
Abstract
Purpose
To identify risk factors associated with mortality in patients with severe community-acquired pneumonia (CAP) caused by S. pneumoniae who require intensive care unit (ICU) management, and to assess the prognostic values of these risk factors at the time of admission.
Methods
Retrospective analysis of all consecutive patients with CAP caused by S. pneumoniae who were admitted to the 32-bed medico-surgical ICU of a community and referral university hospital between 2002 and 2011. Univariate and multivariate analyses were performed on variables available at admission.
Results
Among the 77 adult patients with severe CAP caused by S. pneumoniae who required ICU management, 12 patients died (observed mortality rate 15.6 %). Univariate analysis indicated that septic shock and low C-reactive protein (CRP) values at admission were associated with an increased risk of death. In a multivariate model, after adjustment for age and gender, septic shock [odds ratio (OR), confidence interval 95 %; 4.96, 1.11–22.25; p = 0.036], and CRP (OR 0.99, 0.98–0.99 p = 0.034) remained significantly associated with death. Finally, we assessed the discriminative ability of CRP to predict mortality by computing its receiver operating characteristic curve. The CRP value cut-off for the best sensitivity and specificity was 169.5 mg/L to predict hospital mortality with an area under the curve of 0.72 (0.55–0.89).
Conclusions
The mortality of patients with S. pneumoniae CAP requiring ICU management was much lower than predicted by severity scores. The presence of septic shock and a CRP value at admission <169.5 mg/L predicted a fatal outcome.
Similar content being viewed by others

Introduction
Up to 10 % of all patients hospitalized with community-acquired pneumonia (CAP) require intensive care unit (ICU) management [1, 2]. Despite improvement in its general management, CAP is still a common cause of death in western countries [3, 4]. The main pathogen isolated from CAP patients requiring hospital management is Streptococcus pneumonia [5–7]. The burden of invasive pneumococcal infections is high. In the United Sates, there were 8,000 cases of pneumococcal bloodstream infections and 106,000–175,000 cases of pneumonia caused by pneumococcal infections that required hospitalization per year in 2000 [8]. Moreover, there were rising incidences of pneumococcal infections in infants (<1 year) and the elderly (>65 years) in whom rates may be as high as 30 cases/100,000 per year [8].
The epidemiology of nonsevere pneumonia caused by S. pneumoniae has been well studied [2, 7], but few data have been collected regarding patients developing severe forms of infection and requiring ICU management. In a recent prospective study of 1166 patients with severe CAP who were admitted to ICUs across 17 European countries, S. pneumoniae was the most commonly isolated organism (29 % of cases), and it was the most common cause of bacteremia and empyema [7]. Some studies suggested a correlation between the presence of co-morbidities and poor outcomes [4, 9], but others did not [5, 6]. A recent large prospective study in France indicated that death was influenced by the presence of septic shock and organ failure [10] rather than comorbidities.
In patients requiring ICU management, early identification of those with more severe outcomes would allow for more tailored therapeutic strategies. In this study, we aimed to examine the risk factors associated with mortality in patients with severe S. pneumoniae CAP requiring ICU management, and to assess their prognosis at the time of admission. We retrospectively analyzed the risk factors potentially associated with fatal outcomes in a cohort of patients with a severe form of S. pneumoniae CAP who were admitted to our medico-surgical 32-bed ICU over the last decade.
Methods
Patient population
We retrospectively included all consecutive adults ≥18 years of age who were admitted with severe CAP caused by S. pneumoniae to our 32-bed medico-surgical ICU at the Centre Hospitalier Universitaire Vaudois (CHUV), a community and referral university hospital, between January 2002 and December 2011. Patients with meningitis and/or invasive ear, nose, and throat (ENT) infections were excluded from the analysis. The present research has been performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. The Institutional Review Board “Commission cantonale d’éthique de la recherche sur l’être humain” granted retrospective access to the data without need for individual informed consent.
Data collection
For each patient, we recorded the age, sex, and severe comorbidities according to the standard definitions used in the severity score. Clinical variables (heart and respiratory rate, blood pressure, etc.) and usual biological values (as determined by the accredited Laboratory of the Service of Biomedicine of the CHUV) were extracted from the computerized information system (Metavision, iMDsoft, Israel). C-reactive protein (CRP) levels were measured using the Tina-quant® CRP method on a Modular P apparatus (Roche Diagnostics, Mannheim, Germany). Severity of illness was evaluated on the first ICU day using the Simplified Acute Physiology Score (SAPS) II [11] and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score [12]. Organ dysfunction at 24 h was evaluated by the Sepsis-related Organ Failure Assessment (SOFA) score [13].
Definitions and types of infection
We define sepsis, severe sepsis, and septic shock according to criteria proposed by the 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference [14]. Community-acquired infection was defined as an infection manifesting before or within 48 h after hospital admission, whereas nosocomial infection was defined as an infection occurring at least 48 h after hospital admission. Nosocomial and healthcare-associated pneumonia were excluded. Patients with concomitant pneumococcal meningitis, invasive ENT infections, or endocarditis were not included. Microbiologically documented, severe CAP infections caused by S. pneumoniae were diagnosed according to the adapted American Thoracic Society definition [15].
Statistical analysis
Continuous variables are reported as the mean and standard deviation (SD) or as medians and interquartile ranges (IQR) as indicated. Categorical variables are reported as frequencies. APACHE II, SAPS II, and SOFA scores are expressed as medians and IQR. Comparison of continuous variables between survivors and nonsurvivors was carried out using the Student’s t test for parametric values, and the Mann–Whitney U test for nonparametric values. Fisher’s exact test was used to compare categorical variables.
We assessed the independent predictors of hospital mortality at the time of admission and 24 h after admission with logistic regression models in which we included all variables with a P value ≤0.1 from the univariate analysis. Severity scores are computed after 24 h in the ICU, so they were not included in the models assessing the predictors of hospital mortality at time of admission. Age and gender were included in all models as clinically relevant variables for mortality, excepted for models containing severity scores; indeed the variable age is already used to compute those scores. Given the potential impact of frailer elderly patients, we completed the statistical analysis with age as a categorical variable (age group >65 years vs ≤65 years).
We assessed the discriminative ability of CRP to predict mortality by computing its receiver operating characteristic (ROC) curve. The cut-off for the best sensitivity and specificity was derived from the curve coordinates. The area under the curve (AUC) was reported with 95 % confidence intervals (CI 95 %), as well as the P value for the difference with the reference line.
A two-sided P value <0.05 was considered statistically significant. We used the statistical software SPSS (version 19, IBM Company, USA) for data processing and analyses.
Results
Patient characteristics
From January 2002 to December 2011, 22,226 patients were admitted to the 32-bed medico-surgical ICU. Among them, 84 presented with invasive S. pneumoniae infections, including 77 patients with severe CAP and seven with meningitis.
Outcomes
Among the 77 patients with severe S. pneumoniae CAP requiring ICU management, 12 patients died (15.6 %) (Table 1). Compared to the mortality predicted by the APACHE II scores (32.2 %) and the SAPS II (39.2 %), we observed a lower hospital mortality rate (15.6 %). This trend hold true for elderly >65 years (22.2 %). This corresponded to a standardized mortality ratio (SMR) of 0.48 and 0.40 for APACHE II and SAPS II, respectively. Comorbidity was present in a high proportion of patients, but we did not observe any correlation between comorbidity and the outcome.
The microbiological characteristics, the severity of the infection, and the supportive measures required to treat the patients are presented in Table 2. Septic shock, APACHE II score, SAPS II, SOFA score at 24 h, and the presence of multiple organ failure were correlated with a fatal outcome. In contrast, successful noninvasive ventilation and a high initial CRP value were correlated with survival.
Pneumococcal coverage was adequate in all patients (Table 1). Among initial treatment, combined antibiotics were given in 45 (69 %) of survivors and in 11 (92 %) of non-survivors (P = 0.163).
Outcome prediction at 24 h after admission
In the multivariate analysis, the APACHE II (OR 1.13, CI 95 % 1.02–1.25; P = 0.021), SAPS II (OR 1.06, CI 95 % 1.01–1.11, P = 0.024), and SOFA (OR 1.54, CI 95 % 1.16–2.05, P = 0.003) severity scores at 24 h predicted death. Each score was included in a separate multivariate logistic regression model adjusted for gender, CRP and septic shock, adding age in the analysis with SOFA. When age is included, as a categorical variable (age group >65 vs ≤65), SOFA (OR 1.6; CI 95 % 1.18–2.23, P = 0.030) remained significant to predict mortality.
Outcome prediction at time of admission
Severity scores include the worst values of a high number of physiological variables and can only be computed after 24 h, so they were not included in this analysis. After adjustment for age and gender, septic shock (OR 4.96; CI 95 % 1.11–22.25, P = 0.036) and a low CRP value (OR 0.99; CI 95 % 0.98–099, P = 0.034) predicted death. When age was included as categorical variable (age >65 vs ≤65), septic shock (OR 5.42; CI 95 % 1.18–24.9, P = 0.030), and a low CRP value (OR 0.99; CI 95 % 0.98–099, P = 0.023) remained significant.
Procalcitonin (PCT)
Among the 20 patients (26 %) for whom PCT measurements within 24 h of admission were available, the median PCT value was 20.8 ng/ml (IQ: 4.4–40.4). No statistical difference was found between survivors (14 patients, median 7.4 ng/ml (IQR: 3.5–55.1) and non-survivors (6 patients, median 36.5 ng/ml (IQR 16.3–40.4) (P = 0.35; Mann–Whitney).
CRP
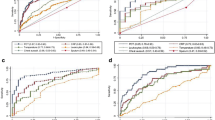
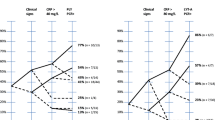
Two-thirds of the patients who died (8 of 12) presented with CRP lower third, with values below 158 mg/L, (Fig. 1). Three quarters of these eight patients (6 of 8) presented with CRP values below 133 mg/L. Table 3 presents patient’s characteristics according to CRP terciles. We assessed the discriminative ability of CRP to predict mortality by computing its ROC curve. The ROC curve of an admission CRP value <169.5 mg/L predicted mortality with a sensitivity of 75 %, a specificity of 72 % (1–0.277), a positive predictive value of 33 %, and a negative predictive value of 94 %. The AUC was 0.72 (CI 95 % 0.55–0.89, P = 0.018) (Fig. 2).

CRP levels among patients with fatal outcomes. Proportion of patients who died according to terciles of CRP levels. Two-thirds of the patients who died (8 of 12) presented with a CRP level below 158 mg/L. Of these eight patients, three quarters (6 of 8) had a CRP value below 133 mg/L

Accuracy of CRP in outcome prediction. ROC curve of CRP levels in the prediction of hospital mortality. The AUC for a CRP value <169.5 mg/L is 0.716 (0.547–0.886)
Discussion
CAP caused by S. pneumoniae has a large burden and is associated with high mortality [10, 16]. Interestingly, we report a lower than expected mortality in our cohort of CAP patients with S. pneumoniae infections requiring ICU management. Indeed, trends toward decreased mortality rates of severe sepsis patients were recently reported by others [17]. These lowered mortality rates may be accounted for by implementation of aggressive management of severe infections over the last decade, as recommended by international guidelines [18].
As with other types of severe infections, the shock and severity scores assessed at 24 h also predicted death in our cohort. Interestingly, our data showed that among patients with CAP caused by S. pneumoniae that required ICU management, the presence of septic shock and a low initial serum CRP level at admission correlated with a fatal outcome. This finding is unexpected and counterintuitive. Most clinicians would consider a priori that low CRP values may be associated with a less severe systemic inflammation response, which should reflect a better prognosis. However, data from animal studies suggest an association between CRP values and survival. In mice, administration of CRP within a few hours of a S. pneumoniae challenge led to a reduction in the concentration of bacteria in the blood, and consecutively lessened the severity of the infection [19, 20]. Over the study period, PCT values were only available for a small number of patients, precluding any conclusion about the absence of difference between survivors and non-survivors.
Several aspects may limit the interpretation of our data. We retrospectively analyzed a small cohort of patients admitted over one decade. Nevertheless, these patients can be considered as a homogenous cohort of severely ill patients requiring ICU management in an institution where the ratio between ICU and intermediate care beds is 1–3. The absences of electronic or computerized documentation of care preclude analyzing the impact of delay between hospital admission and first antibiotic administration on patient outcome. However, community-acquired pneumonia is characterized by an undefined and highly variable time between onset of the disease, clinical manifestations, and hospital admission. As such, the precise interval of time between onset of the disease and the first antibiotic administration is hard to determine, although highly relevant. This observation is only valid in the specific stetting of patients with severe pneumonia requiring ICU management. Our results should be considered as preliminary, but should be of sufficient interest to justify confirmation in larger cohorts of patients.
An eventual confirmation of a significant correlation between low initial CRP values and fatal outcomes may be used to stratify patients with severe CAP caused by S. pneumoniae. Indeed, progressive ICU shortages (e.g., ICU-related costs, shortages of ICU physician, and nurses) may be responsible for the early ICU discharge of patients that are perceived to be at low risk of death, such as those with severe infection and a good perceived prognosis.
Conclusion
Since CRP values are almost universally available within a few hours of ICU admission, they may help to stratify patients with severe CAP due to S. pneumoniae according to their prognoses and to tailor their management accordingly.
References
File TM Jr. Streptococcus pneumoniae and community-acquired pneumonia: a cause for concern. Am J Med. 2004;117:39S–50S.
File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122:130–41.
Shah SS, Ratner AJ. Trends in invasive pneumococcal disease-associated hospitalizations. Clin Infect Dis. 2006;42:e1–5.
Rodriguez A, Lisboa T, Blot S, Martin-Loeches I, Solé-Violan J, De Mendoza D, Rello J, Community-Acquired Pneumonia Intensive Care Units (CAPUCI) Study Investigators. Mortality in ICU patients with bacterial community-acquired pneumonia: when antibiotics are not enough. Intensive Care Med. 2009;35:430–8.
Moine P, Vercken JB, Chevret S, Gajdos P. Severe community-acquired pneumococcal pneumonia. The French Study Group of Community-Acquired Pneumonia in ICU. Scand J Infect Dis. 1995;27:201–6.
Georges H, Leroy O, Vandenbussche C, Guery B, Alfandari S, Tronchon L, Beaucaire G. Epidemiological features and prognosis of severe community-acquired pneumococcal pneumonia. Intensive Care Med. 1999;25:198–206.
Walden AP, Clarke GM, McKechnie S, Hutton P, Gordon AC, Rello J, Chiche JD, Stueber F, Garrard CS, Hinds CJ, ESICM/ECCRN GenOSept Investigators. Patients with community acquired pneumonia admitted to European Intensive Care Units: an epidemiological survey of the GenOSept cohort. Crit Care. 2014;18:R58.
CDC Pneumococcal Disease. Epidemiology and prevention of vaccine-preventable diseases. 12th ed. Atlanta: CDC; 2012. p. 233–48.
Cillóniz C, Ewig S, Polverino E, Muñoz-Almagro C, Marco F, Gabarrús A, Menéndez R, Mensa J, Torres A. Pulmonary complications of pneumococcal community-acquired pneumonia: incidence, predictors, and outcomes. Clin Microbiol Infect. 2012;18:1134–42.
Mongardon N, Max A, Bouglé A, Pène F, Lemiale V, Charpentier J, Cariou A, Chiche JD, Bedos JP, Mira JP. Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive care unit: a multicenter study. Crit Care. 2012;16:R155.
Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270:2957–63.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA(Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–10.
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003;29:530–8.
Brown SM, Jones BE, Jephson AR, Dean NC, Infectious Disease Society of America/American Thoracic S. Validation of the Infectious Disease Society of America/American Thoracic Society 2007 guidelines for severe community-acquired pneumonia. Crit Care Med. 2009;37:3010–106.
Rolo D, Fenoll A, Fontanals D, Larrosa N, Giménez M, Grau I, Pallarés R, Liñares J, Ardanuy C, Serotype 5 Study Group. Serotype 5 pneumococci causing invasive pneumococcal disease outbreaks in Barcelona, Spain (1997 to 2011). J Clin Microbiol. 2013;51:3585–90.
Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311:1308–16.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent JL, Moreno R, Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39:165–228.
Suresh MV, Singh SK, Ferguson DA Jr, Agrawal A. Human C-reactive protein protects mice from Streptococcus pneumoniae infection without binding to pneumococcal C-polysaccharide. J Immunol. 2007;178:1158–63.
Agrawal A, Suresh MV, Singh SK, Ferguson DA Jr. The protective function of human C-reactive protein in mouse models of Streptococcus pneumoniae infection. Endocr Metab Immune Disord Drug Targets. 2008;8:231–7.
Acknowledgments
We thank Laurence Leone for outstanding technical assistance. This study was funded by an unrestricted grant from the “Loterie Romande” and the “Fondation pour la Recherche en Soins Intensifs.” YAQ is supported by the Swiss National Science Foundation (SNF)/Swiss Medical Association (FMH) grant #PASMP3-123226 and a grant from the SICPA Foundation.
Conflict of interest
All authors declare no potential conflicts of interest regarding their contribution to this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
E. Charbonney and P. Eggimann contributed equally to the work.
Rights and permissions
About this article

Cite this article
Que, YA., Virgini, V., Lozeron, E.D. et al. Low C-reactive protein values at admission predict mortality in patients with severe community-acquired pneumonia caused by Streptococcus pneumoniae that require intensive care management. Infection 43, 193–199 (2015). https://doi.org/10.1007/s15010-015-0755-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-015-0755-0