
Abstract
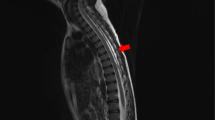
Ureterosigmoidostomy is a urological intervention performed to treat various conditions such as invasive bladder cancer, bladder exstrophy, vesicovaginal fistula, or urethral trauma. However, this intervention may lead to several metabolic complications. Here, we report an interesting case with quadriparesis and intestinal paralysis resulting from severe hypokalemia (the serum potassium level, 1.8 mEq/L) and hyperchloremic metabolic acidosis [pH 6.927 and the arterial bicarbonate level, 8.0 mEq/L] in a 65-year-old man who had undergone bilateral ureterosigmoidostomy for bladder cancer 16 years earlier. The abdominal computed tomography scan also showed that massive fluid consisting of the mixture of the diverted urinary stream and feces was accumulated in the dilated distal colon. The treatment with intravenous potassium and sodium bicarbonate administration combined with the drainage of the diverted urinary stream from the distal colon resulted in the restoration of hypokalemia and acidosis followed by the improvement of quadriparesis and intestinal paralysis. The underlying mechanism and the treatment of metabolic complications after ureterosigmoidostomy are briefly discussed.


Similar content being viewed by others


References
Creevy CD. Facts about uretero-sigmoidostomy. J Am Med Assoc. 1953;151:120–3.
Loughlin JF. Quadriplegia, hypopotassemia, and hyperchloremic acidosis after bilateral ureterosigmoidostomy. N Engl J Med. 1956;254:329–32.
Van Bekkum JW, Bac DJ, Nienhuis IE, De Leeuw PW, Dees A. Life-threatening hypokalaemia and quadriparesis in a patient with ureterosigmoidostomy. Neth J Med. 2002;60:26–8.
Berilgen MS, Mungen B, Yakinci C, Bulut S. Ureterosygmoidostomy-associated hypokalemia-induced quadriparesis and rhabdomyolysis. Pediatr Int. 2005;47:341–2.
Rafique M. Life threatening hypokalemia and quadriparesis in a patient with ureterosigmoidostomy. Int Urol Nephrol. 2006;38:453–6.
Ozmen S, Danis R, Akin D, Gullu N, Ozmen CA, Yazanel O. Ureterosigmoidostomy-associated quadriparesis, non-traumatic rhabdomyolysis, and tetany in an adult. Int Urol Nephrol. 2008;40:245–7.
Fichtner J. Follow-up after urinary diversion. Urol Int. 1999;63:40–5.
Kunzelmann K, Mall M. Electrolyte transport in the mammalian colon: mechanisms and implications for disease. Physiol Rev. 2002;82:245–89.
Boyd JD. Chronic acidosis secondary to ureteral transplantation. Am J Dis Child. 1931;42:366–71.
Narins RG, Krishna GG, Bressler L, Stom MC, Goodkin D, Shay R, Townsend R. The metabolic acidosis. In: Maxwell MH, Kleeman CR, Narins RG, editors. Clinical disorders of fluid and electrolyte metabolism. New York: McGraw-Hill; 1987. p. 597–642.
Acknowledgments
We thank American Journal Experts (http://www.aje.com) for the careful reading and preparation of our manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
About this article

Cite this article
Niwa, H., Fukasawa, H., Kaneko, M. et al. Hypokalemia-associated paralysis and metabolic acidosis in a patient with bilateral ureterosigmoidostomy. CEN Case Rep 5, 40–42 (2016). https://doi.org/10.1007/s13730-015-0187-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-015-0187-9