
Abstract
Purpose
Tuberculous pleural effusion (TPE) is characterized by lymphocytic predominance and high adenosine deaminase (ADA) levels. However, TPEs sometimes present non-lymphocytic predominance, and parapneumonic effusion (PPE) often exceeds the cutoff value of ADA for TPE. Thus, the differential diagnosis of cases with pleural fluid (PF) showing non-lymphocytic predominance and high ADA levels is challenging. However, limited data concerning the clinical differences in these patients are available.
Methods
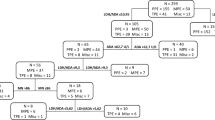
A retrospective study was conducted on TPE and PPE patients with PF showing non-lymphocytic predominance and ADA levels ≥40 U/L in 2009–2013 in a South Korean tertiary referral hospital. The clinical, laboratory, and computed tomography (CT) findings between the groups were analyzed using multivariate logistic regression to develop a prediction model with independent factors for TPE.
Results
Among 353 patients with TPE, 24 (6.8 %) showed PF with non-lymphocytic predominance and ADA levels of ≥40 U/L. Twenty-eight PPE patients who presented PF findings comparable with those of TPE patients were included in the control group. In the final analysis, PF ADA levels >58 U/L and nodular lung lesions on CT were independent positive predictors, while loculated effusion was an independent negative predictor for TPE. Using the prediction model, a score ≥ +3 provided a sensitivity of 88 %, specificity of 93 %, positive predictive value of 91 %, and negative predictive value of 90 % for TPE.
Conclusion
PF ADA levels, nodular lung lesions, and loculated pleural effusion may help differentiate TPE from PPE in patients with PF showing non-lymphocytic predominance and ADA levels ≥40 U/L.

Similar content being viewed by others


References
Krenke R, Korczynski P. Use of pleural fluid levels of adenosine deaminase and interferon gamma in the diagnosis of tuberculous pleuritis. Curr Opin Pulm Med. 2010;16:367–75.
Liang QL, Shi HZ, Wang K, et al. Diagnostic accuracy of adenosine deaminase in tuberculous pleurisy: a meta-analysis. Respir Med. 2008;102:744–54.
Porcel JM. Tuberculous pleural effusion. Lung. 2009;187:263–70.
Levine H, Szanto PB, Cugell DW. Tuberculous pleurisy. An acute illness. Arch Intern Med. 1968;122:329–32.
Gopi A, Madhavan SM, Sharma SK, et al. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest. 2007;131:880–9.
Lin MT, Wang JY, Yu CJ, et al. Mycobacterium tuberculosis and polymorphonuclear pleural effusion: incidence and clinical pointers. Respir Med. 2009;103:820–6.
Porcel JM, Esquerda A, Bielsa S. Diagnostic performance of adenosine deaminase activity in pleural fluid: a single-center experience with over 2100 consecutive patients. Eur J Intern Med. 2010;21:419–23.
Sahn SA, Huggins JT, San Jose ME, et al. Can tuberculous pleural effusions be diagnosed by pleural fluid analysis alone? Int J Tuberc Lung Dis. 2013;17:787–93.
Light RW. Pleural disease. 3rd ed. Baltimore: Williams and Wilkins; 1995. Chapter 9. Parapneumonic effusions and empyema. p. 129–53.
World Health Organization. Tuberculosis. Available at: http://www.who.int./tb. WHO report. 2012.
Bielsa S, Palma R, Pardina M, et al. Comparison of polymorphonuclear- and lymphocyte-rich tuberculous pleural effusions. Int J Tuberc Lung Dis. 2013;17:85–9.
Lee J, Lee SY, Yoo SS, et al. Clinical value of whole-blood interferon-gamma assay in patients with suspected pulmonary tuberculosis and AFB smear- and polymerase chain reaction-negative bronchial aspirates. Diagn Microbiol Infect Dis. 2012;73:252–6.
Kim HJ, Lee HJ, Kwon SY, et al. The prevalence of pulmonary parenchymal tuberculosis in patients with tuberculous pleuritis. Chest. 2006;129:1253–8.
Maji A, Maikap MK, Jash D, et al. Role of common investigations in aetiological evaluation of exudative pleural effusions. J Clin Diagn Res. 2013;7:2223–6.
Valdes L, San Jose E, Alvarez D, et al. Diagnosis of tuberculous pleurisy using the biologic parameters adenosine deaminase, lysozyme, and interferon gamma. Chest. 1993;103:458–65.
Ocana I, Martinez-Vazquez JM, Segura RM, et al. Adenosine deaminase in pleural fluids. Test for diagnosis of tuberculous pleural effusion. Chest. 1983;84:51–3.
Lee J, Lee SY, Choi KJ, et al. Clinical utility of CT-based bronchial aspirate TB-PCR for the rapid diagnosis of pleural tuberculosis. Tuberc Respir Dis (Seoul). 2013;75:150–6.
Im JG, Itoh H, Shim YS, et al. Pulmonary tuberculosis: CT findings–early active disease and sequential change with antituberculous therapy. Radiology. 1993;186:653–60.
Hatipoglu ON, Osma E, Manisali M, et al. High resolution computed tomographic findings in pulmonary tuberculosis. Thorax. 1996;51:397–402.
Wang YH, Lin AS, Lai YF, et al. The high value of high-resolution computed tomography in predicting the activity of pulmonary tuberculosis. Int J Tuberc Lung Dis. 2003;7:563–8.
Lee HM, Shin JW, Kim JY, et al. HRCT and whole-blood interferon-gamma assay for the rapid diagnosis of smear-negative pulmonary tuberculosis. Respiration. 2010;79:454–60.
Kim CH, Lim JK, Lee SY, et al. Predictive factors for tuberculosis in patients with a TB-PCR negative bronchial aspirate. Infection. 2013;41:187–94.
Kwon JS, Cha SI, Jeon KN, et al. Factors influencing residual pleural opacity in tuberculous pleural effusion. J Korean Med Sci. 2008;23:616–20.
Han DH, Song JW, Chung HS, et al. Resolution of residual pleural disease according to time course in tuberculous pleurisy during and after the termination of antituberculosis medication. Chest. 2005;128:3240–5.
Cases Viedma E, Lorenzo Dus MJ, Gonzalez-Molina A, et al. A study of loculated tuberculous pleural effusions treated with intrapleural urokinase. Respir Med. 2006;100:2037–42.
Muller NL. Imaging of the pleura. Radiology. 1993;186:297–309.
Valdes L, Alvarez D, San Jose E, et al. Tuberculous pleurisy: a study of 254 patients. Arch Intern Med. 1998;158:2017–21.
Conflict of interest
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, J., Lee, S.Y., Lim, J.K. et al. Radiologic and laboratory differences in patients with tuberculous and parapneumonic pleural effusions showing non-lymphocytic predominance and high adenosine deaminase levels. Infection 43, 65–71 (2015). https://doi.org/10.1007/s15010-014-0697-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-014-0697-y