coeliac disease in Crete. BMC Gastroenterol 2, 5 (2002). https://doi.org/10.1186/1471-230X-2-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-230X-2-5