
Abstract
Evidence from the past decades strongly suggests that diabetes and depression are associated. Approximately 10–15 % of patients with diabetes meet criteria for comorbid depression. This study is designed to assess the level of depression among type 2 diabetic patients without any complications and type 2 diabetic patients who developed more than two complications due to diabetes. A total of 204 (M:F 138:66) subjects were included in this cross-sectional study. Levels of depressive symptoms were measured using the centre for Epidemiologic Studies Depression scale (CED-D). Considering degree of depression, 74.3 vs. 97.1 % of male had moderate depression (λ 2 = 12.6, p < 0.0001). In female group, 84.4 vs. 97.1 % of them had moderate depression (λ 2 = 1.96, p = 0.162). There was no statistical significant difference noted among gender (p = 0.371). People with diabetes have mild/moderate depressive symptoms which can be better said as “Diabetic distress rather depression” irrespective of the presence of diabetic complications. The role of a psychologist here is more on education, reorienting and reconciliation.
Similar content being viewed by others


Introduction
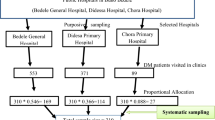
Depression is most common among people with acute/chronic illness. Diabetes is a disorder, needs consistent care and management, which may often frustrate people. Evidence from the past decades suggests that diabetes and depression are associated. Approximately, 10–15 % of patients with diabetes meet the criteria for comorbid major depression. There is an increasing evidence that significant additional functional, fiscal and psychological costs are associated with depression in patients with diabetes [1]. Moreover, depression also contributes to poor self-care and adherence to medical treatment, higher symptom burden, higher glycated haemoglobin (HbA1c), more diabetes complications and increased health-care use and costs in patients with diabetes [2]. A study reported that non-diabetic adults with depression have 30 % increased risk for development of type 2 diabetes [3]. This study is designed to assess the level of depression among two groups of subjects consisted of type 2 diabetic patients without any complications and type 2 diabetic patients who developed more than two complications due to diabetes (Fig. 1).

Comparison of degree of depression gender wise. Considering degree of depression, 74.3 vs. 97.1 % of male had moderate depression (λ 2 = 12.6, p < 0.0001). In female group, 84.4 vs. 97.1 % of them had moderate depression (λ 2 = 1.96, p = 0.162). There was no statistical significant difference noted among gender (p = 0.371)
Subjects and methods
A total of 204 (M:F 138:66), who visited the outpatient department at M.V. Hospital for Diabetes, Royapuram, Chennai, were included in this cross-sectional study. All these attendees were explained about the study and whoever gave consent voluntarily have been considered for the study. Self identities of the participants were protected to maintain confidentiality.
Details on sociodemographic, education status, occupation and personal habits were collected. A structured interview was conducted to assess the levels of depressive symptoms using the Centre for Epidemiologic Studies Depression scale (CES-D). A score of less than 15 indicates no depression, 15–21 indicates mild/moderate depression and above 21 possibility of major depression.
All data were entered using double-entry system into a spreadsheet and reviewed for accuracy prior to analysis. Qualitative information was thematically analyzed.
Prof M. Viswanthan Diabetes Research centre’s committee provided the approval for this study.
Patients were grouped as group 1—type 2 diabetic patients without any complication (n = 101, M:F 70:31; and group 2—type 2 diabetic patients with presence of more than two diabetic complications either micro- or macro-vascular complications (n = 103, M:F 68:35).
Results
A total of 204 subjects (M:F 138:66) with mean age of 48.65 ± 12.5 participated. Table 1 shows demographic details; 57.2 % of male vs. 43.9 % of females had completed their schooling, 28 % of male vs. 22.7 % of females were graduates, 8.7 % of males vs. 12.1 % of females were post graduates and 5.1 % of males vs. 4.5 % of females are professionals. Twenty-eight percent of males vs. 22.7 % of females were in private jobs, 29 % of males and 4.5 % of females owned business, 25.8 % of females vs. 15.9 % males were professionals, 25 % of males were retired and 47 % of females were homemakers; 88.4 % of males and 74.2 % of females were married, 6.5 % of males vs. 15.2 % of females were unmarried, 0.7 % of males and 1.5 % of females were divorced and 4.3% of males vs. 9.1 % of females were widow(er)s.
Non-vegetarians were 81.2 % of males vs. 87.9 % of females and 18.8 % of males vs. 12.1 % of females were vegetarians. Ninety-four percent of females do not use alcohol/tobacco, whereas 10.9 % of men were alcoholics, 7.2 % use tobacco, 7.2 % use both alcohol and tobacco, 6.5 % were smokers, 1.4 % use alcohol and smokeless tobacco and 5.8 % were drug users. Eighty-three percent of males and 73 % of females have stress related to work and family.
The mean degree of depression score in group 1 was 16.8 ± 12.9 (SD) and in group 2 was 15.11 ± 13.3 (SD) (p = 0.372). Considering the degree of depression, 74.3 % of male had moderate depression in the group without complications, whereas 97.1 % of male had moderate depression in the group with complication (λ 2 = 12.6, p < 0.0001). In female group, 84.4 % of them had moderate depression among the group without complications and 97.1 % of female had moderate depression in the group with complications (λ 2 = 1.96, p = 0.162). There was no statistical significant difference noted among gender (p = 0.371).
Discussion
People with diabetes have double the odds of having depression too. Approximately 10–15 % of patients with diabetes meet the criteria for comorbid depression [4]. CURES study from our city has showed significant association between depression and various diabetes complications [5]. But our study shows that majority (above 75 %) of the respondents fall under mild/moderate depression, which can be termed as “Diabetic distress rather depression”. Frustrations can stem from common occurrences such as running out of cost for diabetes treatment and medication, frequent fluctuations in blood sugar levels, stress related to work and life events [6]. Our study also revealed that it is difficult and exhausting to balance the family, work and diabetes self-care regimen, which causes diabetes distress. This may be due to the difference in sample size. However, further research is needed to clarify underlying reasons.
Though several literatures state that depression is higher in women compared to men, our study does not have any significant difference among gender. The confounders were not looked in as the sample size is minimal.
Our study shows depression is more severe in female subjects without diabetes complication in comparison to the subjects with diabetic complication. When looking out for factors, we understood that subjects with comorbid complications have diabetic for more than 5 years. The repetitive counselling sessions by health-care providers have developed pro-coping abilities among them, whereas the group without any comorbid complication were having diabetes less than 5 years. Moreover, they are anxious that they should not develop comorbid complications.
Conclusion
People with diabetes have mild/moderate depressive symptoms irrespective of the presence of diabetic complications. The role of a psychologist here is more on education, reorienting and reconciliation. The counsellor has to measure the psychological outcomes and processes, which will help in understanding the clients, pro-diabetic coping behaviours like diet and exercise, health risk behaviour like smoking and alcohol and client’s attitude towards problem solving, clinical distress management and conflict and resolution management. Facilitating people with diabetes for better coping skills and stress management will help them successfully overcome distress and deal with depression and diabetes.
References
de Groot M, Michael K, Todd D, Jennifer M, Mark MG, Jay S, et al. Depression among adults with diabetes: prevalence, impact, and treatment options. Diabetes Spectrum. 2010;23(1):15–8.
Adriaanse MC, Dekker JM, Spijkerman AM, et al. Diabetes-related symptoms and negative mood in participants of a targeted population-screening program for type 2 diabetes: the Hoorn screening study. Qual Life Res. 2005;14:1501–9.
Knol MJ, Twisk JW, Beekman AT, Heine RJ, Snoek FJ, Pouwer F. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia. 2006;49(5):837–45.
Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes. Diabetes Care. 2001;24:1069–78.
Poongothai S, Anjana RM, Pradeepa R, Ganesan A, Ranjit U, Rema M, Mohan V. Association of Depression with complication of Type 2 Diabetes (CURES – 102). JAPI, 2011 October, Vol.59.
Joe S. Diabetes and depression: some thoughts to think about. Diabetes Spectrum. 2010;23(1):11–5.
Acknowledgments
The researchers sincerely thank Ms. Dhanalakshmi for her assistance in the manuscript writing. We sincerely thank the entire respondents for their time and support.
Conflicts of interest
None
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article

Cite this article
Shaji, S., Elayaraja, B., Kumpatla, S. et al. Assessment of depression among type 2 diabetic patients with complications and without complications. Int J Diabetes Dev Ctries 35, 310–313 (2015). https://doi.org/10.1007/s13410-014-0265-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-014-0265-0